
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A mimic of a STEMI in an elderly male patient at emergency department requiring no stent
Lagath Wanigabadu1*; Jithesh Choyi2; Shahram Ahmadvazi3; Sarah Justice3; Abdalla Khalil2
1 Emergency Department, Maidstone and Tunbridge Wells NHS Trust, UK.
2 Acute Medicine Department, Princess Royal University Hospital King’s College trust London, UK.
3 Cardiology Department, Maidstone and Tunbridge Wells NHS Trust, UK.
*Corresponding Author: Wanigabadu L
Emergency Department, Maidstone and Tunbridge
Wells NHS Trust, UK.
Email: Lagath.Wanigabadu@nhs.net
Received : Sep 01, 2021
Accepted : Oct 07, 2021
Published : Oct 14, 2021
Archived : www.jcimcr.org
Copyright : © Wanigabadu L (2021).
Abstract
An elderly male patient presented with chest pain and an initially abnormal ECG, with 1 mm ST elevation in the lateral leads. As he was pain free on arrival, he was treated locally, where a coronary angiography showed no stenosis and echocardiography showed apical ballooning which indicated Takotsubo Cardiomyopathy (TC). On further questioning, he indicated he has been worrying about his son’s financial circumstances. Patients with TC can present with a history and an ECG resembling and indistinguishable from ST-elevation Myocardial infarction or other types of Acute Coronary Syndrome (ACS).
Citation: Wanigabadu L, Choyi J, Ahmadvazi S, Justice S, Khalil A. A mimic of a STEMI in an elderly male patient at emergency department requiring no stent. J Clin Images Med Case Rep. 2021; 2(5): 1361.
Introduction
As Ischemic Heart Disease (IHD) remains the leading cause of mortality worldwide, patients presenting with symptoms and signs indicative of an acute coronary syndrome are admitted to hospital and treated as such. However, a significant proportion of these patients do not have a flow-limiting lesion on coronary angiography. There is an ever-growing knowledge of myocardial infarction with non-obstructive coronary arteries (MINOCA), which is estimated at ~10% of Acute Coronary Syndrome ACSs [1].
Takotsubo cardiomyopathy, which was until very recently classified as MINOCA, has been recognised as one of the underlying conditions mimicking ACS, estimated to account for ~2% of all ACS admissions [2].
Case presentation
A 76 years old male presented to the emergency department with a central ‘’Heavy’’ chest pain for 4 hours which was associated with diaphoresis and emesis and developed just after finishing his routine walk. The pain eased spontaneously but he was rushed to the hospital by the ambulance crew. On admission, the patient was pain free.
He was on multiple medications, namely doxyphyllin 400 mg Once Daily (OD), metoprolol XL 25 mg OD, valsartan 40 mg OD, torsemide 10 mg OD, ivabradine 5 mg OD and atorvastatin 20 mg OD.
His past medical history include hypertension and gastrooesophageal reflux disease and was on Ramipril 10 mg once a day, Aspirin 75 mg once a day and Omeprazole 20 mg once a day. He was previously treated for prostate cancer and currently in remission. He denied any drug allergies. He has no family history of cardiac diseases and is a teetotaller. He lives alone and is independent with all activities of daily living and walks 5 miles regularly.
On examination, he looked well and was pain free at presentation. His early warning score was zero with a heart rate was 66 bpm and pulse was regular. His blood pressure was 145/96 mmHg. 1st and 2nd heart sounds were noted with no murmurs. His Jugular venous pressure was not raised and didn’t have any pedal oedema. His oxygen saturating 95% on room air. His lungs were clear and his abdomen was soft. The patient was alert with no focal neurological deficit.
