
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Intestinal obstruction due to primary ileocolic diffuse large B-cell lymphoma: A case report
Marina Alarcón Iranzo1*; Matías Gómez Calomarde1; Estefanía Zorraquino2; Miguel Ángel Sanz3; Roberto Lozoya Trujillo4; Maria Dolores Ruiz Carmona4; Amparo Solana Bueno4
1Department of General and Digestive Surgery, Hospital de Sagunto, Valencia, Spain.
2Department of Pathological Anatomy, Hospital de Sagunto, Valencia, Spain.
3Department of Hematology, Hospital de Sagunto, Valencia, Spain.
4Department of General and Digestive Surgery, Hospital de Sagunto, Valencia, Spain.
*Corresponding Author : Marina Alarcón Iranzo
Department of General and Digestive Surgery, Hospital de Sagunto. Servicio de Cirugía. Av. Ramon Y Cajal s/n 46520 Sagunto, Valencia, Spain.
Email: marina.alarcon.iranzo.88@gmail.com
Received : Apr 15, 2021
Accepted : May 11, 2021
Published : May 14, 2021
Archived : www.jcimcr.org
Copyright : © Iranzo MA (2021).
Abstract
The Gastrointestinal (GI) tract is the most frequent site of extranodal lymphoma involvement. Most GI lymphomas are non-Hodgkin’s mature B-cell lymphomas, being diffuse large B-cell lymphoma one of the most common histologic subtypes. About 7% of GI lymphomas are located in the colon, usually at the ileocecal valve, and may grow into the terminal ileum. Abdominal pain and weight loss are common presenting symptoms, although complications such as intestinal obstruction may occur. Abdominal CT scan and barium enema are the most frequently used imaging tests for diagnosis, although colonoscopy with biopsies is required to confirm the diagnosis. Treatment includes surgery and chemotherapy with or without rituximab.
Keywords: Primary colonic lymphoma; Diffuse large B-Cell Lymphoma; Obstruction; Surgery; Management.
Citation: Alarcón M, Gómez M, Zorraquino E, Sanz M, Lozoya R, et al. Intestinal obstruction due to primary ileocolicdiffuse large B-cell lymphoma: A case report. J Clin Images Med Case Rep. 2021; 2(3): 1145.
Case presentation
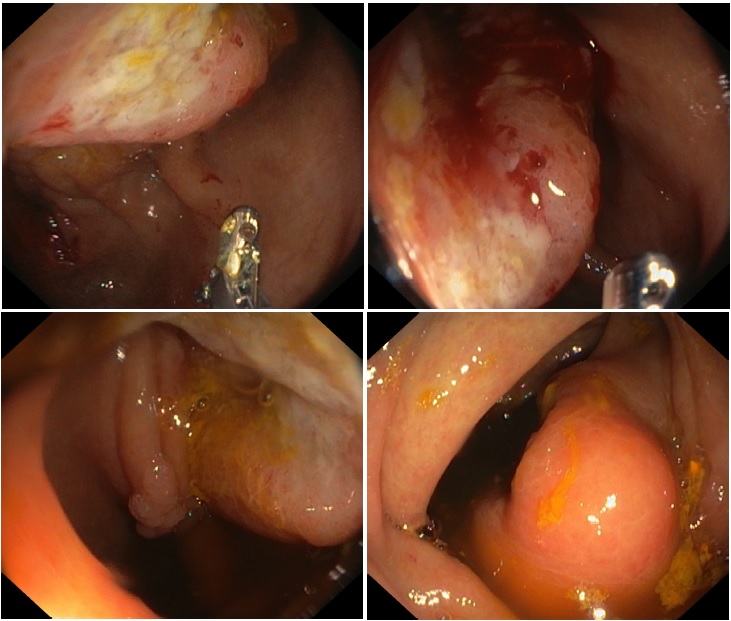
We present the case of an 86-year-old male patient who was being studied for asthenia, weight loss and anemia (Hb 6.2 g/dL). Physical examination revealed a palpable mass in the right iliac fossa. Laboratory tests showed iron deficiency anemia, with no other alterations. In the total body Computed Tomography (CT), asymmetric circumferential mural thickening of the cecum and terminal ileum was identified in a segment of approximately 14 cm, with neoplastic characteristics, associated with adenopathic conglomerate as well as small nodes in the Marina Alarcón Iranzo1*; Matías Gómez Calomarde1; Estefanía Zorraquino2; Miguel Ángel Sanz3; Roberto Lozoya Trujillo4; Maria Dolores Ruiz Carmona4; Amparo Solana Bueno4 1Department of General and Digestive Surgery, Hospital de Sagunto, Valencia, Spain. 2Department of Pathological Anatomy, Hospital de Sagunto, Valencia, Spain. 3Department of Hematology, Hospital de Sagunto, Valencia, Spain. 4Department of General and Digestive Surgery, Hospital de Sagunto, Valencia, Spain. root of the mesentery with engorgement of the mesenteric vessels. Colonoscopy (Figure 1) showed a mamelonated friable lesion on the ileocecal valve, with central depression, which caused partial stenosis of the valve and prevented the endoscope from passing through it. On biopsy, it was a hard lesion with en bloc displacement. The result of the first biopsy was inconclusive due to insufficient sample, so a new colonoscopy with biopsies was requested.
