
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Incarcerated intrapericardial diaphragmatic hernia after laparoscopic pericardial window for malignant pericardial effusion
Ekhlas S Bardisi1,2*; Luning Redmer1*; Luk Verlaeckt1; Filip Vanrykel1
1 Department of Thoraco-Abdominal Surgery, AZ Sint-Blasius, Dendermonde, Belgium.
2 Department of General Surgery, KAUH, Jeddah, KSA.
*Corresponding Author: Ekhlas S Bardisi
Department of Thoraco-abdominal Surgery, AZ
Sint-Blasius, Dendermonde, Belgium, Department
of General Surgery, KAUH, Jeddah, KSA.
Email: e--s--b@hotmail.com
Received : Aug 08, 2021
Accepted : Sep 03, 2021
Published : Sep 08, 2021
Archived : www.jcimcr.org
Copyright : © Bardisi ES (2021).
Abstract
Laparoscopic Pericardial Window (LPW) is a safe, minimally invasive surgical technique for treating pericardial effusion/tamponade. This technique allows adequate decompression and avoids single-lung ventilation and the need for thoracic drainage in severely ill patients; it also provides anatomopathological and microbiological diagnosis leading to treatment measures. An intrapericardial diaphragmatic hernia is among the rarest complications of this procedure.
A 85-year-old man, who underwent LPW for pericardial tamponade, presented to the emergency department 12 days post-operative with bowel obstruction; CT scan showed an incarcerated hernia into the pericardial sac. Laparoscopic reduction and hernia repair were performed using a large-pore Mesh to allow further drainage of histologically proven malignant pericardial effusion.
Keywords: pericardial tamponade; pericardial window; surgical drainage of pericardial effusion; intra-pericardial diaphragmatic hernia.
Citation: Bardisi ES, Redmer L, Verlaeckt L, Vanrykel F. Incarcerated intrapericardial diaphragmatic hernia after laparoscopic pericardial window for malignant pericardial effusion. J Clin Images Med Case Rep. 2021; 2(5): 1300.
Introduction
Surgical options for treatment of pericardial effusions and tamponades include pericardiectomy, trans-pleural approach (via thoracotomy or thoracoscopy), sub-xiphoidal approach, or via Laparoscopic Pericardial Window formation (LPW).
LPW is a safe and minimally invasive surgical technique for the treatment of malignant pericardial effusion and tamponade. This technique induces adequate pericardial sac decompression while avoiding single-lung ventilation and the need for thoracic drainage in severely ill patients and patients with suspected or proven malignant effusion. It also provides an anatomopathological and microbiological diagnosis. However, as in every surgery, there is a risk of complications. Amongst all complications, an incarcerated intrapericardial diaphragmatic hernia is the rarest and can have lethal consequences, either by mass effect on cardiac structures leading to tamponade or by strangulation of the herniated contents.
Case report
We report a 85-year-old man with a history of renal cell carcinoma who recently underwent a laparoscopic pericardial window to treat a pericardial tamponade and obtain an anatomopathological diagnosis as malignant effusion was suspected.
The histopathological findings showed cellular infiltration by a non-Hodgkin lymphoma, a large cell type.
He presented to the emergency department 12 days after hospital discharge with signs and symptoms of bowel obstruction; CT-abdomen showed incarcerated small bowel into the pericardial sac, Figure 1.

