
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Remarks on patients with traumatic brain injury due to traffic accident related to alcohol comsumption treated in Vietduc hospital after implementing the decree 100
Nguyen Duc Chinh1*; Dinh Van Quynh1,2; Pham Gia Anh1; Pham Hai Bang1
1 Viet Duc University Hospital, Vietnam.
2 Thang Long University, Vietnam.
*Corresponding Author: Nguyen Duc Chinh
Department of Infectious Diseases, Viet Duc University
Hospital, 40 TrangThi, HoanKiem, HaNoi, Vietnam.
Email: duc_chinh1960@yahoo.com
Received : Aug 31, 2021
Accepted : Sep 21, 2021
Published : Sep 28, 2021
Archived : www.jcimcr.org
Copyright : © Song X (2021).
Abstract
Purpose: Traumatic Brain Injury (TBI) is still considered as a leading cause of morbidity and mortality of victims by traffic accident. Despite a fact that many measurements and preventions have been applied, the rate of TBI is remained high. Aim of this study was to investigate treatment process of TBI caused by road traffic accident at Viet Duc Hospital after the Decree 100 which has been issued in Vietnam in early 2020.
Materials and method: A retrospective and prospective study has been conducted in Viet Duc Hospital from Dec, 2020 to March, 2021. All the patients with TBI by road traffic accident were enrolled. Severity of TBI was identified by Glasgow Scale (GCS) and BAC (Blood Alcohol Concentration) test taken on arrival. The data was collected from medical record as well as autopsy report and analysed by SPSS.20.0
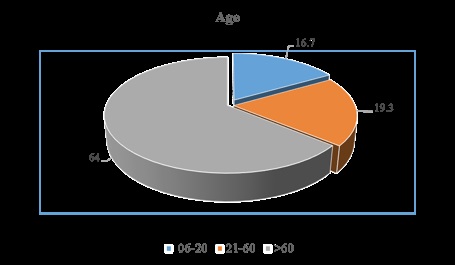
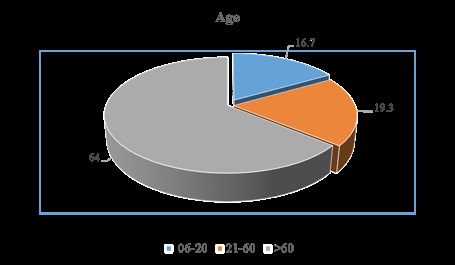
Results: A total of 150 patients with TBI by road traffic accidents were enrolled, age group from 21 to 60 years old accounted for 64%, male accounted for 86.7%. Associated injuries were maxillofacial lesions 48%, extremities 24.7%, chest accounted for 20%. Severity of TBI with GCS 6 - 8 was the highest rate 52%, from 3 - 5 GCS accounted for 30%. 40% were operated on emergency; BAC was positive 46.7%, of which over from 50 mg/L accounted for 32.6%. The patients with GCS from 6 to 8 were BAC positive accounted for a higher rate than groups with GCS above 9 or below 5. The most common TBI lesions were subarachnoid hemorrhage, subdural hematoma and cerebral edema accounted for 67.3%, 60% and 58% respectively. Overall mortality was 26% including in-hospital death and discharged to die.
Conclusions and recommendations: Data from the study has shown that many young men with severe TBI by road traffic accident were BAC positive which can results in the high risk of death and disability. Thus, we highly recommend counterparts should constantly strengthen the propaganda and enforcement measures in order to reduce traffic accidents and TBI patients.
Keywords: traffic accidents; injury; brain trauma severity.
Citation: Chinh ND, Quynh DV, Anh PG, Bang PH. Remarks on patients with traumatic brain injury due to traffic accident related to alcohol comsumption treated in Vietduc hospital after implementing the decree 100. J Clin Images Med Case Rep. 2021; 2(5): 1327.
Introduction
Fatality rates of road traffic accidents caused by alcohol were investigated by the World Health Organization (WHO): Each year, up to 1.35 million people die from traffic accidents, especially in developing countries with high incidences and mortalities, most of them are young adults. An analysis carried out by Allianz showed the significant regional differences: Eastern Europe and central Asia hold the tragic top position with 18.2%, followed by Europe (16.7%) and the Americas (12.9%). Meanwhile, Africa (8%), Asia Pacific (7.3%) and the Middle East (2.4%) stay below the global average of 10.9%. Damage caused by injury globally accounts for 3-5% of gross national income [1-3].
