
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Incidental identification of the aberrant origin of left vertebral artery using magnetic resonance angiography: A case report
Forough Sodaei1; Vahid Shahmaei2; Maryam Noroozian3*
1 Department of Medical Physics and Biomedical Engineering, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
2 Radiology Technology Department, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3 Memory and Behavioral Neurology Department, Roozbeh Hospital, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Maryam Noroozian
Memory and Behavioral Neurology Department,
Roozbeh Hospital, Tehran University of Medical
Sciences, Tehran, Iran.
Email: Maryam.noroozian.mn@gmail.com
Received : Jun 11, 2021
Accepted : Jul 19, 2021
Published : Jul 23, 2021
Archived : www.jcimcr.org
Copyright : © Noroozian M (2021).
Abstract
Background: The vertebral arteries originate from the root of the neck as the first branches of the subclavian arteries. Variations of vertebral arteries are congenital anomalies occurring during embryonic development. Anatomic variations of the left vertebral artery are clinically symptomless and recognized incidentally during angiographic assessments or imaging techniques so the diagnosis of these anomalies is a serious challenge. Anomalous origin of vertebral arteries may lead to neurologic disorders. It is, thus, important to identify variations of the large vessels of the aortic arch when planning neck and cervical spine interventions and diagnostic radiology. For this reason, we would like to present this rare case of left vertebral artery showing a different origin.
Case report: In this work, we describe a 60-year-old female patient with headache, lethargy and blurred vision. We employed magnetic resonance angiography for both the brain and neck. There was no lesion in the brain. Incidentally, we found that the root of the left vertebral artery was anatomically aberrant. The left vertebral artery arose from the nearest section of the left external carotid artery, next to the bifurcation of the left common carotid artery, which is a rare variation.
Conclusion: Understanding the state of anomalous variations of the origin of the vertebral artery might have crucial implications in angiographic and surgical procedures. It is beneficial to perform more screening with noninvasive studies like neck magnetic resonance angiography in clinical cases with potential symptoms coexisting with other diseases in order to predict possible future problems in intracranial and extracranial interventions.
Keywords: Vertebral artery; external carotid artery; anatomic variation; magnetic resonance angiography.
Citation: Sodaei F, Shahmaei V, Noroozian M. Incidental identification of the aberrant origin of left vertebral artery using magnetic resonance angiography: A case report. J Clin Images Med Case Rep. 2021; 2(4): 1241.
Background
The complex anatomy of extra-cranial and intra-cranial arteries has been investigated for many years. Contrast-enhanced MR Angiography (CE MRA) has been recently introduced as an alternative, noninvasive method for evaluating vascular disease, and is now routinely used as a diagnostic tool in the assessment of different parts of body especially the vertebrobasilar diseases. It provides deeper insight into the circulation of the cranial and intracranial vessels under normal conditions and in pathological states caused by both anatomical anomalies and other abnormalities [1-3]. Anatomical anomalies of vessels do not have specific symptoms that could suggest early diagnostic tests due to a wide and heterogeneous range of symptoms similar to other disease. So they are mostly identified incidentally. Anatomical disparity in the Vertebral Artery (VA) are considered as an embryonic malformation with less common incidence [4].
Anatomical variations of the VAs include: maldevelopment of one VA, coexisting with compensatory dilatation of the contralateral artery, absence of one of the VAs, anomalies in VA origin from the aortic arch or from the common carotid artery, paired origin of one VA forming a common vascular trunk, asymmetrical duplication of the VA, etc. [5]. Less commonly, the vertebral arteries arise from the external or internal carotid artery [6]. In this work, we describe a case with the left VA arising from the left proximal external carotid artery in an individual with symptoms, and we will discuss this rare variation.
Case report
Our Persian patient was a 60-year-old non-smoker woman who presented with a history of headache, lethargy and blurred vision. The symptoms were first noted in 2018, after which she visited a nearby clinic. The neurologist asked for brain MRI as well as brain and neck MRA. After that, she was referred to our medical imaging center. The subject underwent brain scanning on 1.5 Tesla GE HDXT MR Scanner with 8 channels head coil. Routine brain MRI was performed. 3D-TOF MRA of the brain was obtained using 3D T1-weighted SPGR. Neck angiography was performed through Contrast Enhanced MRA. A 15 ml of contrast agent (Dotarem) was administered intravenously, 0.01 mmol/kg (or 0.2 mg/kg), at a rate of 3.0 mL/s followed by 20 mL bolus of normal saline. The 3D MRA images reconstruction was carried out by MIP (maximum intensity projection) and VR (Volume Rendering). Brain Magnetic resonance imaging showed no lesion or abnormality. The circle of Willis was normal and there was no atherosclerotic disease or Arteriovenous Malformation (AVM) in the Brain MRA (Figure 1).