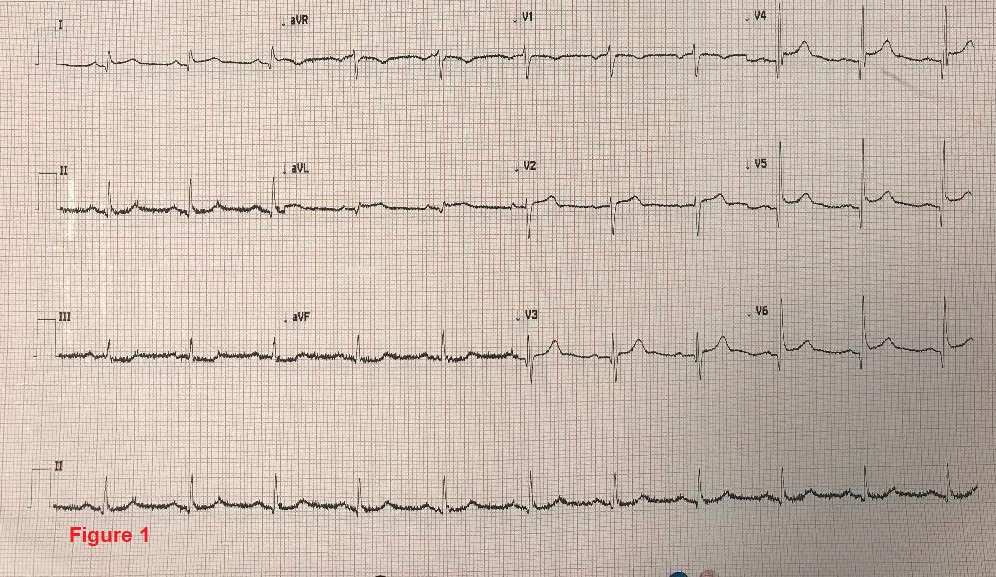
The full blood count, renal functions, liver functions and coagulation profile were within the normal range. Venous blood gas on admission was normal except lactate of 2.3. Initial ECG on admission showed concave 1 mm ST lead elevation in lead V4 – V6 (Figure 1).
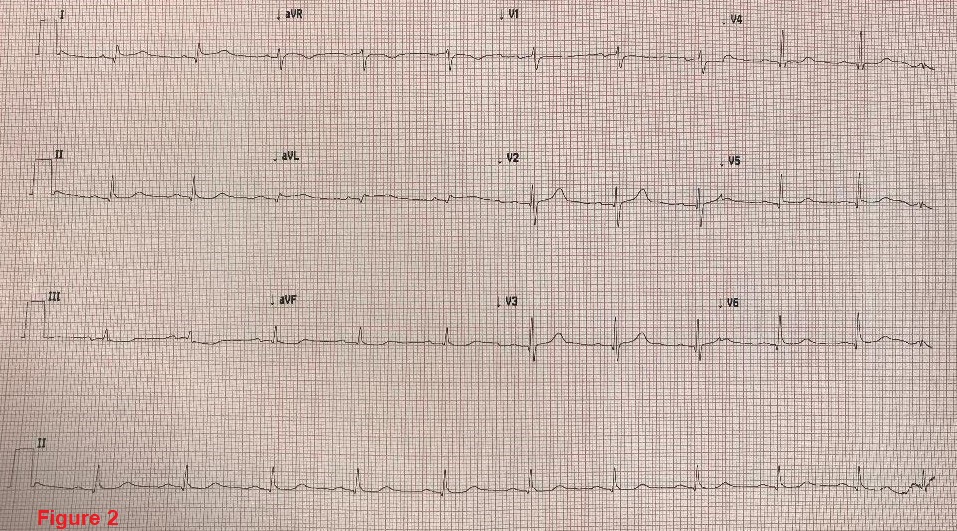
The ECG after 6 hours was normal (Figure 2).