Vietnam is among the countries with high rates of traffic accidents in the world and in the region, reasons are mainly related to alcoholic use. Recently, serious traffic accidents which occurred related to drinking while driving resulted in many victims dying from severe injuries. After Decree 100 has been implemented early in 2020, together with the the Covid-19 pandemic occurred, the number of traffic accidents as well as the victims were decreased. However, there are still many trauma patients related to alcohol abuse, participate in traffic and the mortality is the most common aftermath in the patients with Traumatic Brain Injury (TBI) [4,5].
We have conducted a study to assess the patients with TBI by road traffic accident related to alcohol abuse in which have been treated at Viet Duc University Hospital, a leading surgical facility in Vietnam that is always overloaded with trauma cases. The study aims to give a general picture of the situation of victims by road traffic accidents related to alcohol use in particular after implementing Decree 100 regarding the “Provisions On Penalties For Administrative Violantions In Road And Rail Traffic”, through which we would make recommendations to strengthen the national traffic accident prevention program.
Materials and methodologies
Selection criteria
All patients with TBI caused by road traffic accidents who were cared in the Emergency Department at Viet Duc University Hospital from December 31, 2020 to March 31, 2021, regardless of gender, age, locality and profession, completed medical records, including deaths enrolled.
Blood alcohol concentration test (BAC - Blood Alcohol Concentration) according to the regulations of the Ministry of Health and standard testing machine system of the hospital (Inter-Ministerial Circular 26/2014 July 2014) [6].
Severity of TBI according to Glasgow–Glasgow scale (GCS) which score of 12 or less [7].
Exclusion criteria: Patients with TBI but not caused by traffic accident, Medical records were not completed
Methodology: A retrospective and prospective study
Analysis of database: The data was processed by SPSS.20.0
Results
During the study period, we investigated a total 150 patients with TBI due to road traffic accident caring on emergency, distributed as follows:
The study showed that the patients were BAC positive provided poor care 2.23 times higher than those who do not use alcohol, the difference is statistically significant with p < 0.05.
Discussions
According to WHO, in 2016, alcohol abuse caused about 3 million deaths, accounting for 5.3% of all deaths worldwide. The mortality rate caused by alcohol abuse is higher than counterpart caused by all types diseases such as tuberculosis, HIV/AIDS and diabetes. For non-communicable diseases alone, alcohol caused about 1.7 million deaths, including about 1.2 million deaths from digestive and cardiovascular diseases (0.6 million deaths per year) and 0.4 million deaths from cancers. Not only that, globally, alcohol causes 0.9 million injury deaths, including about 370,000 deaths from traffic accidents [1].
Vietnam is no exception, according to a national survey has conducted in 2015, 44% people drank alcohol excessively, which is a dangerous to health. Additionally, the survey also mentioned that Vietnam produced 3.4 billion liters of beer, 70 million liters of industrial alcohol and about 250 million liters of traditional alcohol. The rate of alcohol use is at an alarming level. On average, each Vietnamese person consumes about 6.6 liters of alcohol/person/year, the percentage of men and teenagers using alcohol is high. This leads to 79,000 deaths in 2016, numerous people were hospitalized for treatment whose cases were related to road traffic accidents and alcohol comsumption [5].
In the report of L M Anh from Vietnam Health Environmental Management Agency (VIHEMA) [8], through the recent statistics on road accidents, the number of cases related to alcohol use was 11.646, accounting for about 9%; The number of patients with BAC positive was 7.340, accounting for 5.7%. The rate of men using alcohol was 12.9 times higher than that of women, BAC level from 50mg/dl to 300mg/dl accounted for 45.8% in the age group from 20 years old to 29 years old. In research by Nguyen Duc Chinh et al [9] at Viet Duc University Hospital in the period between 2011 and 2016 also showed that victims of traffic accidents with BAC exceeding the allowable limit accounted for over 7%. The data of Vu Anh Tuan (VietnameseGerman Transport Research Center) collected in 2018 in Binh Duong and Ho Chi Minh City showed that the rate of traffic accidents by alcohol abuse was 2.6% and 5.1%, respectively, male victims accounted for nearly 90% [10].
