
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Iridocorneal endothelial syndrome: Short report
Benchakroun S*; Taouri N; Tagmouti A; Cherkaoui LO
Department A of Ophthalmology, Mohammed V University Souissi, Rabat, Morocco.
*Corresponding Author: Benchakroun Saad
Department A of Ophthalmology, Mohammed V
University Souissi, Rabat, avenue al arz seceteur 10 lot
G4 hay riad Rabat, Morocco.
Email: saadbenchek@hotmail.fr
Received : Aug 27, 2021
Accepted : Sep 22, 2021
Published : Sep 29, 2021
Archived : www.jcimcr.org
Copyright : © Saad B (2021).
Citation: Benchakroun S, Taouri N, Tagmouti A, Cherkaoui LO. Iridocorneal endothelial syndrome: Short report. J Clin Images Med Case Rep. 2021; 2(5): 1332.
Short report
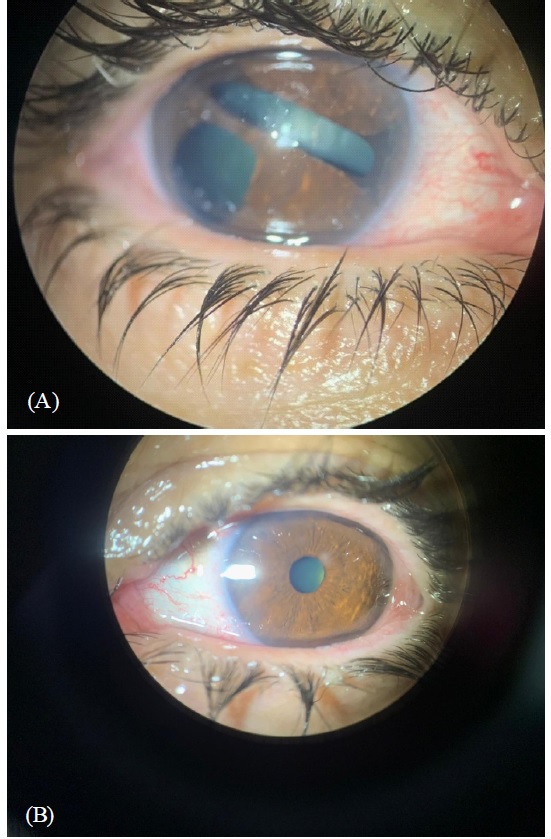
We report a case of a 42-year-old-woman, who presented to the ophthalmic consultation for decreased visual acuity complaints of blurred vision, altered pupillary shape since few months of her right eye.
The clinical examination found a reduced visual acuity to counting fingers in the right eye and 20/20 in the left eye. intraocular pressures was 38 mm Hg OD and 14 mm Hg OS. Slit lamp examination of the right eye found: Corneal edema, iris atrophy with a deformation of the iris architecture and pupillary anomalies, with polycoria (Figure 1). The evaluation of the angle by gonioscopy found areas of broad synechiae anterior to Schwalbe’s line (Figure 2). While the examination of the left eye was normal (Figure 1B). The posterior segment examination was normal in both eyes. Specular microscopy confirmed the presence of unilateral endothelial pleomorphism and polymegathism. In our case of the retained diagnosis was iridocorneal endothelial syndrome
The first clinical description was in 1903 by Harms [1,2]. which is a rare pathology, that touch the corneal endothelium, and leads to it abnormal proliferation [2]. This syndrome is usually unilateral and sporadic, which is commonly touch women in the third to fifth decade [3,4].
Conflict of interest: The author declares that there is no conflict of interest.

References
- Harms C. Eiseitige spontane Lukenbildung ber Iris ohne mechanische Zerrung. Klin Monatsbl Augenheilkd. 1903; 41: 522–528.
- Shields MB. Progressive essential iris atrophy, Chandler's syndrome, and the iris nevus (Cogan-Reese) syndrome: a spectrum of disease. Surv Ophthalmol. 1979; 24: 3-20.
- Wilson MC, Shields MB. A comparison of the clinical variations of the iridocorneal endothelial syndrome. Archives of Ophthalmology. 1989; 107: 1465–1468.
- Salim S, Shields MB, Walton D. Iridocorneal endothelial syndrome in a child. Journal of Pediatric Ophthalmology and Strabismus. 2006; 43: 308–310.