
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The moderated mediation role of malaria knowledge and household income in the relationship between insecticidetreated mosquito nets and malaria prevalence
Tao Hong; Mohammed Aliye*
School of Management, Harbin institute of technology, Harbin P.R China, 150001.
*Corresponding Author: Mohammed Aliye
School of Management, Harbin institute of technology,
Harbin P.R China, 150001.
Email: aliyemohammed@yahoo.com
Received : Sep 16, 2021
Accepted : Oct 22, 2021
Published : Oct 29, 2021
Archived : www.jcimcr.org
Copyright : © Aliye M (2021).
Abstract
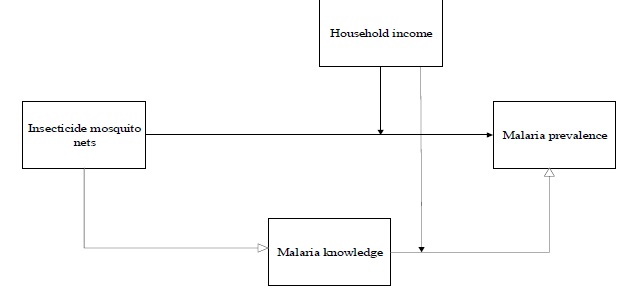
Objectives: The study was premised on the notion that insecticidetreated mosquito nets are positively related to malaria prevalence, and that knowledge mediates the relationship between insecticide-treated mosquito nets and malaria. Furthermore, household income was hypothesized to have a moderating effect on the direct and indirect relationships (through malaria knowledge) between insecticide-treated mosquito nets and the prevalence of malaria.
Methods: The hypothesized relationships were examined using panel data collected from ten regions of Ethiopia during 2011 – 2015. Structural equation modeling and the random effect model were used to test the hypotheses. Statistical analyses were performed using Stata version 13.0.
Results: The results were consistent with our proposed hypotheses, showing a significant relationship between the research variables. The findings suggest that malaria knowledge contributes to improving the relationship between insecticide-treated mosquito nets and malaria prevalence. A positively significant indirect effect (β = 0.47, p = 0.003) as well as direct effect (β = 0.28, p = 0.001) was revealed in the study. Furthermore, a positive impact of household income in strengthening the relationship between insecticide-treated mosquito nets and malaria through knowledge reported, with a considerable value (β = 0.13, p = 0.000). The result also reveals differences in the outcome of malaria prevalence at different levels of household income category, where the indirect effect of insecticide-treated mosquito nets on malaria prevalence via malaria knowledge was positive and significant for households under the second-level income category (β = 0.15, p = 0.000). Conversely, the indirect effect of insecticide-treated mosquito nets on malaria prevalence via malaria knowledge was negative for the high level-income category (β = -0.14, p = 0.022). Besides, insignificant and negative relationships were reported for households under low-level income categories (β = 0.024, p = 0.539).
Conclusion: The findings are potentially useful for the health sector to ensure success in infectious disease prevention and control, particularly malaria, and to explain how various factors contribute to the relationship.
Keywords: malaria; insecticide-treated mosquito nets; malaria knowledge; household-income; structural equation modelling.
Citation: Hong T, Aliye M. The moderated mediation role of malaria knowledge and household income in the relationship between insecticide-treated mosquito nets and malaria prevalence. J Clin Images Med Case Rep. 2021; 2(5): 1391.
Introduction
Malaria is a global health problem that poses an enormous burden on health systems and the broader economy, particularly in Africa [1,2]. About 214 million malaria cases and 438,000 deaths were reported in 2015, where 90% of which occurred in African [3]. In 2016, malaria caused 216 million cases and 445000 deaths worldwide. Africa is the most affected continent, contributing 90% of the global malaria cases and 91% of these deaths [4]. Moreover, 212 million cases of malaria and 429000 deaths were reported [5], where 92% of the deaths occurred in Africa, followed by South-East Asia (6%) and Eastern Mediterranean Region (2%).
Net distribution is an integral part of a selective vector control strategy for malaria protection, having a significant impact on malaria [4]. Regular use of ITNs reduces the overall death risk by 20% and the number of clinical malaria episodes in young children by 50% [6] and is used as preventive measures against malaria [7]. Moreover, ITNs and IRS are recommended as the cornerstone of the strategy for malaria control [8]. Ethiopia implemented malaria control interventions, such as ITNs, IRS, and environmental management to fight against malaria [9]. Accordingly, the impressive decline in child mortality has been attributed to the implementation of vector control interventions [10]. The decline in malaria morbidity and mortality was also reported [11]. However, malaria remains a major health problem in Ethiopia [12]. Malaria is yet prevalent every rainy season, especially in the lowland areas of Ethiopia [13]. The health minister has planned to cut malaria morbidity and mortality by 50% in 2015; however, the goal was not attained [14]. Weak public awareness and practice towards malaria prevention and control alternatives, persistent misunderstandings about malaria, and unsatisfactory malaria control practices were reported [15]. Moreover, respondents who were knowledgeable about IRS compared to respondents who were not knowledgeable are reported as less likely to take up IRS. Where respondents who knew the reason for spraying (to kill mosquitoes) and knew the frequency of spraying (after every six months) were considered knowledgeable about IRS, although gaps in knowledge and fears on health effects were identified as a challenge [16].
Previous studies investigated knowledge, attitudes, and practices related to malaria prevention options such as ITNs [17-21] — these studies provide information on malaria prevention and mostly relied on the assessment of knowledge about malaria with specific study populations, but they did not explore the socio-economic aspects and knowledge of households to explain the relationship. Studies indicate that Ethiopian communities are not well aware of the multi-dimensional challenges of the disease despite the bitter facts of malaria, misuse of ITN, limited knowledge of malaria transmission, and unsatisfactory malaria control methods were reported [22-25]. Therefore, it is pertinent to consider the impact of knowledge on strategic interventions to prevent the spread of the disease. To the best of our knowledge, none of the previous studies considers the role of malaria knowledge in the relationship between ITNs and malaria. In addition, no previous study tested the moderating role of household income in strengthening the relationship between strategic interventions and malaria based on malaria knowledge.
Furthermore, this study aimed to test whether the relationship between ITN and malaria prevalence varies with different levels of household-income categories. Our research, therefore, measured the influence of malaria knowledge and household income in the relationship intending to investigate the effect of ITN on malaria prevalence, with malaria knowledge and household income playing a moderated mediation role. Finally, we conducted our analyses using structural equation modeling and the random effect model of the panel data estimation technique.