In the international reports conducted Sulovic D [12] for 10 years (2001-2011) in Croatia enrolled total 474 deaths related to traffic accidents, 337 cases (71.1%) with BAC positive, in which 117 cases (34.7%) had BAC level 0.5g/kg body and victims of traffic accidents were mostly male drivers, and those accidents were more often associated with alcohol consumption; Petkovic S [13], researched on the influence of the law on prevention of alcohol harms and traffic accidents for 10 years from 2004-2013 in Serbia found that there was no obvious change of death rate, especially after 4 years of applying alcohol-related road, therefore the author recommended adjusting the BAC in traffic law. According to report of Reynaud M [14] in France the victims of traffic accident with BAC higher than the permission limit (0.50 g/L in France) accounted for an overall rate of 9.8%, in which were fatal with BAC higher than the allowed level accounted up to 31.5%. One leading cause of mortality related to road traffic accident is TBI, especially severe TBI, so the burden is increasing worldwide. This issue is also very concerned in the United States. According to statistic of Zachary M et al. [15] about 2.8 million civilians receive medical treatment for TBI, the total cost comprising health care dollars, loss of productivity, and quality of life, associated with TBI in the United States is substantial, with estimates of lifetime cost (in 2009 dollars) ranging from more than $75 billion to more than $200 billion
In our study, the age group of TBI by road traffic accidents was from 21 to 60 years old accounting for 64%, male accounted for the majority of 86.7% (Chart 1-2). The highest rate of associated injuries were maxillofacial injuries in 48%, limb injuries in 24.7%, chest injuries 20% (Table 1). Due to the victims were young and in working age group, if not recovered from TBI, will be a great burden for society, health and families due to a long term care.
Table 1: Associated injuries (N = 150).
Description |
n |
% |
Abdomical injuries |
13 |
8.7 |
Chest injuries |
30 |
20 |
Spine injuries |
12 |
8.0 |
Maxillofacial injuries |
72 |
48.0 |
Extremities injuries |
37 |
24.7 |
Regarding the severity of TBI and prognosis according to the GCS scale, our study showed that the patients with severe TBI level accounted for a high rate. The patients with GCS score of 6 – 8 accounted for the highest rate of 52% (Table 2), in which 40% were operated on emergency. However, the rate of serious cases being discharged to die at home accounted for 25.3%, 0.7% died in hospital, overall mortality was 26% (Table 4). Most common findings from CT scanner were the subarachnoid hemorrhage accounted for 67.3%, followed by subdural hematoma, cerebral edema accounted for 60% and 58% respectively. These types of TBI were mostly indicated for surgery on emergency with high mortality proportion (Table 3).
Table 2: GCS severity (N = 150).
Description |
n |
% |
GCS 3-5 points |
45 |
30.0 |
GCS 6-8 points |
78 |
52.0 |
GCS 9-12 points |
27 |
18.0 |
GCS 13 – 15 points |
0 |
0 |
Total |
150 |
100 |
Table 3: Lesions on CT scanner (N = 150).
Description |
n |
% |
Extradural hematoma only |
50 |
33.3 |
Subdural hematoma only |
90 |
60.0 |
Intracranial hemorrhage |
43 |
28.7 |
Subarachnoid hemorrhage |
101 |
67.3 |
Cerebral contusion |
81 |
54.0 |
Cerebral edema |
87 |
58.0 |
Intraventicular hemorrhage |
21 |
14.0 |
Skull fracture only |
11 |
7.3 |
Other |
55 |
36.7 |
Table 4: Management of patients on emergency (N = 150).
