
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Endoscopic closure of duodenal perforation post-endoscopic retrograde cholangiopancreatography: A case report
Ramin Niknam; Gholam Reza Sivandzadeh*
Gastroenterohepatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
*Corresponding Author: Gholam Reza Sivandzadeh
Gastroenterohepatology Research Center (GEHRC),
Shiraz University of Medical Sciences, Namazi Hospital,
Third floor, 71935-1311 Shiraz, Iran.
Email: ghsivand@sums.ac.ir
Received : July 07, 2021
Accepted : Sep 06, 2021
Published : Sep 10, 2021
Archived : www.jcimcr.org
Copyright : © Sivandzadeh GR (2021).
Abstract
Background: Duodenal perforation post - Endoscopic Retrograde Cholangiopancreatography (ERCP) is uncommon, but if not treated well enough in time, it can have serious consequences. There are few reports that endoscopic-related duodenal perforation has been successfully treated using endoclips.
Case presentation: A 63-year-old woman was referred for ERCP because of cholestatic jaundice caused by common bile duct stones. During the procedure, duodenal perforation post-ERCP was suggested. The endoscopic repair of the perforation was performed immediately using 5 endoscopic clips. Antibiotic therapy was also started and clinical and radiological follow-up was performed. Patient condition was good immediately after surgery and during hospitalization.
Conclusion: Endoscopic treatment of duodenal perforation postERCP can be suggested as a treatment option in highly selected patients which may lead to a reduction in the frequency of surgical interventions.
Keywords: endoscopic retrograde cholangiopancreatography; endoscopy; perforation; endoscopic clips.
Citation: Niknam R, Sivandzadeh GR. Endoscopic closure of duodenal perforation post-endoscopic retrograde cholangiopancreatography: A case report. J Clin Images Med Case Rep. 2021; 2(5): 1304.
Introduction
Endoscopic retrograde Cholangiopancreatography (ERCP) is a diagnostic-therapeutic procedure that has the risk of various complications, including duodenal perforation. Duodenal perforation post-ERCP is uncommon, but if not treated well enough in time, it can have serious consequences. Duodenal perforation is difficult to diagnose during the ERCP. While patients with lateral or medial wall duodenal perforation would invariably require immediate surgical approach, those resulting from guidewire or basket instrumentation may often be managed conservatively [1-4].
Case report
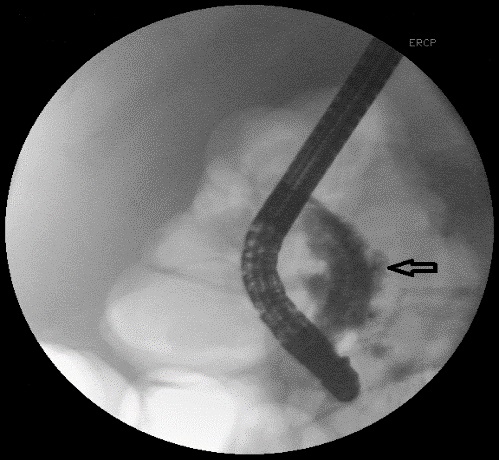
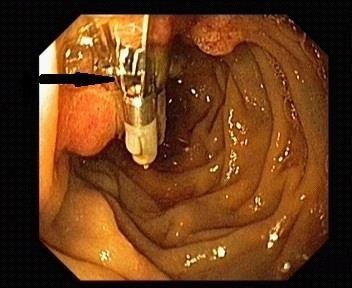
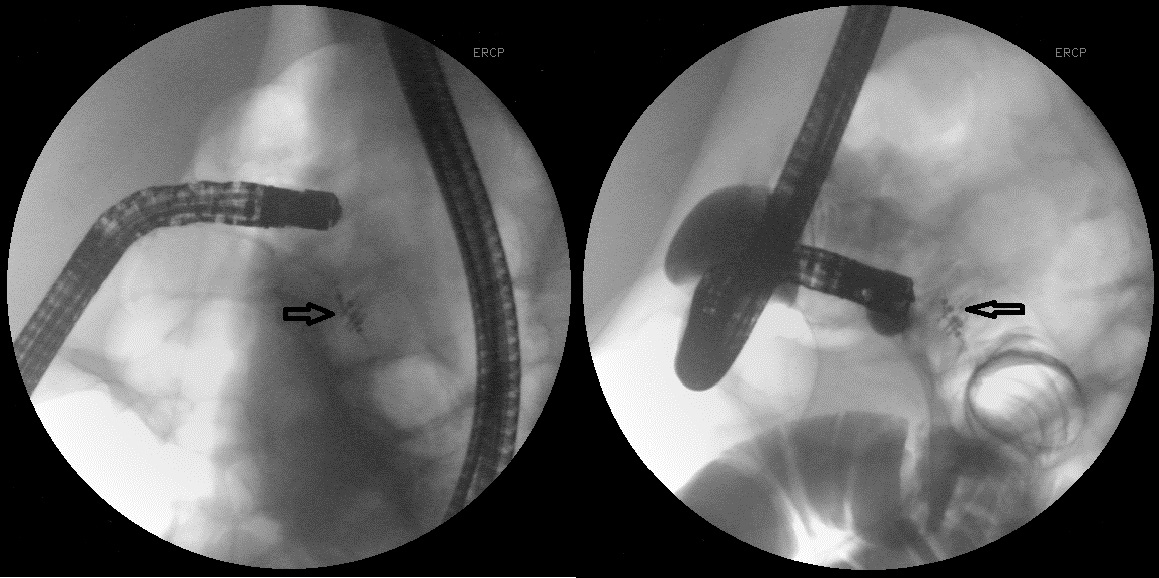
A 63-year-old woman was referred for ERCP because of cholestatic jaundice caused by Common Bile Duct (CBD) stones. The patient had a history of cholecystectomy due to gallstones 6 months prior to the present visit. During ERCP, after sphincterotomy and contrast (Meglumine compound) injection for CBD cannulation, contrast was completely diffused in the retroperitoneal space and duodenal perforation post- ERCP was suggested (Figure 1). The endoscopic repair of the perforation was performed immediately using 5 endoclips (Figure 2). The success of perforation closure was demonstrated by contrast injection just after endoscopic treatment (Figure 3,4). Antibiotic therapy was started and clinical and radiological follow-up was performed. Patient condition was good immediately after surgery and during hospitalization, with no new complications.