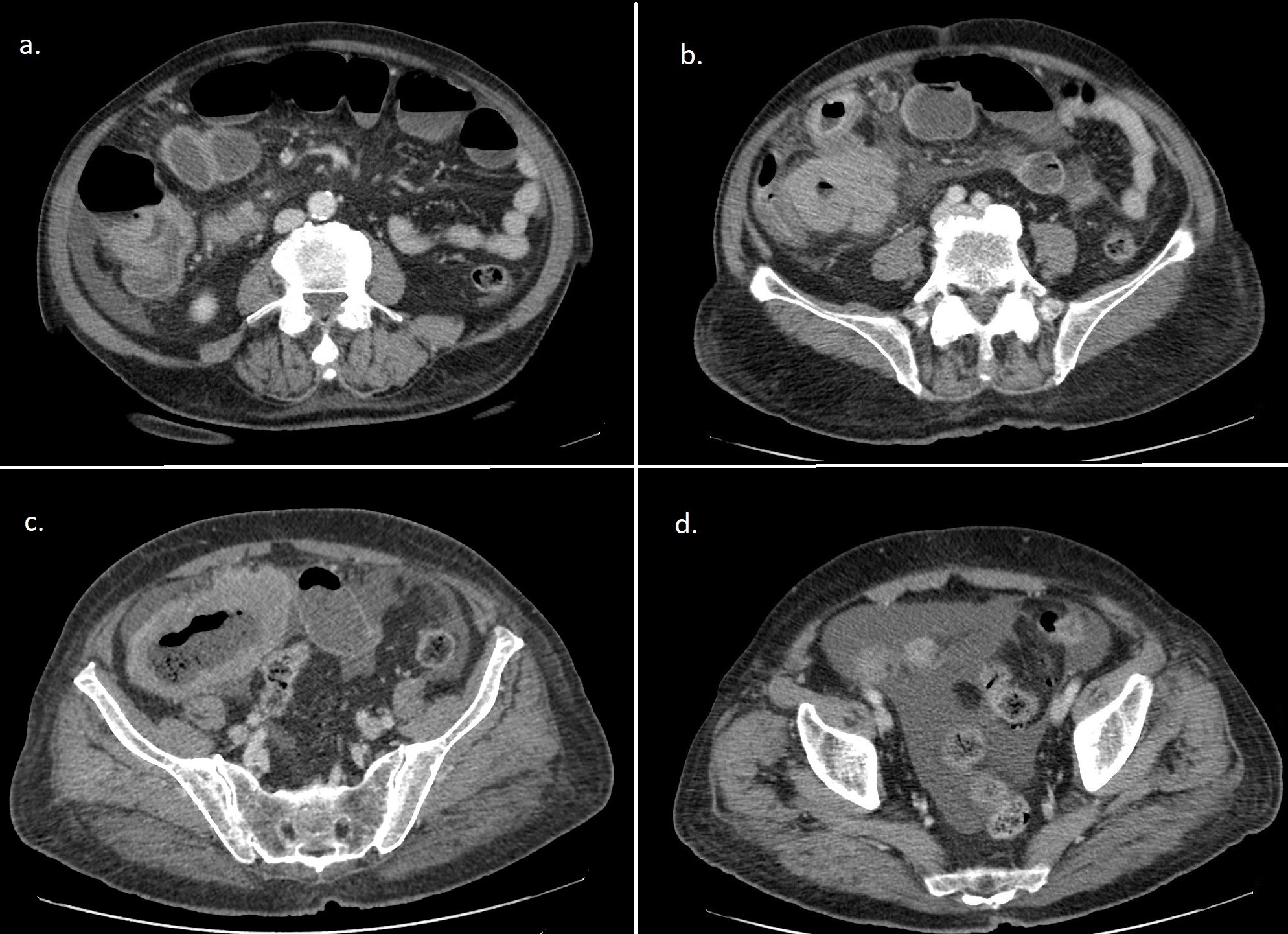
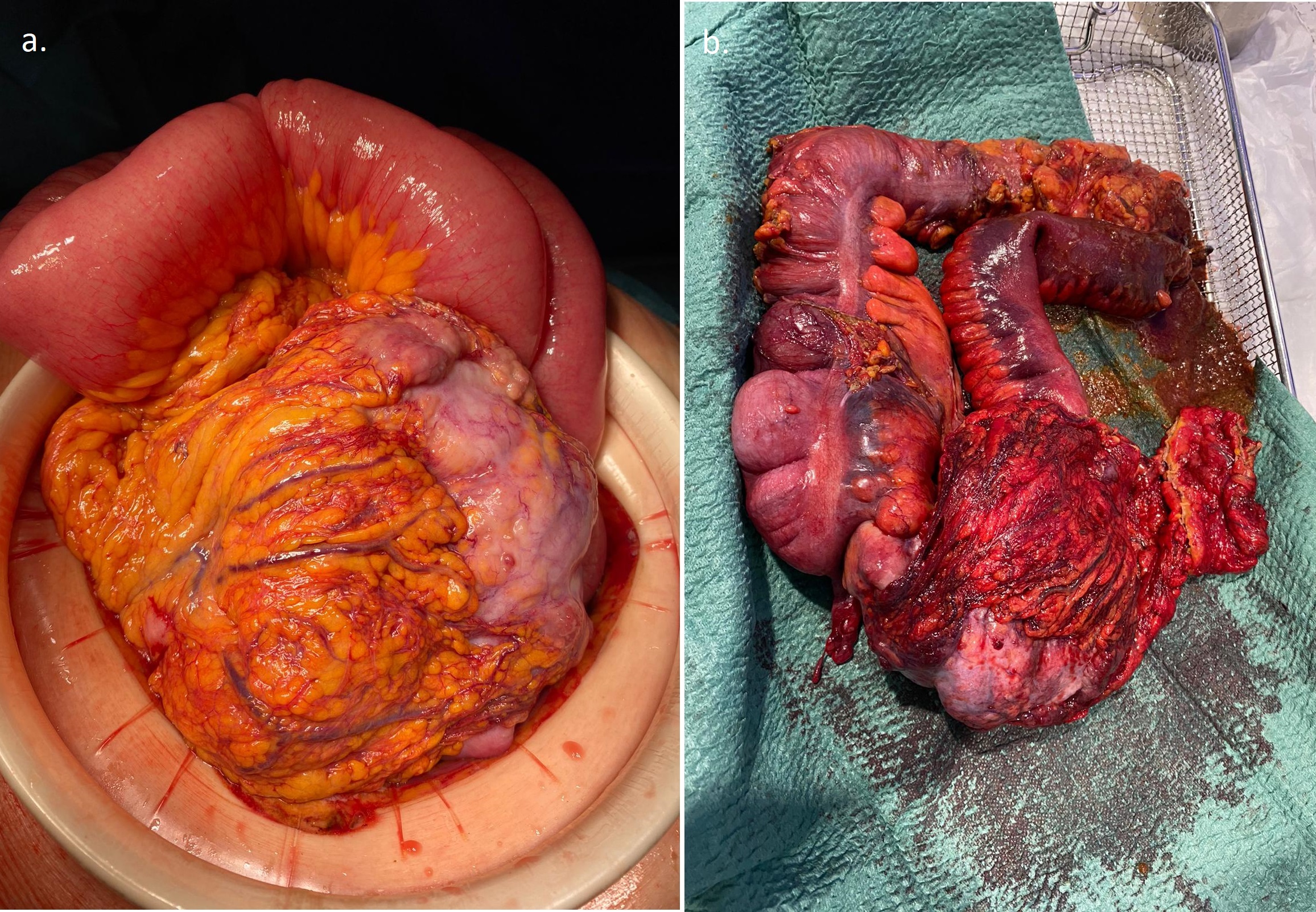
Five days after the second colonoscopy, the patient came to the Emergency Department reporting abdominal pain, vomiting and absence of intestinal transit of more than 72 hours. Laboratory tests showed leukocytosis with left shift and increased CRP. An abdominal X-ray showed dilatation of small bowel loops and an abdominopelvic CT scan (Figure 2) showed asymmetric and circumferential mural thickening of the cecum and terminal ileum, already known, which by the morphology of the aneurysmal dilatation of the lumen and the significant extent of involvement suggested probable lymphomatous etiology. As new findings in CT scan abundant amount of peritoneal ascites, greater parietal contrast uptake of the affected segment and retrograde dilatation of the ileum were identified, findings suggesting an incipient intestinal ischemic process. On suspicion of an intestinal occlusion due to neoplasia of the terminal ileum-ileocecal valve with onset of intestinal distress, the patient underwent an emergency exploratory