
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Primary Herpes Simplex viral infection of bilateral nipples and areolae with reactive arthritis: An uncommon presentation of a common disease
B Thanushah1*; N Thamilvannan2; M Ahilen3; S Ahilan4; SH Chandrarathna5
1 Acting Consultant Dermatologist, Teaching Hospital, Batticaloa, Sri Lanka.
2 Consultant Dermatologist, Teaching Hospital, Batticaloa, Sri Lanka.
3 Consultant Physician, Teaching Hospital, Batticaloa, Sri Lanka.
4 Consultant Histopathologist, Teaching Hospital, Batticaloa, Sri Lanka.
5 Registrar in Dermatology, Teaching Hospital, Batticaloa.
*Corresponding Author: B Thanushah
Acting Consultant Dermatologist, Teaching Hospital,
Batticaloa, Sri Lanka.
Email: thashahnu@yahoo.com
Received : Aug 26, 2021
Accepted : Sep 23, 2021
Published : Sep 30, 2021
Archived : www.jcimcr.org
Copyright : © Thanushah B (2021).
Citation: Thanushah B, Thamilvannan N, Ahilen M, Ahilan S, Chandrarathna SH. Primary Herpes Simplex Viral infection of bilateral nipples and areolae with reactive arthritis: An uncommon presentation of a common disease. J Clin Images Med Case Rep. 2021; 2(5): 1335.
Introduction
Herpes Simplex Viruses (HSV) are members of the Herpesvirales, subfamily Alphaherpesvirinae. They are linear double standard DNA viruses. Skin manifestations caused by HSV is one of the commonest cutaneous infectious diseases encountered during dermatology practice. It affects most people on one or more occasions during their lives. Cutaneous presentations are characterized by painful localized grouped vesicles. Type 1 HSV is mainly associated with orofacial involvement. Type 2 HSV is mainly associated with anorectal involvement. However, HSV infection can occur almost any area of skin or mucous membrane.
Characteristic nature of this virus is its dormant stage after primary infection. After the primary episode of infection, HSV resides in a latentstate in spinal dorsal root ganglia. During a recurrence, the virus follows the nerves that supplies cutaneous sensation onto the skin or mucous membranes, where it multplies, causing the clinical lesion. After each attack, it enters the resting state. During an attack, the virus can be inoculated into new sites of skin, which can then develop blisters as well as the original site of infection.
Primary attacks of Type 1 HSV infections occur mainly in infants and young children. Type 2 HSV infections occur mainly after puberty and are often transmitted sexually. HSV is transmitted by direct or indirect contact with person with active herpes simplex, which is infectious for 7–12 days. Asymptomatic shedding of the virus in saliva or genital secretions can also lead to transmission of HSV, but this is infrequent, as the amount shed from inactive lesions is less than when it is active. The incubation period of the infection is 2–12 days.
Minor injury helps inoculate HSV into the skin. For example: A thumb sucker may transmit the virus from their mouth to their thumb, HSV involving nipple is seldom reported in the literature.
Herein we present a case of primary HSV infection involving both nipples associated with reactive arthritis in a lactating mother.
Case report
A 25-year-old female from Batticaloa, admitted to a medical ward with the history of joint pain involving both shoulders, knees and hips associated with painful tiny vesicles involving both nipples for 4 days duration. She was otherwise healthy with no significant past medical illnesses. She had no fever or other systemic complaints.
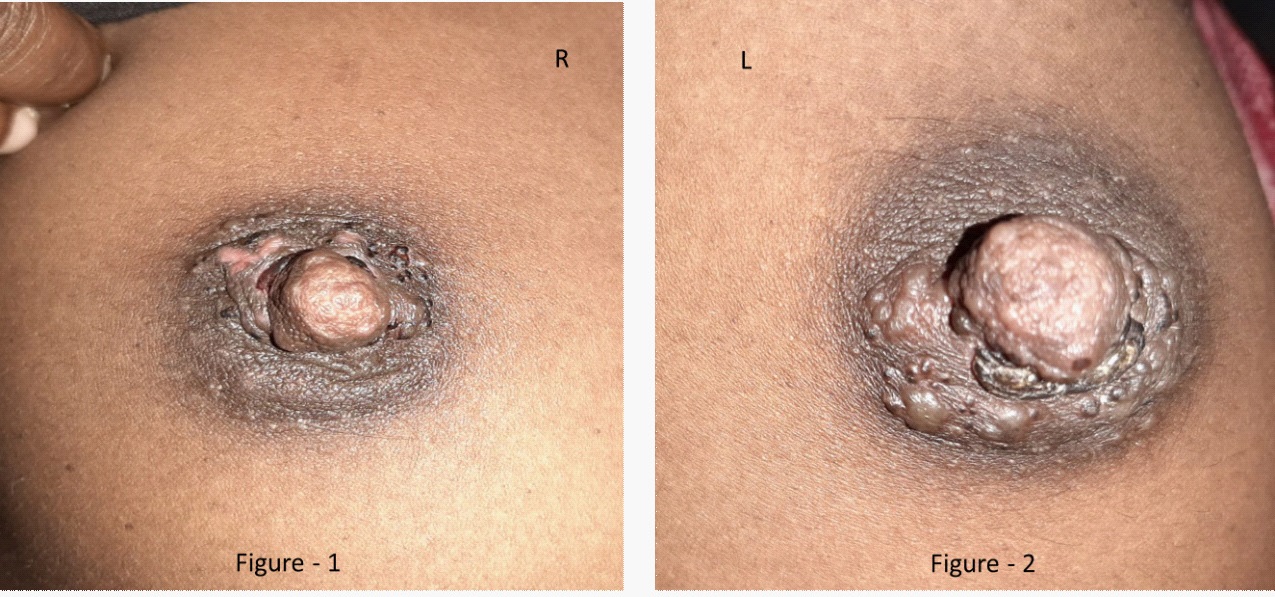
Examination revealed tender mildly swollen bilateral knee joints with limitation of movements due to pain and swelling. No swelling or tenderness were found over shoulders and hips. There were tender slightly erythematous and erosive cluster of vesicles noted localized over both nipples and confined to areolas. But there weren’t any clinical evidence of mastitis and axillary or inguinal lymphadenopathy (Figure 1&2).