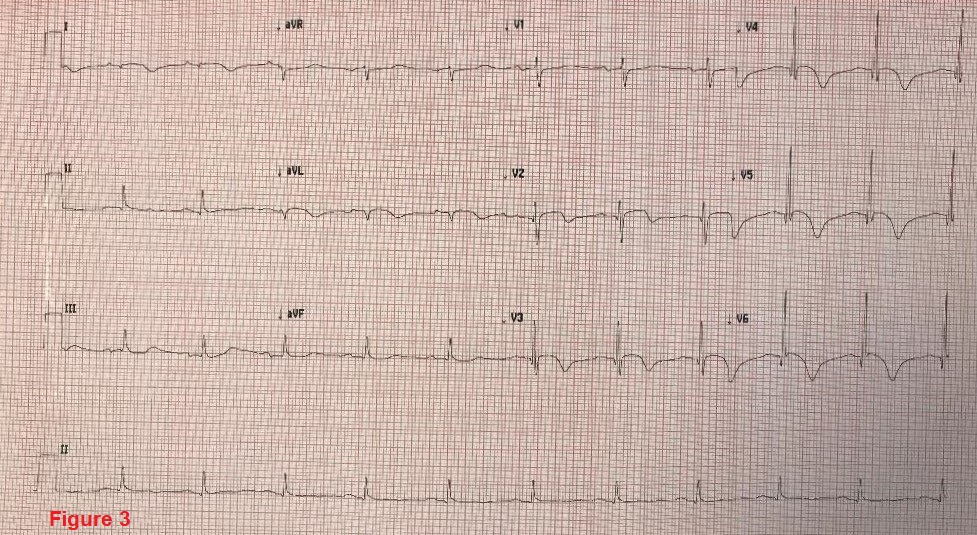
Repeated ECG 18 hours after the admission showed deep T wave inversions in leads V2 – V6, lead I and AVL (Figure 3).
The initial cardiac enzyme done on admission was 4 hours from the onset of pain and Troponin T was 2637 ng/litre (<14 ng/litre is normal). Troponin T was repeated after 3 hours and was 2687 ng/litre which was less than a 2% rise.
Lateral ST Elevation Myocardial Infarction was suspected and the patient was discussed with the regional primary coronary angioplasty centre. As patient was pain free, it was decided to manage him locally. The patient was prescribed Aspirin 300 mg and Clopidogrel 300 mg orally and Fondaparinux 2.5 mg subcutaneously.
An echocardiogram revealed a severely impaired left ventricular systolic function with an ejection fraction of 20-30%. Diastolic function was grade 2. Regional wall motion abnormalities noted in the left ventricle with contraction of the basal segment and rest being akinetic. No significant valvular abnormalities noted and moderate pulmonary hypertension was noted with pulmonary artery systolic pressure of 62 mmHg (Normal range 18-25mmHg).
On further questioning, the patient revealed that in the last few days he has been worrying about his son’s economic crisis.
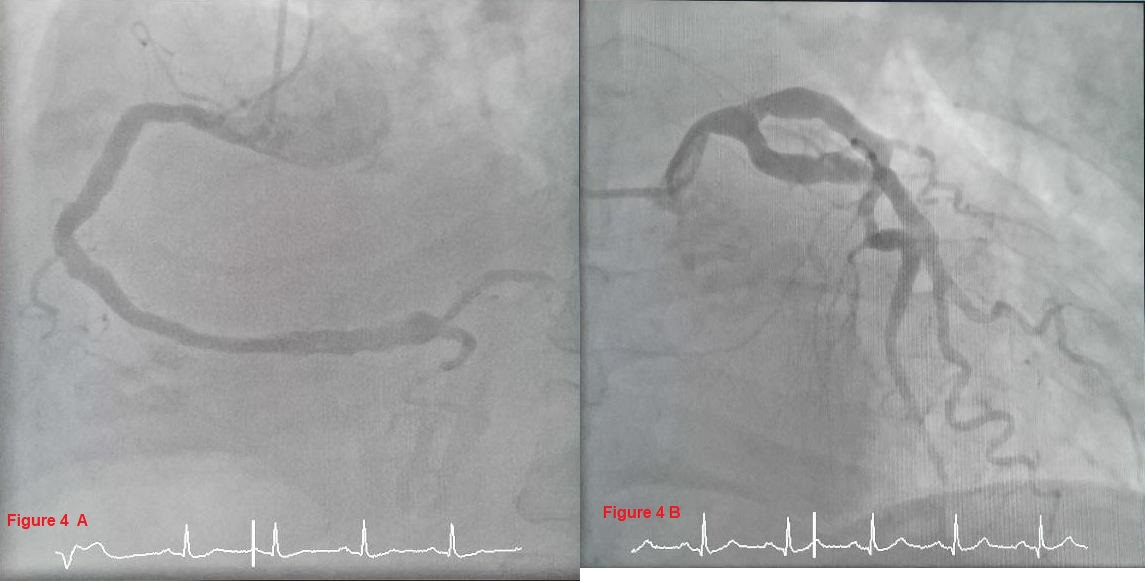
An angiogram was performed 12 hours after admission which revealed generally large calibre coronary arteries with plaque disease (Figure 4).