lapatorotomy. During the intervention, a very voluminous neoplasm of the ileocecal valve extending to the terminal ileum with significant induration and mesenteric edema was observed, which caused retrograde dilatation of the small intestine with congestive loops of the terminal ileum and moderate diffuse peritoneal ascites. A right hemicolectomy with extended resection to the terminal ileum (Figure 3) was performed. The patient's postoperative course was satisfactory.
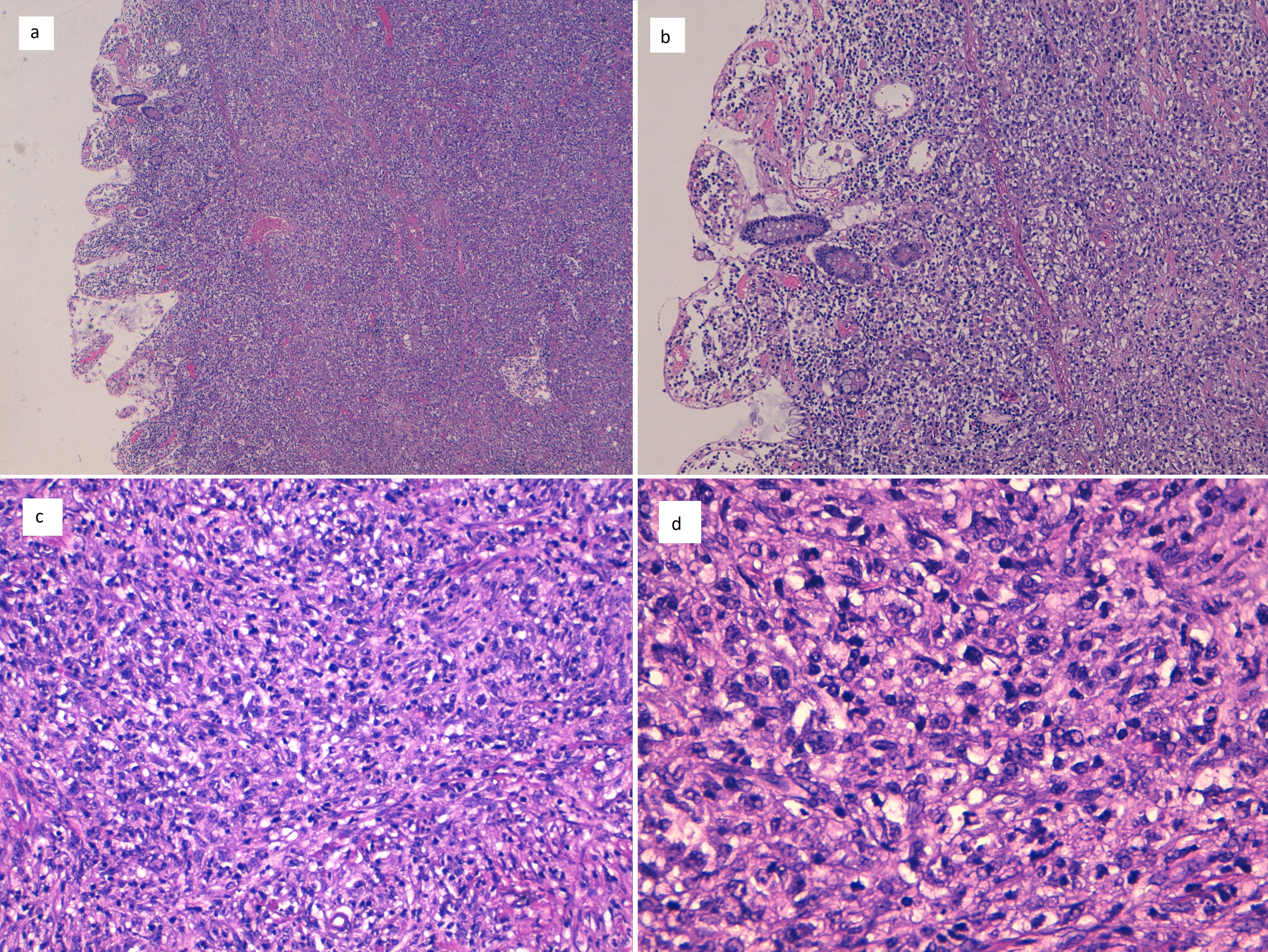
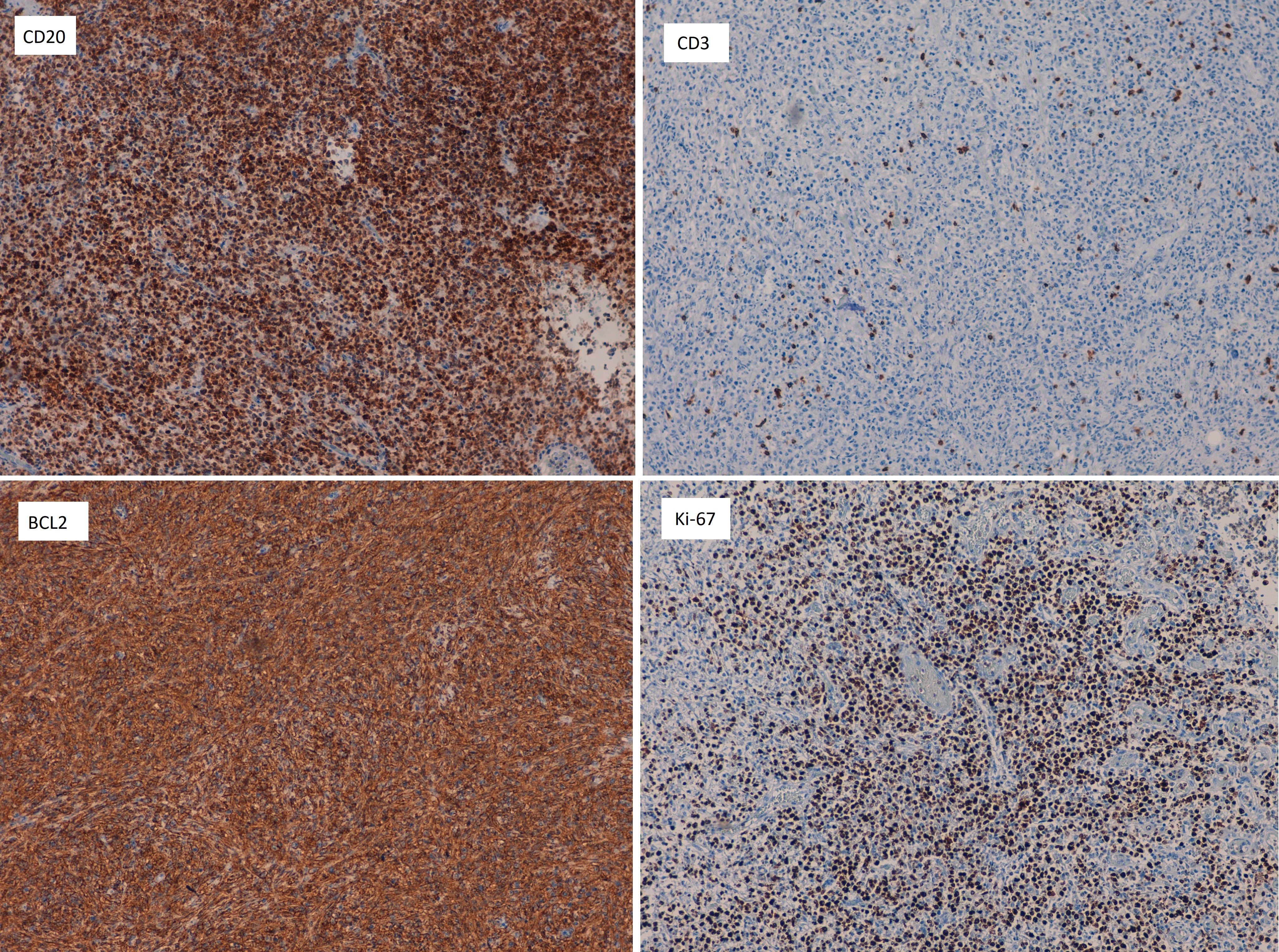
The specimen anatomopathological exam revealed a Diffuse Large Cell B-Cell Lymphoma (DLBCL) affecting the entire wall thickness of the cecum, ascending proximal colon and ileum, with a maximum dimension of 16.8 cm, with free surgical margins and two lymph node metastases. Histological study (Figure 4) showed a diffuse proliferation of large pleomorphic lymphocytes that infiltrate the entire thickness of the intestinal wall and obliterate the glandular architecture of the mucosa. The immunohistochemical study (Figure 5) was positive for