Discussion
There are a few reports that endoscopic-related duodenal perforation has been successfully treated using endoclips [5,6]. We presented a case of duodenal perforation post-ERCP that was successfully treated by endoscopic endoclips. Duodenal perforation is an uncommon complication of ERCP [4], but if not treated well enough in time, it can have serious consequences. Duodenal perforation is difficult to diagnose during the ERCP because routine use of sedative during the procedure is performed as well as perforation occurs in the lateral wall of duodenum by the side view endoscope. The mechanism, location, and extent of perforation diagnosed by due to clinical and radiographic characteristics can contribute to a conservative or surgical approach [4]. The risk of ERCP-related perforation increases with older age, sphincterotomy, the presence of sphincter of Oddi dysfunction, CBD dilatation, biliary stenosis, and longer duration of this process [1]. Machado, in a literature review on 251 cases of ERCP-related perforation, found that the predominant perforation site were duodenal wall (34.5%), perivaterian (31.3%), common bile duct (23.0%), and unknown (7.9%). Conservative management was applied in 62.2% of which 92.9% were successful. The most important factor for better outcome was early diagnosis and prompt treatment [4]. While patients with lateral or medial wall duodenal perforation would invariably require immediate surgical approach, those resulting from guidewire or basket instrumentation may often be managed conservatively [1-4].
According to a few case reports, similar to our patient, endoscopic-related duodenal perforation has been successfully treated using endoclips Endoscopic treatment of iatrogenic gastrointestinal perforations through endoclips is a safe and effective method that has led to a reduction in the frequency of surgical interventions [5,6].
Conclusion
Endoscopic treatment of duodenal perforation post-ERCP can be suggested as a treatment option in highly selected patients which may lead to a reduction in the frequency of surgical interventions.
Conflict of interest: Authors declared that there is no conflict of interests.
References
- Enns R, Eloubeidi MA, Mergener K, Jowell PS, Branch MS, et al. ERCP-related perforations: risk factors and management. Endoscopy. 2002; 34: 293-298.
- Ercan M, Bostanci EB, Dalgic T, Karaman K, Ozogul YB, et al. Surgical outcome of patients with perforation after endoscopic retrograde cholangiopancreatography. J Laparoendosc Adv Surg Tech A. 2012; 22: 371-377.
- Nepal P, Maemura K, Mataki Y, Kurahara H, Kawasaki Y, et al. Management of horizontal duodenal perforation: A report of three cases and review of literature. Surg Case Rep. 2017; 3: 119.
- Machado NO. Management of duodenal perforation post-endoscopic retrograde cholangiopancreatography. When and whom to operate and what factors determine the outcome?. A review article. JOP. 2012; 13: 18-25.
- Parlak E, Koksal A, Disibeyaz S, Uskudar O, Sasmaz N. Endoscopic closure of ERCP-related duodenal perforations by using endoclips: A case series. Surg Laparosc Endosc Percutan Tech. 2013; 23: e225-228.
- Nakagawa Y, Nagai T, Soma W, Okawara H, Nakashima H, et al. Endoscopic closure of a large ERCP-related lateral duodenal perforation by using endoloops and endoclips. Gastrointest Endosc. 2010; 72: 216-217.