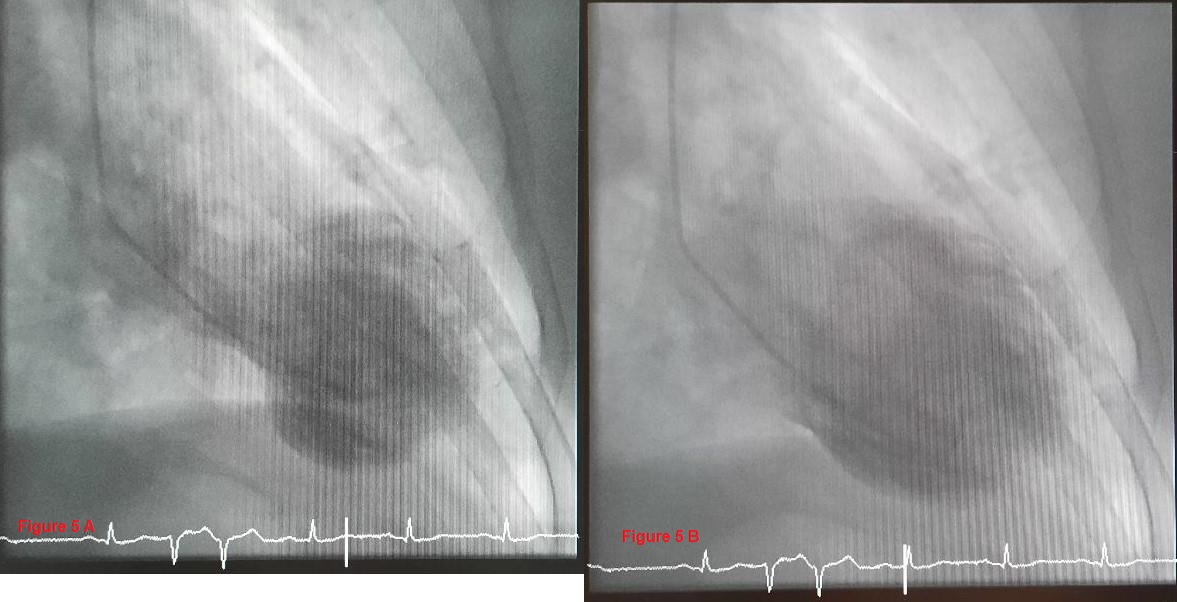
The left ventricle demonstrated apical ballooning in keeping with Takotsubo Cardiomyopathy (Figure 5).
During the hospital stay, patient remained marginally hypotensive and bradycardic, limiting further medication to be initiated. Therefore, only ACE inhibitor (ACEi) was started. During the hospitalisation, he developed acute breathlessness and had clinical signs of fluid overload with bi-basal crepitations, as well as chest X-ray evidence of pulmonary oedema, which was managed with intravenous and then oral diuretics. He also had a brief episode of paroxysmal atrial fibrillation, with a CHADS2 VAsc score of 3 and he was anticoagulated.
After 5 days of hospital stay, he was discharged on Apixaban 5 mg twice a day, Bumetanide 0.5 mg in the morning, and Ramipril was reduced to 1.25 mg at night. At the time of discharge, he was back in sinus rhythm and was haemodynamically stable.
He had a repeat echocardiogram in 3 months which demonstrated normal left ventricular systolic function with an ejection fraction of 55%. He has been continuing his regular 5 miles walk with no symptoms.
Discussion
Takutsubo Cardiomyopathy, since its first recognition in Japan nearly 30 years ago, has become more widely recognized. It is estimated that ~2% of patients admitted with a suspected ACS. This is likely an under-diagnosed, especially when we consider that patients with milder symptoms may not seek medical attention [3].
The term Takutsubo is a Japanese word, describing the resemblance of the left ventricular appearance of the majority of such cases to a pot with a narrow neck and a round bottom used to catch octopuses. Our understanding of the pathophysiology of TC is rather limited and various hypotheses have been suggested, with catecholamine storm cardiotoxicity gaining more weight and TC induced by epinephrine has been reported [4].