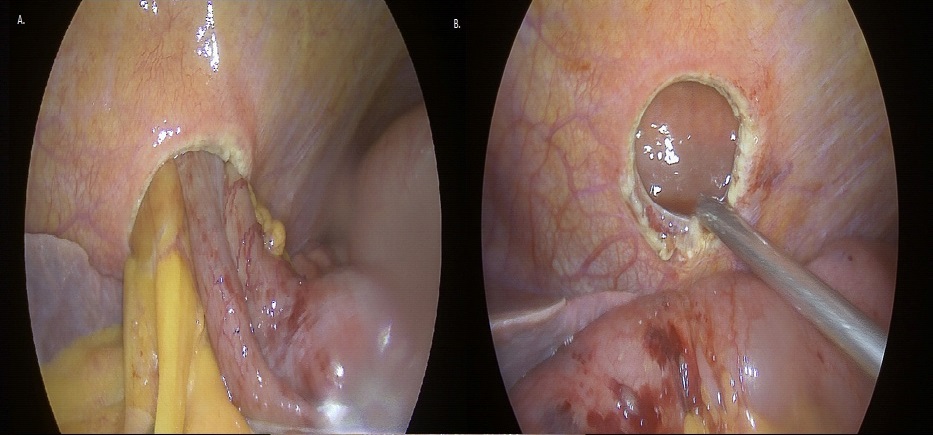
Urgent laparoscopic exploration showed the incarcerated hernia via the iatrogenic pericardial window. Reduction of the hernia was performed. In total, 50 cm of the small intestine was reduced from the pericardial sac, Figure 2. No resection was required.
The diaphragmatic hernia-defect was bridged with a DualLayer Composite large-pore IPOM-DynaMesh®. The mesh was fixed with CapSure™, Figure 3.

Post-operatively, the patient gained a fast and full recovery of bowel motility and was transferred to the hematological unit for further oncological workup. The diagnosis of a stage IVa diffuse large B-cell non-Hodgkin lymphoma with pericardial invasion was confirmed.
Rituximab and reduced dose CHOP (R-mini-CHOP) chemotherapy were offered to the patient. Unfortunately, the patient experienced severe toxicity, halting further treatment.
Best supportive care was given to the patient.
Comments
Laparoscopic transdiaphragmatic pericardial window has been proven to be a simple, fast, safe, and effective surgical technique for diagnostic and therapeutic purposes in the case of pericardial effusion and tamponade.
We describe a rare but potentially fatal complication of this procedure.
One should consider incarcerated iatrogenic diaphragmatic herniation after LPW when a patient presents with signs of bowel obstruction.
Computed tomography should be the preferred diagnostic imaging.
Although rare, a confirmed pericardial diaphragmatic hernia should be repaired immediately to avoid the risk of bowel strangulation and unneeded resection. Laparoscopic reduction and hernia repair should be performed using Dual-Layer Composite large-pore Mesh to allow further drainage of suspected/proven malignant or chronic pericardial effusion.
Ethical approval: Ethics Committee informed that approval was not required for this study.
Consent: Unfortunately, the patient died few weeks after the start of the chemotherapy, we received only verbal consent from the patient before his death, and we could not reach any first-degree relatives to obtain their consent. However, all the images and the data have been used anonymously in this paper. A copy of the declaration letter confirming the anonymized data is available for review by the Editor-in-Chief of this journal on request.
Conflict of interest statement: None to declare.
Funding sources: No funding was obtained for this study.
References
- Mann GB, Nguyen H, Corbet J. Laparoscopic creation of pericardial window. Aust N Z J Surg. 1994; 64: 853-5.
- Totté E, Hee R, Brabant P, Wollaert B, Gheuens E, et al. Laparoscopic transabdominal pericardial window: new standard in the treatment of recurrent pericardial effusion complicated by cardiac tamponade. Surg Endosc. 2002; 16: 859-63.
- Chin RY, Glew MJ, Brady P. Iatrogenic intrapericardial diaphragmatic hernia. ANZ J Surg. 2002; 72: 681-3.
- Picardi EJ, Bedingfield J, Statz M, Mullins R. Laparoscopic pericardial window. Surg Laparosc Endosc. 1997; 7: 320-3.
- Smith CA, Galante JM, Pierce JL, Scherer LA. Laparoscopic transdiaphragmatic pericardial window: getting to the heart of the matter. J Am Coll Surg. 2011; 213: 736-42.
- Docekal J, Fabian T. Pericardial window formation complicated by intrapericardial diaphragmatic hernia. Case Rep Surg. 2014; 2014: 132170.
- Staltari D, Diaz A, Capellino P, Benavides F, Ramos R, Pierini L, Morales I. Laparoscopic pericardio-peritoneal window: an alternative approach in the treatment of recurrent pericardial effusion, in-hospital evolution and survival. Surg Laparosc Endosc Percutan Tech. 2007; 17: 116-9.