CD20, Bcl-2, Bcl-6 and MUM1. Given this result, the patient was evaluated by hematologists. The study was completed with PET-CT, in which no hypermetabolic lesions were observed at the level of the terminal ileum, cecum or in other locations; bone marrow biopsy, which ruled out the presence of malignant lesions, and bone marrow aspirate, which showed normal cellularity with correct representation and maturation of the three hematopoietic series. Since this was a localized stage (T3N1M0B0 in the Paris TNMB staging system) with free surgical margins, treatment was completed with 3 cycles of rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) every 21 days.
Discussion
The Gastrointestinal (GI) tract is the most frequent site of extranodal lymphoma involvement. Most GI lymphomas are non-Hodgkin’s mature B-cell lymphomas, of which Mucosa-Associated Lymphoid Tissue (MALT) and DLBCL are the most common histologic subtypes [1,2]. The most frequent site of primary GI lymphomas is the stomach, where approximately 75% of lymphomas are located, followed by the small intestine (8.6%) and the colon (7%) [2,3]. Primary colonic lymphomas are rare and comprise about 0.2%-1.2% of all colonic malignancies. Colonic lymphomas are usually located near the ileocecal valve and grow into the terminal ileum [2-4], as seem to have ocurred in the present case.
Although the etiology is unknown, some risk factors described for colonic lymphoma are a history of previous lymphoma, previous treatments with radiotherapy or chemotherapy, immunosuppression, autoimmune diseases or some viral infections [5].
Clinical presentation of intestinal lymphomas is variable, being the abdominal pain the most common symptom (70%). Colonic lymphomas may also present with weight loss (43%) or an abdominal mass (29%) while small bowel lymphomas usually associate symptoms of ileus, weight loss, bleeding, perforation or palpable mass [1,2,4]. Our patient initially presented with weight loss, palpable mass and anemia (probably due to intestinal bleeding) and during the study was complicated by an intestinal obstruction that required emergent surgical treatment. The most common imaging studies performed for the study of colonic lymphomas are CT scan and barium enema [2], which can show different radiological patterns: Bulky polypoid masses (mainly located at ileocecal valve), local infiltrative tumors with wall thickening and aneurysmal dilatation [3]. However, it is necessary to make the differential diagnosis between lymphomas and adenocarcinomas of the colon, for which colonoscopy and biopsy are required. Other studies such as peripheral blood smear, bone marrow biopsy and PET-CT are indicated to rule out systemic involvement and to stage the disease. In our patient, all these studies excluded the presence of systemic disease [6]. Histologically, DLBCL is characterized by medium to large lymphoid cells containing large round, oval or slightly irregular nuclei with vesicular nuclear chromatin, prominent nucleoli and an ample amount of basophilic cytoplasm, and show a moderate to high proliferation index. In most cases, the predominant cells resemble large centroblasts or immunoblasts, although they may commonly coexist. DLBCL show positivity for BCL6 and are frequently CD10 and BCL2 positive [7].
