
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Two case series of Chiladiti syndrome and a review of literature
Citra Aryanti*; I Ketut Wiargitha; I Nengah Kuning Atmadjaya
Department of General Surgery, Udayana University, Sanglah General Hospital, Indonesia.
*Corresponding Author: Citra Aryanti
Department of Obstetrics and Gynecology, University
of Sumatera Utara, Medan, Indonesia.
Email: citra.aryanti@hotmail.com
Received : Oct 07, 2021
Accepted : Nov 24, 2021
Published : Nov 30, 2021
Archived : www.jcimcr.org
Copyright : © Aryanti C (2021).
Abstract
Introduction: Chilaiditi’s syndrome was repeatedly an unforgettable case in Emergency Department due to its various symptoms.
Methods: This case report consisted two reported cases of Chilaiditi syndrome. Then, we followed the methods of PRISMA for systematic review.
Results: In this report, two cases of Chilaiditi syndrome with the different chief of complaint when admitted to the hospital. A 35-yearold woman presented to the Emergency ward with abdominal pain, while the older subject, a 67-year-old man complained of shortness of breath. Plain radiograph showed an elevated right hemidiaphragm and the presence of subphrenic air, making the diagnosis of Chilaiditi syndrome. Both patients were managed conservatively with nasogastric tube decompression and intravenous fluid. The follow up showed favorable results and symptoms resolved.
Discussion: Chilaiditi syndrome might not be a rare entity, but a difficult syndrome to identify clinically due to its various unspecific symptoms. The radiological examination was needed to be carried out for the diagnosis. Conservative management led to favorable results.
Conclusion: Clinicians should be more aware of the diagnosis of Chilaidity syndrome with its various symptoms. Radiological evidence should be obtained for the confirmed diagnosis, and conservative management was the modality choice.
Keywords: Chilaiditi syndrome; radiology; conservative.
Citation: Aryanti C, Wiargitha IK, Atmadjaya INK. Two case series of Chiladiti syndrome and a review of literature. J Clin Images Med Case Rep. 2021; 2(6): 1443.
Introduction
Chilaiditi was first described by a radiologist, named Demetrius Chilaiditi in 1910, after his publication of 3 cases of hepatodiphragmatic interposition of colon [1]. Chilaiditi’s syndrome refers to either temporary or permanent interposition of the small intestine or colon to the hepatodiaphragmatic space, causing symptoms. Male dominated the cases with a 4:1 ratio than that of female [2]
Chilaiditi syndrome was mostly asymptomatic or present with mild signs such as unspecified abdominal pain, nausea, vomiting, and constipation. In advanced cases, it might be presented with shortness of breath if the lung was lifted [3]. These symptoms could be misled the surgeon to carry out unnecessary surgery for seriously mistaken abnormalities [4]. However, on the other side, this syndrome could precipitate or found coincidence with other serious abnormalities. Regardless of that, in the Emergency Department, the diagnosis of the chilaiditi syndrome was mostly forgotten to be a differential diagnosis of such various symptoms. In this case report, we presented two cases of the chilaiditi syndrome, who presented with different symptoms.
Methods
This case report is described based on two cases encountered in center in the past 1 year. Literature searching for systematic reviews followed the methods of PRISMA. Systematic reviews cover all Chiladiti cases reported throughout the world. The parameters assessed were symptoms, clinical findings, radiological findings, management, and results of treatment. In addition, the results of the systematic review were also compared to the cases we reported in the discussion section.
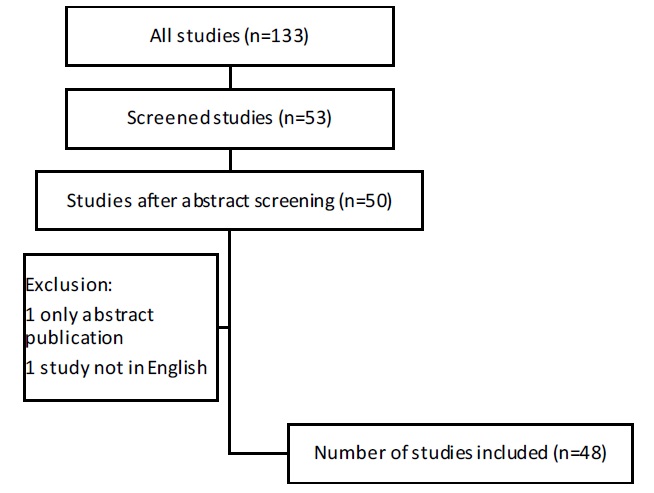
In a systematic literature search of the Publisher and Cochrane Central Register of Controlled Trials databases using the search terms (“chilaiditi” [MeSH Terms] OR “chilaiditi” [All Fields]) AND (“Syndrome” [MeSH Terms] OR “syndrome” [All Fields]), we identified 133 citations defined for the purpose of this review. From the 133 articles, 47 articles consisting of 60 cases were included which were matched with the parameters from this study. The data was managed by PRISMA guidelines and other Note programs. Figure 1 shows a flow diagram of the literature search algorithm.