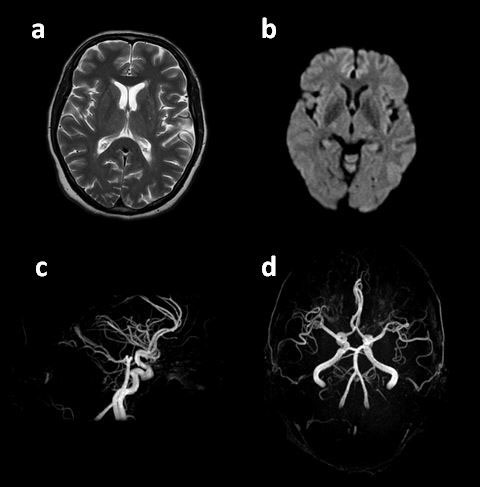
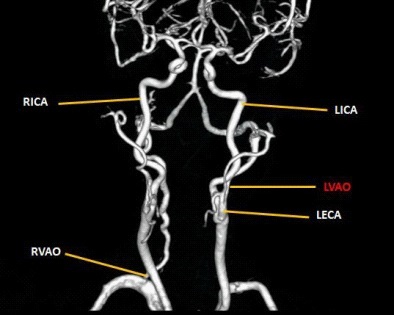
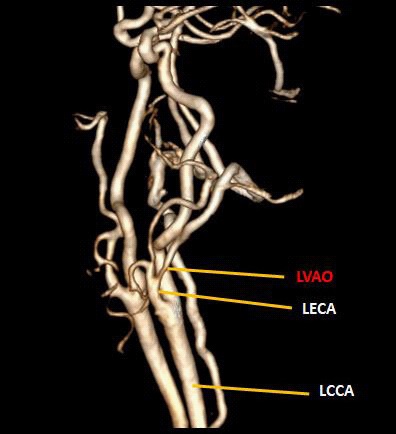
At the first look, the neck MRA seemed to be normal and there was no arterial stenosis or other pathological abnormalities. Interestingly, with more precise observation, we found that the left VA arose from the nearest section of left external carotid artery, next to the bifurcation of the Left common carotid artery which is a rare variation (Figure 2-4).

Discussion
MRI is a precise diagnostic tool for many cerebrovascular diseases [7]. Specifically, CE-MRA is becoming increasingly common, and with improvement of the spatial resolution of this technique, identifying pathology including lesions and abnormalities of the large vessels and vertebral arteries will become a popular method [8]. During the process of embryologic development, anatomic variants can form. The VAs may take place in different ways and need to be observed in their ordinary position to avoid a misdiagnosis where the vessels are congenitally absent. Aberrant origins may lead to hemodynamic alterations and predispose the patient to intracranial aneurysm formation. In this study, our case describes the variation of the left VA origination. In general, the left vertebral artery originates from the left subclavian artery. Many publications have reported abnormal VAs with different genesis including trunk of thyrocervical artery, brachiocephalic artery, common carotid artery, and the aorta [9-12]. However, there are less than 5 studies which reported that VA originates from external carotid artery [8,13- 15]. Elevated risk for cerebrovascular accidents including ath for cerebrovascular accidents including atherosclerosis, intracranial vascular deformities, arterial cutting up and resulting intracranial complexities due to confusion of the blood flow proceeding from aberrant origin of the VAs have been illustrated in many studies [8-16]. The extra-cranial section of the VA is often affected by atherosclerosis leading to a restriction notably in its root [17]. VA stenosis typically occurs at the origin and is the direct cause of 9% of posterior circulation ischemic strokes and TIA [18]. Following the previous studies, most individuals with structural anomalies of the left vertebral artery are clinically symptomless or with symptoms resulting from other than the abnormal VA [19], so it is crucial to identify this anatomical variation.
Conclusion
In the current study, a case with a rare variation of abnormal root of left VA was presented. In angiography, vascular surgery, and spinal surgery including cervical spines, it is essential to detect unusual anatomies of the VAs, as it can reduce the risk of VA trauma during interventional radiological procedures. In addition, it can deepen physicians' understanding of hemodynamics, time-saving techniques, and contrast media consumption during angiographic catheterization [20,21]. Additional screening is required with noninvasive studies like MRA in patients with potential symptoms so as to be aware of likely interventional complications.