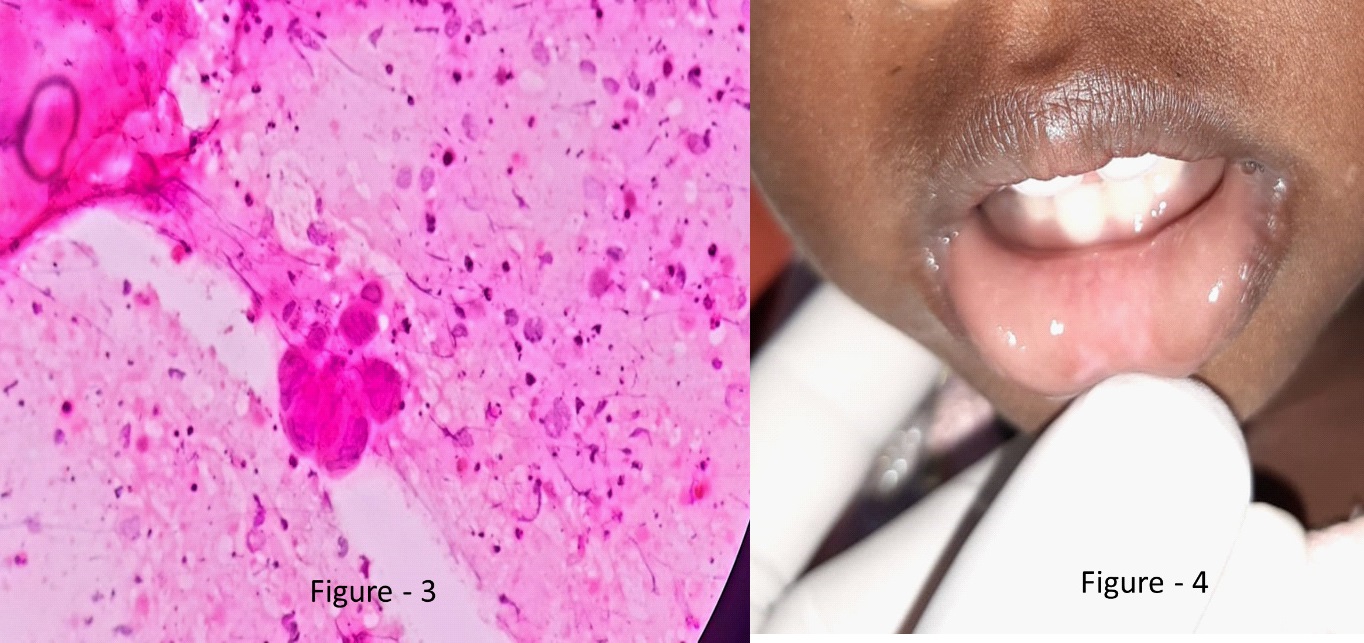
Interestingly on further questioning, she admitted that she was a breastfeeding mother of a 1 ½ years old child and child had had painful lip erosions 10 days prior to her presentation. Baby’s lip erosions were healed at the time of admission (Figure 4).
Investigations revealed mild neutrophil leukocytosis with white cell count of 14×103 mm3 and neutrophils 82%. ESR was 92 and CRP 22 and mildly elevated liver enzymes. Rheumatoid factor and Anti-nuclear antibody were negative. Ultrasound scan of the abdomen was normal.