Description |
n |
% |
Surgeries |
60 |
40.0 |
Admitted for further care in patient wards |
20 |
13.3 |
Caring in ICU |
15 |
10.0 |
Transferral |
14 |
9.3 |
Discharged to die at home * |
38 |
25.3 |
Died in first 6 hours * |
1 |
0.7 |
Other |
2 |
1.3 |
Total |
150 |
100 |
*Over all mortality was 26.0%
In the last years, the alcohol and drug abuse caused of traffic accidents in Vietnam was so much concerned. It was mentioned in the report of Vu Anh Tuan (Vietnamese-German Transport Research Center) in 2018, Nguyen Duc Chinh at al. in Viet Duc University Hospital from 2011 to 2016 showed the patients of traffic accidents with BAC exceeding the allowable limit (50mg/L) account for over 7%. Based on many reports and survey on this matter, the Vietnam government has issued the Decree 100 regarding Provisions On Penalties For Administrative Violantions In Road And Rail Traffic, of which mentioned about the allowable limit of BAC has revised to zero [9,10]. Many countries worldwide have implemented strict regulation for safe traffic such as in Germany if a driver has a blood alcohol level of over 1.1 per mille, auto physical damage insurance will no longer cover the damage to the driver's own vehicle. Similarly, liability insurance for damage to third parties will no longer hold full effect. Rights of recourse up to 5,000 EUR can be asserted by the insurer. In addition, the driver will be guilty of a criminal offence [3]
In our study, the rate of BAC positive was 46.7%, which means that nearly half of TBI patients violated the law as prescribed by Decree 100. In which, the patients with BAC from 50 – 150 mg/L accounted for 17.3%, over 150 mg/L accouted for 15.3% (Table 4). The number of TBI with GCS scoring from 6 to 8 were BAC positive accounted for a higher proportion than the GCS group above 9 and below 5. In the previous study by Nguyen Duc Chinh et al. at Viet Duc hospital also showed similar results of severe TBI usually has a higher BAC [9].
The prognostic factor for TBI patients will be worse because these cases have poor care outcomes 2.23 times higher than those who do not use alcohol, the difference is statistically significant with p< 0 ,05 (Table 5). The reason is that when the victim is admitted to the hospital in a coma (unconscious) condition mixed with a drunken status, it will make the process of diagnosis and care more difficult for patients who are not intoxicated. Most studies estimate that between 30% and 50% of patients treated for TBI were intoxicated at the time of injury, with even greater intoxication estimates for patients injured in motor vehicle accidents and assaults [15,16,17].
Table 5: Ethanol concentration related to the severity of stroke (N = 150)
BAC |
n |
% |
GCS |
GCS |
GCS |
Zero |
80 |
53.3 |
23 |
45 |
12 |
< 50mg/L |
21 |
14.0 |
3 |
11 |
7 |
50 – 150 mg/L |
26 |
17.3 |
13 |
12 |
1 |
> 150 mg/L |
23 |
15.3 |
6 |
10 |
7 |
Total |
150 |
100 |
45 |
78 |
27 |
Table 6: Relationship between alcohol use and care outcomes (N = 150)
Variables |
Outcomes |
OR |
p |
||
Poor |
Good |
||||
BAC |
Positive |
31 |
39 |
2,23 |
0.021 |
Negative |
21 |
59 |
|||
Total |
52 |
98 |
|
|
|
Other reports showed that alcohol use and Traumatic Brain Injury (TBI) are inextricably and bidirectionally linked. Alcohol intoxication is one of the strongest predictors of TBI, and a substantial proportion of TBIs occur in intoxicated individuals. An inverse relationship is also emerging, such as TBI can serve as a risk factor, or modulate the course of Alcohol Use Disorder (AUD). Critically, alcohol use after TBI is a key predictor of rehabilitation outcomes, prognosis, and additional head injuries. This review provides a general overview of the bidirectional relationship between TBI and AUD and a discussion of potential neuropsychological and neurobiological mechanisms that might underlie the relationship [18-21]. According to Sulovic D [12] Reynaud M [14], trauma cases caused by traffic accidents with BAC above 0.50 g/L all have high mortality rates, especially due to TBI and difficulties to manage in emergency.
Conclusions
Since the implementation of Decress 100 in early 2020, the number of victims by road traffic accident has decreased, including the TBI in general. However, still numerous serious TBI patients related to alcohol abuse have been treated in the high level hospitals as Viet Duc University Hospital. It is worth noting that there were many cases with high BAC affected the quality of care, resulting the high risk of morbidity and mortality. Additionally, almost the patients were young, so it burden to the medical care and social issue. Therefore, we recommend that it is still necessary to regularly strengthen monitoring of alcohol abuse when participating in traffic and strictly punish those who break the law
Acknowledgements: The contribution of all staff and colleagues in the departments of Emergency, Orthopedic, Planning of Viet Duc University Hospital.