Theoretical background: The mediating role of malaria knowledge between strategic interventions and malaria control
The conceptual model we draw on to establish the relationship between ITN and malaria prevalence is the health belief model (HBM). According to the model, it is not only the subjects’ beliefs that matter but also their knowledge and attitude [26]. Personal perception is also influenced by the whole range of interpersonal factors affecting health behaviors. Differences in malaria knowledge have been shown to cause discrepancies in tackling malaria disease [27]. The HBM hypothesizes that health-related action depends on three classes of factors [28,29]. The first class is the existence of sufficient motivation (or health concern) to make health issues salient or relevant. The second class is the belief that one is susceptible to a severe health problem, which is often viewed as a perceived threat. The third class is the belief that following a particular health recommendation would be beneficial in reducing the perceived threat at a subjectively acceptable cost. The model remains the most widely employed theory of health behavior [30] and the most commonly recognized approach in the health field [31]. The theory is based on the understandings that a person will take health-related action if the person believes they are susceptible to the condition (perceived susceptibility); the condition has serious consequences (perceived severity); taking action would reduce their vulnerability to the condition (perceived benefits), and these benefits outweigh the cost of taking action (perceived barriers) [32]. The response is accepted more easily if the person is exposed to factors that prompt measures (cues to action) and is confident in their ability to act successfully (self-efficacy) [33].
Insecticide-treated mosquito nets (ITNs) were identified as the most effective malaria prevention approach [21] and have decreased malaria incidences by 50% in various settings and malaria mortality rates by 55% in children under five years old in Sub-Saharan Africa [4]. The perceived benefit and barrier of the HBM do matter on the user preferences. Factors associated with taking up IRS were socio-economic status and related factors. The success of malaria control intervention requires the regular use of ITN to prevent malaria and mosquito bites [34]. Inadequate knowledge about malaria and lack of ITNs observed [35], which is one of the challenges for the appropriate use of these interventions. Higher use of bed net was reported in the rainy season with 80%, vulnerability to high mosquito areas, and access to a health facility as contributing factors for use with better than the one far from a health facility [36]. Similarly, pregnant women were more likely to implement malaria preventive actions if they lived within five kilometers of clinics, were satisfied with available health services, and were knowledgeable about the malaria preventive measures [37]. Awareness creation about the program is critical to engage in preventive and control measures [38], which occurred through iterative actions to strengthen the responsiveness of the population to malaria prevention. Better utilization of ITN reported among the community who understand infection and transmission methods of malaria [39]. Besides, differences in the level of malaria knowledge have been shown to cause differences in tackling malaria [27] due to differences in intervention use. Similarly, respondents who were knowledgeable about malaria control intervention, such as IRS, were more likely to accept the spray compared to those who are not knowledgeable [16].
Moreover, better ownership and use of ITNs were reported by the communities with good knowledge than unknowledgeable ones [7]. The influence of knowledge gaps and a wrong perceptions were also reported affecting the use of insecticidetreated nets to protect malaria [40]. Likewise, lack of knowledge about malaria reported having to hinder any measures of personal protection [41]. Health motivation is the central focus of the HBM to evoke health concerns, for example, living in a malaria-prone area and the possibility of contracting the disease [33,42]. Results also indicate that antenatal care (ANC) services were a crucial factor for knowledge of malaria where women who reportedly received ANC are 3.9 times more likely to have accurate knowledge of malaria when compared to those who did not use skilled ANC services [43], and their educational level was significantly associated with this knowledge. However, myths and misconceptions about malaria were stated, and of 49.3% that owned insecticide-treated bed nets (ITNs), only 18.2% used them consistently. Ethiopian study reported a low level of caretaker’s knowledge regarding mosquito bites to cause malaria by 66.4% of respondents. It was quite heterogeneous by localities (ranging from 26.1% to 89.4%) and altitude. Being low in high altitude and low in transmission areas (p < 0.05). 69.3% of the children slept under LLIN in the previous night, of malaria-related knowledge items, only knowledge of LLIN was associated with net use [24].
The present study employed the theory of the HBM, holding that the independent variable (ITN) should influence the dependent variable (malaria prevalence) through mediating variables (malaria knowledge) and moderating variables (household income). Thus, when a person has good knowledge, having a positive attitude, and has access to intervention tools, they are more likely to practice preventive measures. Additionally, a person who has sufficient income and is knowledgeable about the program is more likely to access the interventions to protect from malaria. Thus, mediation occurs when the causal effect of an independent variable (X) on a dependent variable (Y) is transmitted by a mediator (M) [44], while the moderating variable is the interaction terms at which the strength of the relationship between two variables is dependent on a third variable. So, the HBM is a tool used to explore the perceptions and beliefs about malaria and the use of strategic interventions such as ITNs [45]. Accordingly, the theory-guided the study in establishing the relationship between the explanatory variable (ITNs) and the outcome variable (malaria-prevalence), and we examined whether household income has a moderating effect on a direct and indirect relationship (through malaria knowledge). Based on these logical arguments and previous literature, we hypothesize that:
H1
. An insecticide-treated mosquito net is positively and significantly related to malaria prevalence.
H2
. An insecticide-treated mosquito net is positively associated with malaria knowledge.
H3
. Malaria knowledge is positively related to malaria prevalence.
H4
. Malaria knowledge links insecticide-treated mosquito
nets to malaria prevalence.
The moderating role of household income on the relationships between strategic interventions and malaria control
Effective preventive action is the outcome of public health program, which resulted in the access of the community to malaria control interventions. Malaria morbidity and mortality were associated with people’s socio-economic status [46] and remain the leading cause of morbidity and mortality in low and middle-income countries [47,48]. The burden of chronic disease is reported to increase in low and middle-income countries, where it constitutes multiple burdens along with infectious diseases [49]. The notion coincides with the finding which reported a positive association between household income and ITN to use to protect malaria [50]. Furthermore, the quality of life and health status is linked to the economic, income, and educational status of residents [51]. In addition, malaria elimination is recorded from high-income countries, while it is a challenge for low and middle-income countries [52]. Moreover, the association between income and malaria preventive action was reported, where higher income groups are two times more likely to practice than low-income groups [53]. Access to the intervention was influenced by household income [54]. Although ITN is suggested as a means of malaria reduction, communities with large families and low incomes are more affected by malaria disease [55]. Furthermore, income level, age, education, and occupation was reported as a significant predictor variable for knowledge of malaria and intervention use [56]. Also, despite the reported reduction in prevalence from 60 to 20% for cases at the local health center, misconceptions about the cause of malaria and misuse of preventive strategies were noted, where poverty was deemed to be a contributing factor to malaria transmission [57].