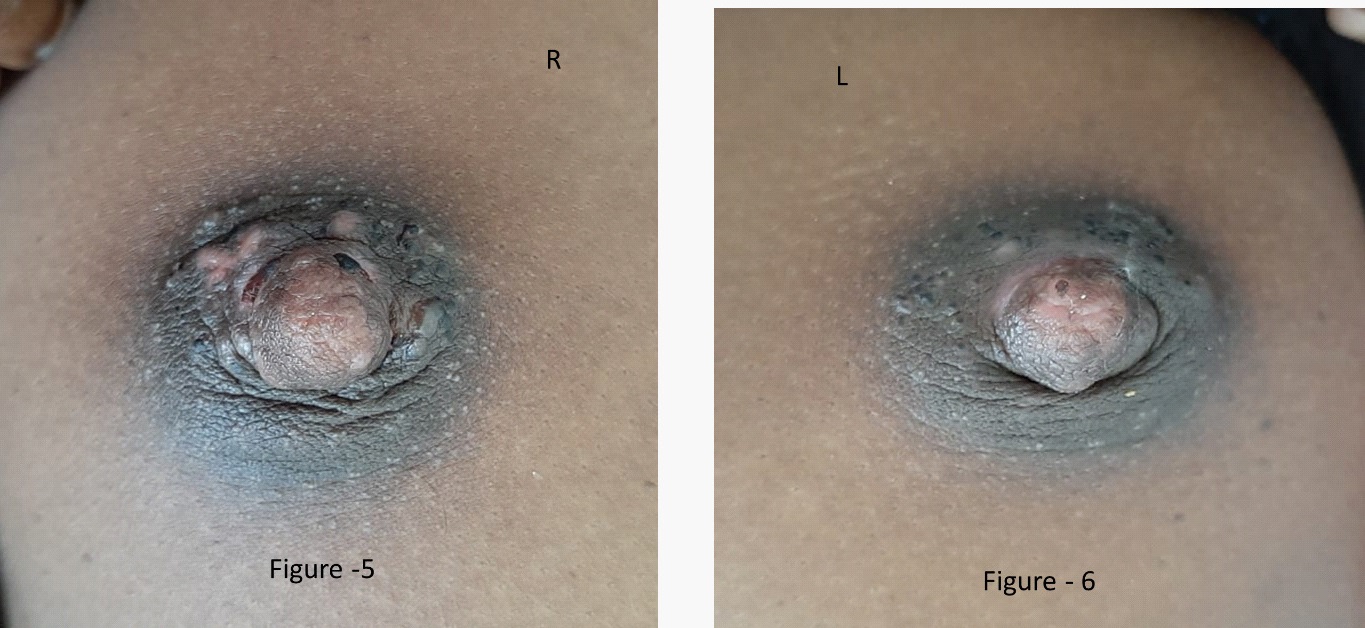
Tzanck smear done from vesicles showed multinucleated giant cells (Figure 4). Clinical diagnosis of Primary HSV involving both nipples with reactive arthritis was made based on her history, examination, and investigations. She was started on oral acyclovir and analgesics. She made a complete resolution of clinical symptoms and normalization of the blood parameters after 5 days of treatment (Figure 5 & 6).
Discussion
HSV infection caused by HSV I and II serotypes commonly manifest as orolabial and anogenital vesicles and erosions, respectively. HSV shows varies of clinical manifestations range from uncomplicated isolated mucocutaneous lesions to severe disseminated life-threatening HSV infection in all age groups. The course depends on the age of the patient, the immune status of the host, the site of infection, the individual's previous immunity to autologous or heterologous viruses, and the antigenic type of the virus.
HSV infection of the nipple and periareolar area is exceptionally rare and probably underrecognized. It is usually unilateral and does not recur. Source of infection of nipple HSV is often from autoinoculation, sexual transmission, or breastfeeding.
Only few reported cases of HSV infection of nipple available in the literature, whereas HSV involving bilateral nipples is not reported so far. We report this first case of Primary HSV involving both nipples and areolae with reactive arthritis in breastfeeding mother who acquired the infection by inoculation of the virus from gingivostomatitis of the baby.
Diagnosis often clinical, and bed site test Tzanck smear aids rapid diagnosis. Immunohistochemistry enables viral identification and is not freely available in all centers. Treatment relies on early commencement of oral antiviral therapy such as acyclovir, famciclovir or valaciclovir [1-5].
Early and prompt diagnosis is necessary to prevent complications like mastitis and encephalitis.
References
- El Hayderi L. Herpes Simplex Virus Infections of the Nipple. Open Dermatol J. 2012; 6: 29–32.
- Oiso N, Tsuruta D, Imanishi H, Amatsu A, Kobayashi H, Kawara S, et al. Spotted hyperpigmentation: Disfigured melanosomes in melanocytes and keratinocytes. J Eur Acad Dermatology Venereol. 2008; 22: 876–8.
- Barrett ME, Heller MM, Stone HF, Murase JE. Primary herpes simplex virus infection of the nipple in a breastfeeding woman. Cutis. 2016; 97: E10–1.
- Brown H, Kneafsey P, Kureishi A. Herpes simplex mastitis: Case report and review of the literature. Can J Infect Dis. 1996; 7: 209–12.
- Soo MS, Ghate S. Herpes simplex virus mastitis: Clinical and imaging findings. Am J Roentgenol. 2000; 174: 1087–8.