Acknowledgements: The authors would like to thank the staff of Bahar medical imaging center.
Ethical approval: The informed consent was obtained from a participant included in the study in accordance with the supervision of the ethics committee of Tehran University of Medical Sciences, Tehran, Iran.
References
- Koelemay MJ, Lijmer JG, Stoker J, Legemate DA, Bossuyt PM. Magnetic resonance angiography for the evaluation of lower extremity arterial disease: A meta-analysis. JAMA. 2001; 285: 1338-1345.
- Grist TM. MRA of the abdominal aorta and lower extremities. J Magn Reson Imaging. 2000; 11: 32-43.
- Adamis MK, Li W, Wielopolski PA, et al. Dynamic contrast-enhanced subtraction MR angiography of the lower extremities: Initial evaluation with a multisection two-dimensional time-offlight sequence. Radiology 1995; 196: 689-695.
- Kim YD, Yeo HT, Cho YD. Anomalous variations of the origin and course of vertebral arteries in patients with retroesophageal right subclavian artery. J Korean Neurosurg Soc. 2009; 45: 297–299.
- Spielmeyer W. The anatomic substratum of yhe convulsive state. Arch Neurol Psychiatry 1930; 23: 869.
- Olszewski J, Niewiadomski P. Anatomical Anomalies of CarotidVertebral Arteries in Patients with Dizziness and Impaired Hearing. In: Rezzani R, Rodella LF, eds. Carotid Artery - Gender and Health. IntechOpen. 2018.
- Sodaei F, Shahmaei V. Identification of penumbra in acute ischemic stroke using multimodal MR imaging analysis: A case report study. Radiol Case Reports. 2020; 15: 2041–2046.
- Satti SR, Cerniglia CA, Koenigsberg RA. Cervical vertebral artery variations: An anatomic study. Am J Neuroradiol. 2007; 28: 976– 980.
- Brugièrest P, Djindjian M, Revel MP, Chakir N, Gaston A. Anterior cervical spinal artery originating from a right vertebral artery with a bifid origin. Neuroradiology. 1990; 32: 506-507.
- Gluncic V, Ivkic G, Marin D, Percac S. Anomalous origin of both vertebral arteries. Clin Anat. 1999; 12: 281–284.
- Kesler WW, Sabat SB. Isolated anomalous origin of the vertebral artery from the common carotid artery. Interact Cardiovasc Thorac Surg. 2018; 27: 615–616.
- Akdemir Aktaş H, Farımaz M, Fırat A, Göçmen R. Rare congenital anomalies of the internal carotid artery: anatomic and radiologic aspects of three cases and review of the literature. Surg Radiol Anat 2020; 42: 1363–1370.
- Ali A, Sedora Roman NI, Cox M, Kung D, Choudhri O, Hurst RW, et al. Anomalous Origin of the Right Vertebral Artery from the Right Common Carotid Artery. Cureus. 2018; 10.
- Flynn RE. External carotid origin of the dominant vertebral artery. Case report. J Neurosurg. 1968; 29: 300–301.
- Lin CY, Liu YS, Chen YC, Shih YH, Chang CC. Variations in the origin and course of the extracranial vertebral artery on multidetector computed tomography angiography. Iran J Radiol 2018; 15: e61623.
- Goray VB, Joshi AR, Garg A, Merchant S, Yadav B, et al. Aortic arch variation: a unique case with anomalous origin of both vertebral arteries as additional branches of the aortic arch distal to left subclavian artery. AJNR Am J Neuroradiol. 2005; 26: 93-95.
- Mahmutyazicioǧlu K, Saraç K, Bölük A, Kutlu R. Duplicate origin of left vertebral artery with thrombosis at the origin: Color Doppler sonography and CT angiography findings. J Clin Ultrasound. 1998; 26: 323–325.
- Caplan LR, Wityk RJ, Glass TA, et al. New England Medical Center Posterior Circulation registry. Ann Neurol 2004; 56: 389–398.
- Caplan LR, Wityk RJ, Glass TA, et al. New England Medical Center Posterior Circulation registry. Ann Neurol. 2004; 56: 389-398.
- Gluncic V, Ivkic G, Marin D, Percac S. Anomalous origin of both vertebral arteries. Clin Anat. 1999; 12: 281-284.
- Tsai IC, Tzeng WS, Lee T, et al. Vertebral and carotid artery anomalies in patients with aberrant right subclavian arteries. Pediatr Radiol. 2007; 37: 1007-1012.