Moreover, the positive association of household income on the use of ITNs to protect against malaria was reported [50]. The study also revealed that the quality of life and health status are basically linked to the economic, income, and educational attainment of residents [51]. Malaria elimination from highincome countries was reported, though it is a challenge for low and middle-income countries [52]. Likewise, the study revealed the association between income and practice of malaria preventive actions, where higher income groups are more likely to practice two times higher than low-income groups [53]. Besides, the report shows access to intervention is influenced by household income [54]. Moreover, malaria was reported as the leading cause of morbidity and mortality in low and middle-income countries [47,48]. Similarly, the burden of chronic diseases is increasing in low and middle-income countries, where it constitutes multiple burdens along with infectious diseases and other health problems [49]. Similarly, though ITN was suggested as a means of a malaria-reducing approach, the communities with large families and low incomes were reported to be more affected by malaria disease [55]. Incremental improvements in socio-economic development, infrastructure, health services, housing, etc., have been reported to contribute to decreases in the malaria reproduction rate and improve the possibilities for malaria elimination over a longer time [27,58]. The study in Kenya shows; age, marital status, occupation, and income levels were the significant determinants of IRS utilization among the rural communities [56]. The other study also showed age, educational level, occupation, and income levels were significant predictor variables for knowledge about malaria and using IRS as a control tool [56]. Also, the mass distribution of insecticide-treated net neither showed community-wide benefit nor influenced the Spatio-temporal clustering of malaria. Though proved to be protective at the individual level, sleeping under the insecticide-treated nets was influenced by gender, age, and proximity to the vector breeding site, lack of convenient space to hang more than one net was reported as a challenge. Hence, we propose the following hypothesis:
H5 . Household income moderates the strength of the direct relationship between insecticide-treated mosquito nets and malaria prevalence, such that the relationship will be stronger for a better income household than those who are poor households.
H6 . Household income moderates the mediated relationship between insecticide-treated mosquito nets and malaria prevalence via malaria knowledge, in such a way that the strength of the mediated relationship will be different for different income level categories.
Materials and methods
Selection of sample and data
Under the objective of investigating the moderation mediation role of malaria knowledge and household income in the relationship, the author evaluated data from the Ethiopian national malaria indicator survey (EMIS) and health and healthrelated indicators, that obtained from the Federal Ministry of Health, Ethiopia fielded from 2011 to 2015 empirically. The data are collected by the Ethiopian Public Health Institute/Ministry of Health collaboratively with Central Statistics Agency (CSA), US President’s Malaria Initiative (PMI), United Nations Children’s Fund (UNICEF), Malaria Control and Elimination Partnership in Africa (MACEPA/PATH), Malaria Consortium (MC)- Ethiopia, World Health Organization (WHO), and ICAP. The data contains extensive details about malaria and related indicators on an annual basis. All malaria epidemic regions of the country are included in the study and the data are secondary panel data containing 50 observations for final review after condensing as suitable. All relevant variables for the current study were identified. Accordingly, malaria (outcome variable), insecticidetreated mosquito nets (independent variable), the income of the household (moderating variable), and malaria knowledge (mediating variable) were selected for the current study.
Analysis
Stata version 13.0 software package was used for statistical data analysis. The insecticide-treated net was used as an intervention strategy for malaria protection, and malaria knowledge was found to mediate the relationship. Household income played a moderating role, and we evaluated malaria prevalence as an outcome effect. We followed a two-step approach to conduct the analysis and deduce the results — the principal component analysis was used to condense variables given by multiple indicators. We tested the theoretical framework in two steps. First, the proposed linear relationship among the study variables and the mediating effect are examined at once in the same model (hypotheses 1-5). Second, the proposed moderator “household income” was integrated into the model to test whether the direct and indirect relationship (via malaria knowledge) between ITN and malaria prevalence varied according to different levels of household income (hypotheses 6). The significance of the study and the corresponding 95% confidence interval was determined using Wilson’s test. We used a z-test to verify the statistical significance of the study variables for the outcome variables and the mediating and moderating effect of malaria knowledge and household income in the relationship. The coefficient was used to evaluate the mediation of malaria knowledge and moderation of household income via knowledge on ITN-malaria prevalence relationships. All variables and correlations were found to be significant if (p<0.05)
Empirical models
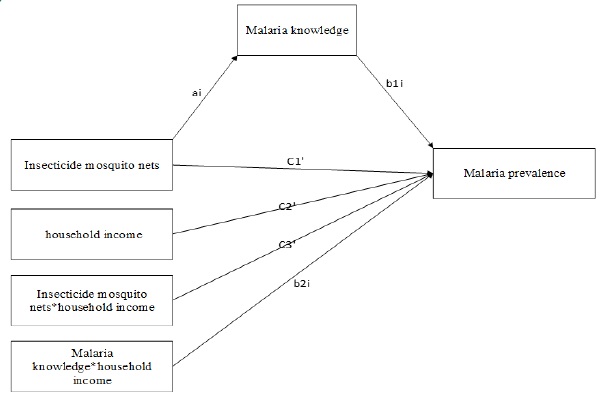
Dependent variables, i.e., malaria prevalence, independent variable, i.e., insecticide-treated mosquito nets, mediating variable, i.e., malaria knowledge, and moderating variable, i.e., household income. At the first stage, the author runs descriptive statistics and correlation analysis among the study variables. In the second stage, the author applied the random effect model (REM) regression by splitting the data country-wise and keep the variables, malaria knowledge, and income of the household as a control variable. In the third stage, the author applied structural hierarchal moderation mediation regression. Thus, the model is to explain the links of ITNs to malaria prevalence, knowledge to malaria prevalence, ITNs to malaria knowledge, household income to malaria prevalence, malaria knowledge to household income, as well as household income interaction to malaria prevalence in structural hierarchal moderated mediation regressions. Furthermore, the mediation effect of malaria knowledge in the relationship between explanatory and outcome variables is explained in the model.
The author designed various equations to examine the overall impact of the study variables. Thus, Equation (1) was designed to test the relationship between ITNs and malaria prevalence. Equation (2) was used to examine the effect of malaria knowledge on malaria prevalence. Equation (3) was designed to test ITNs and malaria knowledge relationships to approve the mediational effect. Equation (4) was employed to investigate the moderating role of household income on malaria prevalence. Equation (5) was designed to test the effect of household income on malaria knowledge. Equation (6) was developed to investigate the moderating role of household income in the relationship between ITNs and malaria prevalence through knowledge of malaria, while Equation (7) was used to test the effect of knowledge and income interaction in the relationship between ITNs and malaria prevalence. Finally, the mediating effect of malaria knowledge in the relationship between ITNs and malaria prevalence was investigated in Equation (8). The present research was also measuring the strength of the relationship on the outcome of malaria at different levels of household income category to approve the moderated mediation effect. The model used a log of dependent and independent variables to capture the moderating factors of household income given by multiple indicators through principal component analysis. The following eight equation models were used to test the results of the research hypotheses:
Where MP represents a dependent variable, ITN is an independent variable, malaria knowledge (Know) represents a mediating variable, household income (Income) is a moderating variable, while β represents an estimate of the effect, and represents the error term of the equation [59]. We assessed the moderated mediation effect by disintegrating paths into direct and indirect impact to identify the immediate effect of the variables using the structural equation model [60]. The randomeffect model was used to solve endogeneity and serial correlation; hence it has the advantage of higher efficiency relative to the fixed-effect model (FEM), leading to smaller standard errors of coefficients and higher statistical power to detect effects [61,62]. The moderation and mediation were assessed by disintegrating paths into direct and indirect impact to identify the immediate effect of the variables under the structural equation model [60].