While the majority (~90%) of patients are post-menopausal females, it can be seen in other ages and males, as illustrated in our case report.
Patients with TC may present with sudden onset chest pain and an ECG indistinguishable from a ST Elevation Myocardial Infarction (STEMI) in as many as 50% of the patients among a wide range of ECG findings such as ST depression and T wave abnormalities, as well as an entirely normal ECG [5].
While a careful history might elicit recent emotional or physical stress, it does not exclude a true STEMI and local primary angioplasty activation and discussion should take place. While ECGs in most cases show some degree of abnormality, normal ECG has also been reported. There have been several criteria produced, and recently the International Takotsubo Diagnostic Criteria (InterTAK Diagnostic Score) have proposed one, to arrive at a consensus [6,7].
Essential to the diagnosis is a transient left ventricular dysfunction, often in the shape of apical ballooning, although many other subtypes have been reported. In the majority of the cases, the wall motion abnormality does not follow an epical coronary artery distribution, and there is no significant coronary artery disease. Patients often have raised cardiac markers, whereas brain natriuretic peptide levels are significantly raised. The prognosis in majority of cases is very good but complications such as acute Heart Failure (HF), Left Ventricular Outflow Tract Obstruction (LVOTO), Mitral Regurgitation (MR), ventricular arrhythmias, systemic thromboembolism, and cardiogenic shock have been reported and recurrent cases have also been reported. The mortality appears to be more than previously understood and similar to patients with an acute coronary syndrome, with in-hospital mortality of 5% [8].
There has been no randomised control trial to lead the treatment, but in the majority of uncomplicated cases, standard heart failure treatment with ACEi/Angiotensin II Receptor Blocker and beta-blocker, +/- diuretics and mineralocorticoid receptor antagonist are used.
Conclusion
Takutsubo cardiomyopathy can mimic STEMI and can be indistinguishable from STEMI. While a careful history may elicit stress, physicians should follow local pathways for activation of primary angioplasty.
It is more common in post-menopausal females with recent emotional or physical stress, but can be seen in males of all ages.
Most patients have significant but transient left ventricular dysfunction with apical ballooning.The prognosis in the majority of cases is very good but several complications, such ventricular dysrhythmia has been reported. Despite a widely assumed good prognosis, it carries 5% in-hospital mortality [9].
References
- Buono A, Pedrotti P, Soriano F, Veas N, Oliva F, et al. L’infarto miocardico senza ostruzione coronarica significativa (MINOCA): Inquadramento diagnostico, patogenesi, terapia e prognosi [Myocardial infarction with non-obstructive coronary arteries (MINOCA): diagnosis, pathogenesis, therapy and prognosis]. G Ital Cardiol (Rome). 2019; 20: 499-511.
- Yalta K, Ucar F, Yilmaztepe M, Zorkun C. Takotsubo cardiomyopathy and acute coronary syndromes: Are they always mutually exclusive? Indian Heart J. 2018; 70: 326-327.
- Eshtehardi P, Koestner SC, Adorjan P, et al. Transient apical ballooning syndrome--clinical characteristics, ballooning pattern, and long-term follow-up in a Swiss population. Int J Cardiol. 2009 10; 135: 370-5.
- Maes S, Dhooghe NSJJ, Schotte H, Cattoir S, Jacobs TF, Van Landuyt K. Takotsubo Cardiomyopathy Induced by Epinephrine Infiltration for Liposuction: Broken Heart Syndrome. Aesthet Surg J. 2019; 39: NP431-NP436.
- Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010; 55: 333-41.
- Ghadri JR, Wittstein IS, Prasad A, Sharkey S, et al International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur Heart J. 2018; 39: 2032-2046.
- Templin C, Ghadri JR, Diekmann J, Napp LC, et al.Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med. 2015; 373: 929-38.
- Tornvall P, Collste O, Ehrenborg E, Järnbert-Petterson H. A CaseControl Study of Risk Markers and Mortality in Takotsubo Stress Cardiomyopathy. J Am Coll Cardiol. 2016; 67: 1931-6.
- Kim H, Senecal C, Lewis B, Prasad A, Rajiv G, et al. Natural history and predictors of mortality of patients with Takotsubo syndrome. Int J Cardiol. 2018; 267: 22-27.