Several different staging systems, such as Ann Arbor, Lugano or the Paris staging system, a modification of the Tumor, Node, Metastases (TNM) staging system for epithelial tumors, have been used to stage primary GI lymphoma. To date, there is no consensus regarding the best staging system for GI DLBCL. Some studies have evaluated the value of these three different staging systems in predicting clinical outcomes in patients with primary GI lymphoma. These studies reported a superiority of the Paris system in predicting overall survival in these patients [8,9]. Hwang et al demonstrated the relevance of the T parameter in the Paris staging system as a promising prognostic factor in resected intestinal DLBCL, but this prognostic significance was evidenced only in univariate analysis [8]. Therefore, further large-scale studies are needed to confirm these findings. In our patient, the Paris staging system was employed, showing a stage T3N1M0B0 after completing the surgery and the extension study.
Although there is no consensus on the optimal treatment of gastrointestinal DLBCL, the most widely accepted management option is surgical resection followed by Chemotherapy (CHOP) or rituximab plus CHOP (R-CHOP) [5,6,8,10,11]. The indication for primary surgery is based on the high risk of complications (obstruction, perforation or bleeding) during chemotherapy. In addition, in some studies in patients with localized intestinal DLBCL, surgery plus chemotherapy was associated with a lower relapse rate than chemotherapy alone [10]. In the present case, the patient presented intestinal obstruction before definitive diagnosis, requiring emergent surgery. Once the diagnosis of DLBCL was obtained, treatment with three cycles of chemotherapy was completed. It was decided to administer this abbreviated chemotherapy regimen to reduce chemotherapy-related toxicities because it was a localized stage with negative resection margins, despite being a bulky disease. Rituximab was added to the CHOP regimen in our patient, despite the fact that several studies have shown no improvement in survival in patients treated with R- CHOP compared to those treated with CHOP [8].
The prognosis of localized colonic lymphoma treated with surgical excision and chemotherapy is good according to the results of some studies [4,5,10,11]. A prospective non-randomized trial that included patients with stage I/II GI DLBCL who received primary surgical resection followed by CHOP chemotherapy demonstrated favorable outcomes with a 5-year disease-free survival rate of 83% [11].
References
- Wong MT, Eu KW. Primary colorectal lymphomas. Colorectal Dis. 2006; 8: 586-591.
- Beaton C, Davies M, Beynon J. The management of primary small bowel and colon lymphoma-A review. Int J Colorectal Dis. 2012; 27: 555-563.
- Lo Re G, Federica V, Midiri F, et al. Radiological Features of Gastrointestinal Lymphoma. Gastroenterol Res Pract. 2016; 2016: 2498143.
- Bairey O, Ruchlemer R, Shpilberg O. Non-Hodgkin’s lymphomas of the colon. Isr Med Assoc J. 2006; 8: 832-835.
- Gay ND, Chen A, Okada CY. Colorectal Lymphoma: A Review. Clin Colon Rectal Surg. 2018; 31: 309-316.
- Tauro LF, Furtado HW, Aithala PS, D’Souza CS, George C, Vishnumoorthy SH. Primary lymphoma of the colon. Saudi J Gastroenterol. 2009; 15: 279-282.
- Bautista-Quach MA, Ake CD, Chen M, Wang J. Gastrointestinal lymphomas: Morphology, immunophenotype and molecular features. J Gastrointest Oncol. 2012; 3: 209-225.
- Hwang HS, Yoon DH, Suh C, Park CS, Huh J. Intestinal diffuse large B-cell lymphoma: An evaluation of different staging systems. J Korean Med Sci. 2014; 29: 53-60.
- Chang S, Shi X, Xu Z, Liu Q. TNM staging system may be superior to Lugano and Ann Arbor systems in predicting the overall survival of patients with primary gastrointestinal lymphoma. J BUON. 2015; 20: 812-819.
- Kim SJ, Kang HJ, Kim JS, Oh SY, Choi CW, et al. Comparison of treatment strategies for patients with intestinal diffuse large B-cell lymphoma: Surgical resection followed by chemotherapy versus chemotherapy alone. Blood. 2011; 117: 1958-1965.
- Lee J, Kim WS, Kim K, Ahn JS, Jung CW, et al. Prospective clinical study of surgical resection followed by CHOP in localized intestinal diffuse large B cell lymphoma. Leuk Res. 2007; 31: 359-364.