Results
Descriptive analysis
The author has empirically investigated 50 observations from 10 malaria-endemic regions of Ethiopia. Data in Table 1 shows descriptive details, i.e., the means (M), standard deviations (SD), and correlations among the study variables are listed in Table 1. Correlation analysis showed that all of the study variables were positively and significantly associated with each other. All of the significant associations among the study variables were in the expected directions.
Table 1: Descriptive statistics of research variables
|
M |
SD |
Malaria |
ITNs |
Knowledge |
Income |
Interaction |
Malaria pr. |
9.328151 |
0.361 |
1.0000 |
|
|
|
|
ITNs |
11.39936 |
0.536 |
0.5543* |
1.0000 |
|
|
|
Knowledge |
3 |
0.141 |
0.4778* |
0.5918* |
1.0000 |
|
|
Income |
2 |
0.141 |
0.6559* |
0.4964* |
0.7907* |
1.0000 |
|
Interaction |
24.64259 |
2.170 |
0.7059* |
0.6769* |
0.7998* |
0.9632* |
1.0000 |
Note: Malaria pr. represents malaria prevalence, ITNs represent insecticide-treated mosquito nets, knowledge represents malaria knowledge, income represents household income. M represents Mean; SD standard deviation, *p < 0.05.
Testing the direct relationship
The direct relationship between the study variables was tested simultaneously. The results are presented in Table 2. The results showed that a positive relationship between insecticidetreated mosquito nets (ITNs) and malaria was reported (β = 0.28, p < 0.01). Besides, a positive coefficient (β) has had reported in our analysis for all study variables, suggesting a positive relationship between insecticide-treated mosquito nets, malaria knowledge, the income of the household, and malaria prevalence.
Table 2: Results of the direct relationship
|
Equation (1) |
Equation (2) |
Equation (3) |
Equation (4) |
Equation (5) |
ITNs |
0.278** |
0.0523* |
|
|
|
|
(0.0866) |
(0.0288) |
|
|
|
knowledge |
|
|
0.651 |
|
|
|
|
|
(0.417) |
|
|
Income |
|
|
|
0.628*** |
1.655*** |
|
|
|
|
(0.132) |
(0.340) |
Constant |
6.165*** |
2.403*** |
7.374*** |
1.744*** |
6.018*** |
|
(1.083) |
(0.372) |
(1.335) |
(0.301) |
(0.762) |
N |
50 |
50 |
50 |
50 |
50 |
Note: Malaria prevalence is dependent variable, knowledge denotes malaria knowledge, income denotes household income. Standard errors in parentheses *p < 0.05, **p < 0.01, ***p <0.001.
Testing the direct and indirect relationship (hypotheses 1-5)
Recently, the moderation mediation analysis has received great attention in the literature as a useful tool for broadening the theoretical and practical understanding of causal mechanisms and was applied in the present study. The effect of malaria knowledge and household income in the relationship between explanatory variables and outcome variables (insecticide-treated mosquito nets and malaria prevalence) was tested using structural hierarchal regression analysis. The proposed direct and indirect relationships for all hypotheses were simultaneously tested under structural equation modeling. The results are depicted in Table 3. Accordingly, the results showed a significant and direct relationship between insecticide-treated mosquito nets and malaria prevalence (β=0.28, p=0.001), providing support for hypothesis 1. Additionally, insecticide mosquito net is positively related to malaria knowledge (β=0.053, p=0.049), and malaria knowledge positively related to malaria prevalence (β=65, p=0.118), confirming hypothesis 2 and 3. Our result also supports the partial mediation of Judd & Kenny [63], which reported a positive effect of mediating factors on the outcome of malaria. The findings were corroborated by the study report, which showed insecticide-treated mosquito nets as the most preferred strategy for malaria prevention [21]. Other studies also indicate the use of insecticide-treated mosquito nets to protect against malaria among the study communities [19]. Likewise, [54] reported a proper use of insecticide-treated mosquito nets could cut transmission of malaria disease at least by 60% and child mortality by 20%. To further confirm mediation, we used Judd & Kenny Difference of Coefficients Approach, which involves subtractions of the partial regression coefficient obtained [63]. The result showed the indirect effect of insecticide-treated mosquito nets on malaria prevalence through malaria knowledge (β=0.47, p=0.003) was significantly different from zero, with 95%CI. Thus, hypothesis 4 regarding the mediation effect of malaria knowledge was supported.
Table 3: Results of structural equation model path analysis
Structural path |
Coef. |
Std. Er |
Z |
p>z |
[95%Conf.interval] |
|
ITNs ➔ malaria prevalence |
0.28 |
0.086 |
3.21 |
0.001 |
.1078217 |
.4472075 |
Malaria knowledge ➔ malaria prevalence |
0.65 |
0.416 |
1.56 |
0.118 |
-.1651322 |
1.467698 |
ITNs ➔ malaria knowledge |
0.05 |
0.029 |
1.82 |
0.049 |
-0041617 |
.4472075 |
Income ➔ malaria prevalence |
1.65 |
0.339 |
4.87 |
0.000 |
.9894127 |
2.320555 |
Income ➔ malaria knowledge |
0.58 |
0.117 |
4.94 |
0.000 |
.3502223 |
.811466 |
ITNs*Income ➔ malaria prevalence |
0.12 |
0.022 |
5.46 |
0.000 |
.0765954 |
.1624085 |
Know*Income ➔ malaria prevalence |
0.31 |
0.077 |
4.03 |
0.000 |
.1600749 |
.4632444 |
Know*Income ➔ malaria knowledge |
0.16 |
0.021 |
7.86 |
0.000 |
.123759 |
.2060035 |
ITNs➔ knowledge➔ malaria prevalence |
0.47 |
0.096 |
2.94 |
0.003 |
.0935075 |
.4694023 |
Note: ITNs represent Insecticide-treated mosquito nets, knowledge represents malaria knowledge, income represents household income.