References
- World Health Organization. Global status report on alcohol and health. 2018.
- World Health Organization. Global status report on road safety 2018. 17 June 2018.
- Allianz. Every tenth fatal traffic accident due to alcohol. 2014.
- Workshop on implementing the regulation and plans to strengthen the injury preventions in community for period from 2011 to 2015, 11th, August. Ministry of Health. 2011.
- Tran Thi Ngoc Lan, Luong Mai Anh, Khieu Thi Quynh Trang, Tran Dac Phu. Current death related to road traffic accident in Vietnam. Practical Medicine No. 786-2011: 67-70.
- Regulation on Testing The Blood Alcohol Concentration For Drivers Of Road Vehicles. 26/2014/TTLT-BYT-BCA. 2014.
- Teasdale G, Jennett B, Murray L, Murray G. Glasgow coma scale: to sum or not to sum. Lancet. 1983; 2: 678.
- Luong Mai Anh at al. The situation of alcohol use - traffic accidents and the prevention of the health sector. The transport Journal, Special issue of Traffic Safety. 55th year. 2016; 76-80.
- Nguyen Duc Chinh, Tran Tuan Anh, Pham Thi Thuy. Road traffic accidents related to alcohol use through trauma patients due traffic accidents treated at Viet Duc Hospital 2009-2010. Practical Medicine No. 786 – 2011: 37 - 40.
- Vu Anh Tuan. Impact of alcohol abuse related to the drivers’ behavior of motorcycle and motorbike in Vietnam. Workshop on Traffic accident prevention, Hanoi. 2018.
- David J.Hanson. Alcohol Consumption and Traffic Crashes. Sociology Department, state University of New York. 1997-2009.
- Sutlovic D, Scepanovic A, Bosnjak M, Versic-Bratincevic M, Definis-Gojanovic M. The role of alcohol in road traffic accidents with fatal outcome: 10-year period in Croatia Split-Dalmatia County. Traffic Inj Prev. 2014; 15: 222-7.
- Petković S, Palić K, Samojlik I. Blood alcohol concentration in fatally injured drivers and the efficacy of alcohol policies of the new law on road traffic safety: A retrospective 10-year study in autonomous province of Vojvodina, Republic of Serbia.Traffic Inj Prev. 2016; 17: 553-7.
- Reynaud M, Le Breton P, Gilot B, Vervialle F, Falissard B. Alcohol is the main factor in excess traffic accident fatalities in France. Alcohol Clin Exp Res. 2002; 26: 1833-9.
- Zachary M. Weil, John D. Corrigan, and Kate Karelina. Alcohol Use Disorder and Traumatic Brain Injury. Alcohol Res. 2018; 39: 171–180.
- Le Hoang Tung Uyen, Tran Quang Vinh. Outcome prediction in severe head in first 48 hours by GCS. Midical Journal of Hồ Chí Minh City. 2010; 14: 639 – 64
- Patel HC, Bouamra O, Woodford M, King AT, Yates DW, Lecky FE, “Trends in head injury outcome from 1989 to 2003 and the effect of neurosurgical. Lancet. 2005; 366: 1538-1544.
- Michael A. Vella, MD, MBA1, Marie Crandall, MD, MPH, FACS2, and Mayur B. Patel, MD, MPH, FACS3. Acute Management of Traumatic Brain Injury Surg Clin North Am. 2017; 97: 1015–1030.
- Werner C, Engelhard K. Pathophysiology of traumatic brain injury. Br J Anaesth. 2007; 99: 4–9.
- Orsi C, Ferraro OE, Montomoli C, et al. Alcohol consumption, helmet use and head trauma in cycling collisions in Germany. Accid Anal Prev. 2014; 65: 97–104.
- Bombardier CH, Rimmele CT, Zintel H. The magnitude and correlates of alcohol and drug use before traumatic brain injury. Arch Phys Med Rehabil. 2002; 83: 1765–1773.