As seen in Table 3, the effect of the interaction between insecticide-treated mosquito nets and household income on malaria was positive and significant (β=0.12, P=.000), indicating a moderating effect. Thus, the results supported our proposed hypothesis 4. Regarding the moderated mediation effect, we checked four conditions suggested under Preacher et al. (2007) that needed to be met for the existence of a moderation mediation effect [44]. To establish moderation-mediation, 1) the relationship between the independent variable and the outcome variable should be significant; 2) the interaction of the moderator variable and the mediator variable with the outcome variable should be significant; 3) the mediator variable should be significantly related to the outcome variable, and 4). the magnitude of conditional indirect effect should be different at different levels of household income. The analysis showed that ITN was significantly related to malaria prevalence (β=0.28, p < .001), thus satisfying condition 1. The interaction between malaria knowledge and household income had a significant effect on malaria prevalence (β=0.31, p=0.000), thus meeting condition 2. Malaria knowledge was positively related to malaria prevalence (β=0.65, p=0.118), thus meeting condition 3. See Table 3 for results. These results were consistent with our proposed hypothesis 5. The present study also shows a positive association between the interaction of malaria knowledge and the income of the household on malaria knowledge (β=0.16, p=0.000). Revealing the moderation role of household income on malaria knowledge, in such a way that, economically advanced communities have better program awareness than the poor, this is maybe due to the access to information tools and have better educational status.
Testing the conditional direct and indirect effects (Hypotheses 6)
The consequences of the program on welfare depend on whether it affected mostly the outcome (malaria prevalence) at low, second, middle, fourth, and high-level income categories. It is, therefore, important to investigate at what level of household income the program was effective irrespective of the cumulative function of household income to impact the relations. As we have checked the three conditions for the moderated mediation effect to exist, here we examine the fourth condition. Thus, regarding condition 4, the conditional indirect effect ITNs on malaria prevalence via malaria knowledge was found to be different across different levels of household income. As seen in Table 4, the indirect effect of insecticide-treated nets on malaria prevalence via malaria knowledge was positive and significant (β=0.15, p=0.000) for households under the secondlevel income category. Conversely, for the household with lowlevel incomes, the indirect effect of insecticide-treated nets on malaria prevalence via malaria knowledge becomes insignificant (β=0.024, p=0.539). A significantly negative indirect effect of insecticide-treated nets on malaria prevalence via malaria knowledge is shown (β= -.139, p=0.022) for the high-levelincome category. These results were consistent with our proposed hypothesis 6. See Table 4 for results related to hypotheses 6. These results constitute an example of the differential impact of various income level categories to influence ITNs and malaria relations.
Table 4: Conditional indirect effect of insecticide-treated nets on malaria prevalence.
Income level categories |
Coef. |
Std. Er |
Z |
p>z |
[95%Conf.interval] |
|
Low-level income |
0.024 |
0.039 |
0.42 |
0.539 |
-.0520826 |
.09961 |
Second-level income |
0.154 |
0.042 |
3.69 |
0.000 |
.0720282 |
.2356026 |
Middle-level income |
0.110 |
0.041 |
2.68 |
0.007 |
.0297021 |
.1905831 |
Fourth-level income |
0.073 |
0.035 |
2.04 |
0.041 |
.0029975 |
.1420064 |
High-level income |
-.139 |
0.060 |
-2.29 |
0.022 |
-.2589428 |
-.0199555 |
Discussions
The aim of this work was to shed light on the following interesting yet overlooked concerns. Thus, the study is endeavored to investigate the mediating mechanisms of malaria knowledge between insecticide-treated mosquito nets and malaria prevalence in the public health context. Then it sought to analyze the moderating effect of household income in the relationship between insecticide-treated mosquito nets and malaria prevalence. The success of malaria control intervention requires the regular use of ITNs to prevent malaria and mosquito bites [64]. Knowledge of the people about malaria transmission is an important predictive factor of ITNs utilization [65]. The findings contribute to research on public health in the context of infectious disease prevention and control by conceptualizing and empirically testing the moderated mediation effect of malaria knowledge and household income in the relationship between insecticide-treated nets and malaria prevalence. The results of structural hierarchal regression modeling mainly supported all the anticipated relationship hypotheses. The study demonstrates a positive and direct relationship between ITNs and malaria prevalence. The findings are consistent with those of previous studies [35,66,67], which showed the benefit of ITNs for malaria protection. The findings imply that ITNs are an actionbased mechanism designed in response to malaria. This finding is consistent with previous findings that ITNs are a malaria prevention method [18].
Furthermore, this finding promotes a contextualized understanding of the possible causes of malaria by providing a set of antecedents rooted in public health, which may inspire cerebral rationalizations. We also found that ITN was positively related to malaria knowledge, and malaria knowledge was positively related to malaria prevalence. The result demonstrated the use of malaria knowledge to increase the effective use of ITNs. These findings highlight the need for knowledge intervention in the implementation of malaria control interventions, such as ITNs. Consistent with the study conducted in four provinces of Zambia that showed high levels of knowledge about malaria with regards to mosquito being the vector and the capacity of malaria to kill in all the provinces, and did not vary statistically [68]. Correlation between increased knowledge and good treatmentseeking behavior was demonstrated. However, the translation of knowledge to improved practice was inadequate. Programs must consider local values and emphasize the role of vectors in the transmission of disease to ensure protection from malaria [69-71]. By relating insecticide-treated mosquito nets to malaria prevalence, this study highlights the implications of malaria knowledge and household income in fighting against malaria for an individual community. Furthermore, the present findings suggest a positive and significant relationship between ITNs and malaria prevalence when the outcome variable is linked with explanatory factors as malaria knowledge plays a mediating role. This argument is consistent with the previous conceptualization that perceived severity, benefit, and self-efficacy, reflecting a reaction to practice [45]. Likewise, this study is consistent with the report that people’s behavior in response to the threat is influenced by their current perception and conceptualization of the diseases [35].
Furthermore, the direct as well as the indirect relationship (via malaria knowledge) between ITNs and malaria prevalence was stronger for the households of the second-level income category. This finding revealed that households owning better income have an improved level of knowledge about malaria. The association may be explained by a person from economically advanced households might have more exposure to information tools such as mass media than the poor. Consistent with the previous finding that reported household income, educational status, and residence as the predictors of malaria knowledge [72]. The present study also found a strong effect of household income in the relationship, suggesting that individuals perform best malaria control interventions when household income is moderate, and that performance is negative and insignificant when household income is too low and too high respectively. Here the relationship may be explained as an individual person from an economically rich family may have an access to search for other alternatives than the existing interventions. On the other hand, the associations for low-income households may be explained by a person who is from a very poor family may be exposed to limitations on the basic necessities such as food, and prefer to sell than households with a better income. This finding is consistent with a previous study, which reported that a lowincome earning community might not have access to effective preventive interventions such as ITNs [73]. Similarly, household income was also reported among the factors that influence awareness regarding malaria and possible malaria prevention access, such as vaccines [74].
Moreover, this study will help to develop an in-depth understanding of the relationship between malaria and household income and the relationship between strategic interventions and the prevalence of malaria in order to achieve malaria elimination. This study has empirically proven its role in evaluating situational factors as moderators and mediators in the relationships when umpiring the ethicality of an action. Generally, our study concludes that there is a positive relationship between ITNs and malaria prevalence, and household income and malaria knowledge play a moderated mediating role. Improvements in the knowledge of malaria transmission and prevention approach revealed as an essential intervention for increasing proper use of ITNs that affects the outcome of malaria. This is therefore a need to strengthen the policy on knowledge of malaria prevention and control as an integral component with the distribution of ITNs in the health care setting to enhance its utilization.
Implications
Malaria imposes a heavy burden on people, particularly in Ethiopia. Local understandings about malaria and the use of malaria control interventions are critical factors in sustained malaria control. Nevertheless, many studies on malaria prevention and control have not studied the effect of malaria knowledge and household income on strategic interventions and malaria relationships. As reported in different studies, access to interventions cannot solve the challenges of its utilization for infectious disease prevention and control, primarily malaria. Therefore, the provision of proper health education programs has to be given due focus to improve awareness about malaria and its prevention. Our findings support the active moderated mediation roles of malaria knowledge and household income in the relationship, where low-level income households are reported to have an insignificant and negative relationship with ITNs. The study reported associations of access to and use of intervention methods with household income [7]. This study offers concrete and practical information for policymakers and health planners on the invaluable advantage of malaria knowledge and household income to ensure the program’s optimum performance. Malaria threatens mostly pregnant women and children, and achieving malaria elimination goals is possible only through awareness creation backed by proper education of vulnerable groups. Therefore, the study recommends that policymakers should strengthen the provision of health education that helps improve program-related knowledge.
Furthermore, the findings demonstrate the incorporation of health-related subjects in education curricula from the primary school level, in line with community-based health literacy for adults. Furthermore, the report suggests that health planners should ensure that the program is understood, particularly in relation to the prevention and control of communicable diseases such as malaria, to strengthen the usage culture of prevention interventions. Also, despite improving access regarding malaria prevention and control methods, policymakers and health planners should recognize that proper education is a significant factor in strengthening the relationship between intervention strategy and malaria. Thus, for infectious disease prevention and control programs to succeed, dimensional observation is crucial. Therefore, the provision of proper health education programs has to give due focus to improve awareness about malaria and its prevention.
Overall, the policy as presently formulated, despite the general understanding of the broad public health implications, the burden of infection and death in sub-Saharan Africa has been largely neglected. This has contributed to the low awareness of malaria control interventions, such as ITNs and IRS, strategic implementations, and the long delay in the elimination of this deadly disease in Africa, and the inability to meet the RBM/ MDGs targets set for 2015. The health implication of these shortcomings is a worsening healthcare sector, a decline in quality of life, unsafe environment, and structural disequilibria. This research offers concrete and practical information to policymakers and health planners, the invaluable advantage of malaria knowledge and income of the household to assure the program’s optimum performance. Malaria threatens mostly pregnant women and children, and achieving malaria elimination goals is only possible through awareness creation backed by proper education for vulnerable groups. So, the study recommends policymakers strengthen the provision of health education programs. Besides, the findings demonstrate the incorporation of health-related subjects in education curricula from the primary school level, in line with community-based health literacy for adults, has to be given due attention to strengthening the usage culture to prevention interventions.
Conclusion
The present study explored how malaria control intervention in terms of mosquito protection positively related to the outcome of malaria through malaria knowledge and household income. Nevertheless, many studies on malaria prevention and control have not studied the effect of these factors on strategic interventions and malaria prevalence. As reported in different studies, access to interventions alone cannot solve the challenges related to utilization. Therefore, the provision of proper health education has to be given due focus to improve awareness about malaria and its prevention. In addition, various studies reported associations between household income and access to and use of intervention methods [7]. Our findings support the active moderated mediation roles of malaria knowledge and household income in the relationship. This study offers concrete and practical information for policymakers and health planners about the priceless advantage of malaria knowledge and household income to ensure the program’s optimum performance. Malaria threatens mostly pregnant women and children, and achieving malaria elimination goals is possible only if program-related understandings for the community are in place. Therefore, this study recommends policymakers strengthen the provision of proper health messages for better sympathetic, such as community-based health literacy for adults. Moreover, it would be significant to discover the cumulative effect of these factors in fighting against malaria on the relationship between explanatory and outcome variables. The findings support the importance of malaria knowledge and household income in the relationship.
Declarations
Disclosure statement for publication: All authors have made substantial contributions to: Conception and design of the study, or acquisition of data, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version submitted. This manuscript has not been submitted for publication in another journal.
Consent for publication: Not applicable
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Competing Interests: The authors declare no conflict of interest.
References
- Greenwood, B. New tools for malaria control – using them wisely. Journal of Infection. 2017; 74: S23–S26.
- DFID Malaria Burden and Interventions Evidence Overview. 2010.
- WHO Global Malaria Programme: WORLD MALARIA REPORT; World Health Organization, Geneva, Switzerland. 2015.
- WHO Global Malaria Programme. World malaria report; World Health Organization, Geneva, Switzerland. 2017.
- World Health Organization (WHO): World malaria report; Geneva. Switzerland. 2016.
- Seyoum D, Speybroeck N, Duchateau L, Brandt P. Long-Lasting Insecticide Net Ownership, Access and Use in Southwest Ethiopia: A Community-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2017; 1312: 1–16.
- Tassew A, Hopkins R, Deressa W. Factors influencing the ownership and utilization of long-lasting insecticidal nets for malaria prevention in Ethiopia. Malaria Journal. 2017; 1–9.
- Tarkang, E. Assessing the ownership, usage, and knowledge of Insecticide Treated Nets (ITNs) in Malaria Prevention in the Hohoe Municipality, Ghana. PanAfrican Medical Journal. 2017; 67: 1–8.
- Watiro, A.H. Insecticide-treated net ownership, and utilization and factors that influence their use in Itang, Gambella region, Ethiopia : cross-sectional study. Risk Management and Healthcare Policy. 2016; 9: 101–112.
- Ernst KC, Erly S, Adusei C, Bell ML, Kessie DK, et al. Reported bed net ownership and use in social contacts is associated with uptake of bed nets for malaria prevention in pregnant women in Ghana. Malaria Journal. 2017; 16: 1–10.
- Manana PN, Kuonza L, Musekiwa A, Mpangane HD, Koekemoer LL. Knowledge, attitudes, and practices on malaria transmission in Mamfene , KwaZulu- Natal Province, South Africa 2015; 18: 1–7.
- Magaço A, Botão C, Nhassengo P, Saide M, Ubisse A, et al. Community knowledge and acceptance of indoor residual spraying for malaria prevention in Mozambique: A qualitative study. Malaria Journal. 2019; 18: 1–12.
- Taremwa IM, Ashaba S, Adrama HO, Ayebazibwe C, Omoding D, et al. Knowledge, attitude and behavior towards the use of insecticide-treated mosquito nets among pregnant women and children in rural Southwestern Uganda. BMC Public Health. 2017; 17: 1–8.
- President’s Malaria Initiative: Malaria Operational Plan; Addis Ababa, Ethiopia. 2016;
- Molla Gedefaw ZA. Knowledge, Attitude and Practice of the Community towards Malaria Prevention and Control Options in Anti-Malaria Association Intervention Zones of Amahara National Regional State, Ethiopia. Journal of Tropical Diseases. 2013; 01.
- Wadunde I, Mpimbaza A, Musoke D, Ssempebwa JC, Ediau M, et al. Factors associated with willingness to take up indoor residual spraying to prevent malaria in Tororo district, Uganda: a crosssectional study. Malaria Journal. 2018; 17.
- Molla Gedefaw ZA. Knowledge, Attitude and Practice of the Community towards Malaria Prevention and Control Options in Anti-Malaria Association Intervention Zones of Amahara National Regional State, Ethiopia. Journal of Tropical Diseases. 2013; 1.
- Fuge TG, Ayanto SY, Gurmamo FL. Assessment of knowledge, attitude and practice about malaria and ITNs utilization among pregnant women in Shashogo District, Southern Ethiopia. Malaria Journal. 2015; 14: 1–9.
- Forero DA, Chaparro PE, Vallejo, AF, Benavides Y, Gutiérrez JB, et al. Knowledge, attitudes and practices of malaria in Colombia. Malaria Journal. 2014; 13: 165.
- Simon Alain Inah, Jimmy Ebi Eko ZU, JAI. Knowledge of Malaria among Adult Residents in Abi Local Government Area, Cross River State, Nigeria. Asian Journal of Research in Medical and Pharmaceutical Sciences. 2017; 1: 1–9.
- Animut A, Negash Y, Kebede N. Distribution and utilization of vector control strategies in a malarious village of Jabi Tehran District, north-western Ethiopia. Malaria Journal. 2014; 13.
- Taffese HS, Hemming-schroeder E, Koepfli C, Tesfaye G, Lee, M, et al. Malaria epidemiology and interventions in Ethiopia from 2001 to 2016. Infectious Diseases of Poverty. 2018; 7.
- Haile S, Abera S, Muhdin S, Kumalo A. Knowledge and Practice towards Prevention and Control of Malaria in Tepi Town, Sheka Zone, Southwestern Ethiopia. Health Sci. J. 2015; 10.
- Birhanu Z, Yihdego YY. ebiyo; Yewhalaw D. Caretakers’ understanding of malaria, use of insecticide-treated net and care seeking-behavior for febrile illness of their children in Ethiopia. BMC Infectious Diseases. 2017; 17: 629.
- Workineh B, Mekonnen FA, Sisay M, Gonete KA. Malaria outbreak investigation and contracting factors in Simada District, Northwest Ethiopia: A case-control study. BMC Research Notes. 2019; 12: 280.
- Constructs T, Concept T. Health Belief Model. 2003.
- Tokponnon FT, Ogouyémi AH, Sissinto Y, Sovi A, Gnanguenon V, et al. Impact of long-lasting, insecticidal nets on anaemia and prevalence of Plasmodium falciparum among children under five years in areas with highly resistant malaria vectors. Malaria Journal 2014; 13: 1–11.
- Rosenstock IM, Strecher VJ, Becker MH. Health Education & Behavior. Society for Public Health Education. 2012; 15: 175–183.
- Health Belief Model.
- Hounton SH, Carabin H, Henderson NJ. Towards an understanding of barriers to condom use in rural Benin using the Health Belief Model: A cross-sectional survey. BioMed Central. 2005; 8: 1–8.
- Cecilia Van Zyl-Schalekamp, A.S. Perceived Threat of Malaria and the Use of Insecticide Treated Bed Nets in Nigeria. African Sociological Review. 2013: 17: 25–44.
- Michielsen K, Chersich M, Michielsen K, Chersich M, Temmerman M Dooms, et al. Van Nothing as Practical as a Good Theory ?. The Theoretical Basis of HIV Prevention Interventions for Young People in… Nothing as Practical as a Good Theory ? The Theoretical Basis of HIV Prevention Interventions for Young People in Sub-Saharan Africa: A. AIDS Research and Treatment. 2016; 2012.
- Robert T. Croyle PD. Theory at a Glance. 2005.
- Alexander Suuk Laar, Amos Kankponang Laar, P.A.D. Community perception of malaria and its influence on health-seeking behaviour in rural Ghana: a descriptive study. MalariaWorld Journal. 2013: 4.
- Vishnu Nandan Koduri, K.G. Awareness about Mosquito Borne Diseases and Practice about Preventive Methods Against Mosquito Bite in Rural Field Practice Area of a Tertiary. Journal of Medical Science And Clinical Research. 2018; 06: 512–518.
- Pinchoff J, Hamapumbu H, Kobayashi T, Simubali L, Stevenson JC, et al. Factors associated with sustained use of long-lasting insecticide-treated nets following a reduction in malaria transmission in southern Zambia. The American Society of Tropical Medicine and Hygiene. 2015; 93: 954–960.
- Bbosa R.S, Ehlers VJ. Pregnant Women’s Utilisation of Anti-Malaria Services in Uganda. SciMed Central. 2017; 4: 1–7.
- Gorgui Diouf Department, Yihua Xu, P.N.K. Evaluation of the Effectiveness of Intervention for Malaria Control in Rural Areas in China. Global Journal of Health Science. 2010; 2.
- Alemu MB, Asnake MA, Lemma MY, Melak MF. Utilization of insecticide-treated bed net and associated factors among households of Kola Diba town, North Gondar, Amhara region, Ethiopia. BMC Research Notes. 2018; 1–5.
- Doda Z, Solomon T, Loha E, Gari T, Lindtjørn BA. qualitative study of use of long-lasting insecticidal nets (LLINs) for intended and unintended purposes in Adami Tullu, East Shewa Zone, Ethiopia. Malaria Journal. 2018; 1–14.
- Nitin Joseph, Maria Nelliyanil, Shashidhar M Kotian, Mohammed Omar, R. Srikanth Aswin, Saiteja Donkena, Smita Jugnu, P.C. Awareness, practices and expenditure towards mosquito bite prevention methods in urban and semi-urban areas of South India. International Journal of Mosquito Research. 2015; 2: 53–59.
- health communication from theory to practice. Second Edition. 2014; ISBN 9781118122198.
- Tobin-West C, Kanu E. Factors influencing the use of malaria prevention methods among women of reproductive age in periurban communities of Port harcourt city, Nigeria. Nigerian Postgraduate Medical Journal. 2016; 23: 6.
- Kristopher J Preacher, D.D.R.& A.F.H. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivariate Behavioral Research. 2007: 42: 185–227.
- Watanabe N, Kaneko A, Yamar S, Leodoro H, Taleo G, Tanihata T, Koji Lum J, Larson, PS. Determinants of the use of insecticideTreated bed nets on islands of pre-and post-malaria elimination: An application of the health belief model in Vanuatu. Malaria Journal. 2014; 13: 441.
- Ahmad YM, K.H. Malaria as a Cause of Morbidity and Mortality in Bangladesh: A Socio-Economic Overview; Research on Humanities and Social Sciences. 2015; 5: 2224–5766.
- Rugnao S, Gonahasa S, Sebuguzi CM, Opigo J, Yeka A, et al. LLIN Evaluation in Uganda Project (LLINEUP): Factors associated with childhood parasitemia and anemia 3 years after a national longlasting insecticidal net distribution campaign: A cross-sectional survey. Malaria Journal. 2019; 1–12.
- Wangroongsarb P, Hwang J, Thwing J, Karuchit S, Kumpetch SRA, et al. Using respondent-driven sampling to identify malaria risks and occupational networks among migrant workers in Ranong, Thailand. PLoS ONE. 2016; 11.
- Health Sector transformation plan (HSTP). Federal Ministry of Health, Addis Ababa, Ethiopia. 2015.
- Balami AD, Said S, Afiah N, Zulkefli M, Norsa B, Audu B. Knowledge, motivation, self ‑ efficacy, and their association with insecticidal net use among pregnant women in a secondary health center in Maiduguri , Nigeria. Malaria Journal. 2018: 17; 359.
- Knight EK. Health Equity Guide for Public Health Practitioners and Partners. 2015.
- Salam RA, Das JK, Lassi ZS, Bhutta ZA. Impact of communitybased interventions for the prevention and control of malaria on intervention coverage and health outcomes for the prevention and control of malaria. Infectious Diseases of Poverty. 2014; 3: 1–15.
- Tayseir TM. Masaad, Yousif M. Elmosaad, Abd Elbasit Elawad Mohammed, Ahmed Elnadif Elmanssury, Mahmoud Jaber, Mustafa M. Mustafa, H.E. Knowledge, Attitude and Practices Among Mothers Towards Insecticide-Treated Nets in Abuharira Village -Um Remta Locality- The White Nile State -2015. Science Journal of Clinical Medicine. 2015; 6: 24–31.
- Odoko JO, Nwose EU, Igumbor EO. Utilization of insecticidetreated nets against malaria among pregnant women in Southern Nigeria. International Journal of Research in Medical Sciences. 2017; 5.
- Dawit Getnet Ayele TTZ, HGM. The risk factor indicators of malaria in Ethiopia. International Journal of Medicine and Medical Sciences. 2013; 5: 335–347.
- Munga S, Kimwetich Z, Atieli F, Vulule J, Kweka EJ. Knowledge and perceptions about indoor residual spray for malaria prevention in mumberes division, Nandi county in central province of Kenya. Tanzania Journal of Health Research. 2017; 19: 1–9.
- Ingabire CM, Alaii J, Hakizimana E, Kateera F, Muhimuzi D Nieuwold I. et al. Community mobilization for malaria elimination: Application of an open space methodology in Ruhuha sector, Rwanda. Malaria Journal. 2014; 13: 1–8.
- Preskill H, Parkhurst M. Juster M. Assess Progress, and Impact. Collective Impact Forum. 2014.
- Bell A. Explaining Fixed Effects: Random Effects Modeling of Time-Series Cross-Sectional and Panel Data*. European political science association. 2015; 3: 133–153.
- Breen R, Karlson KB, Holm A. Total, Direct, and Indirect Effects in Logit and Probit Models. Sociological Methods and Research. 2013; 42: 164–191.
- Schmidheiny, K. Short Guides to Microeconometrics. Panel Data: Fixed and Random Effects; 2018; 2.
- Bollen KA, Odum HW. A General Panel Model With Random And Fixed Effects: A Structural Equations Approach. NIH Public Access. 2011; 1: 1–34.
- Mackinnon DP, Fairchild AJ, Fritz MS. Mediation Analysis. The Annual Review of Psychology. 2007; 58: 593–614.
- Oladimeji KE, Mahlako J, Gwegweni T, Ojewole E, Yunga ST. Knowledge of malaria prevention among pregnant women and non - pregnant mothers of children aged under 5 years in Ibadan, South West Nigeria. Malaria Journal. 2019; 18: 1–12.
- Kumar M, Raghavendra K, Kleinschmidt I, Bhatt RM, Kumar D, Bellamy T, Valecha N. Impact of long-lasting insecticidal nets on prevalence of subclinical malaria among children in the presence of pyrethroid resistance in Anopheles culicifacies in Central India. International Journal of Infectious Diseases. 2017.
- Getachew, D. Ecology and Distribution Pattern of Anopheles Mosquitoes and Malaria Transmission in Ghibe River Basin , southwestern Ethiopia. 2017.
- Sovi A, Azondékon R, Aïkpon RY, Govoétchan R, Tokponnon F, et al. Impact of operational effectiveness of long-lasting insecticidal nets (LLINs) on malaria transmission in pyrethroid-resistant areas. Parasites & Vectors. 2013; 6: 319.
- Shimaponda-Mataa NM, Tembo-Mwase E, Gebreslasie M, Mukaratirwa S. Knowledge, attitudes, and practices in the control and prevention of malaria in four endemic provinces of Zambia. Southern African Journal of Infectious Diseases. 2017; 32: 29–39.
- Ukpai OM, Irole-Eze OP, Amaechi EC, Ejike BU, Ejike EN,et al. A Study of Knowledge, Attitude, and Practices Regarding Malaria Among Inhabitants of Ezinihite Local Government Area, Imo State, Eastern Nigeria. Manila Journal of Science. 2017; 10: 65– 74.
- Ruberto I, Camara S, Banek K, Loua MK. Knowledge, attitudes, and practices of malaria control among communities from the health district of Forécariah in the Republic of Guinea, West Africa. Journal of Vector-Borne Diseases 2014; 51: 119–127.
- Amaechi E, Ukpai O. Knowledge, attitude and practices about malaria among mothers and care-givers in Aba South Local Government Area, Abia State , Nigeria. Animal Research International. 2013; 10: 1786 – 1791.
- Goshu YA, Yitayew AE. Malaria knowledge and its associated factors among pregnant women attending antenatal clinic of Adis Zemen Hospital, North-western. PLOS ONE. 2019; 14: 1–11.
- Attu H, Adjei JK. Local knowledge and practices towards malaria in an irrigated farming community in Ghana. Malaria Journal. 2018; 17: 150.
- Chukwuocha UM, Okorie PC, Iwuoha GN, Ibe SN, Dozie IN, et al. Nwoke, B.E. Awareness, perceptions, and intent to comply with the prospective malaria vaccine in parts of South Eastern Nigeria. Malaria Journal. 2018; 1–7.