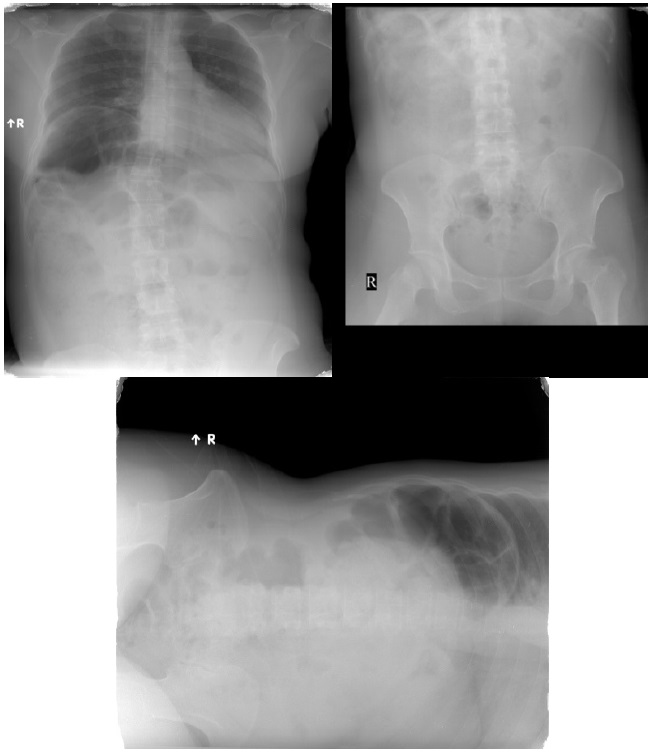
X-Ray (Figure 2). The right hemidiaphragm was also shown to be elevated. Abdominal ultrasound confirmed the prominent haustra at the right hemidiaphragm, a Chilaiditi sign. The patient was managed conservatively with intravenous fluid and conservatively. She was discharged after 2 days of inpatient care with the favorable condition. However, the patient refused any radiograph to be done for final confirmation due to relieving symptoms.
Results
Case 1
A 35-year-old woman was presented with intermittent epigastric pain for 3 days before admitted to the Emergency Department. The epigastric pain was worse, with the presence of nausea and vomiting since 2 days ago. She also complained about the difficulty of passing stool. She stated that she did not have flatus for 1 day. Any history of surgery and previous illness were denied. Physical examination showed epigastric tenderness without any sign of peritoneal irritation. The patient was firstly evaluated by the primary health care without any imaging modalities, then she was referred to our hospital with the suspicious diagnosis of acute abdomen. Laboratory findings were within normal limits. Then, she underwent abdominal XRay, in the supine, erect, and left lateral decubitus position. The plain radiographs findings revealed the presence of air at the subphrenic which did not change in the left lateral decubitus
Case 2
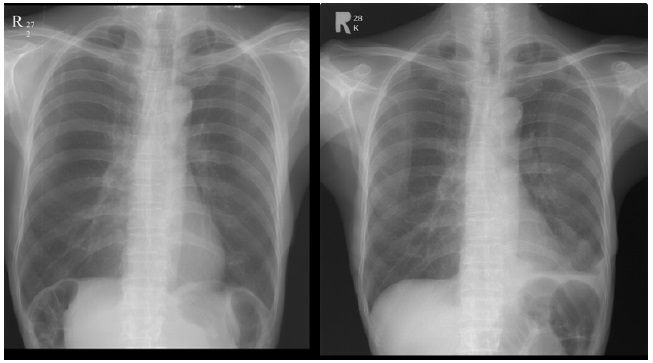
A 62-year-old man presented with shortness of breath for 1 week before hospital admission. The patient has a history of mass at the buccal which has not been confirmed by open biopsy. He also complained of unspecified abdominal pain, but did not come too often. He had nausea but denied any history of vomiting. He had additional symptoms, epistaxis, which was suspect from the tumoral bleeding. Physical examination showed only slight decreased breath sound at the bottom of the right lung. Unremarkable findings were shown for the abdominal region. Chest radiograph was obtained and confirmed the elevated right hemidiaphragm, a Chilaiditi sign, with the presence of minimal right lung pleural effusion due to pulmonary metastases (Figure 2). He was then managed conservatively with oxygenation, decompression and intravenous fluid. In this patient, he also received tranexamic acid to control the tumoral bleeding. After several days of care, the symptoms were resolved and the patient was discharged. Another follow up and workup diagnostic for the buccal mass was done after the symptoms resolved.
Discussion
Chilaiditi syndrome was found in 0.25-0.28% of the population [3]. Actually, the chilaiditi syndrome was first described by Cantini in 1865, it was public after observation in the clinical examination in 1910 by Chilaiditi. Chilaiditi syndrome is a great mimicker with symptoms that imitate various medical and surgical emergencies [5]. Several theories have been proposed for chilaiditi syndrome, including the cause of anatomic distortions such as the laxity, absence, or elongation of the suspensory ligaments or the falciform ligament [6]. Some authors suggested that there is weak zone of the liver surface that created low resistance of minimal pressure, even pressure from fibrous bands between diaphragmatic muscle fibers [7]. Other causes were liver atrophy, elevated diaphragm due to phrenic nerve injury, development of sub diphragmatic spaces after liver surgery, or obesity/weight loss that cause distortion of abdominal fat [3].
These diaphragmatic slips are often found on the right hemidiaphragm, with their concavity parallel to the falciform ligament [8]. The presence of diaphragmatic slips and associated hepatic grooves, in this case, created the ‘indented' appearance of free air on the plain radiographs. A lung that is compressed by the distended loops of the bowel underneath his diaphragms will the cause of his respiratory distress, similar to dyspnoea associated with ascites [3].
From table 1, we presented our literature search in the last 10 years for the study that reported Chilaiditi syndrome cases. All cases were found as an incidental finding from the Chest XRay and confirmed by abdominal CT Scan. Nearly all continents had reported at least one case of Chiladiti syndrome, with a total of cases. Majority of the reported cases showed that the most common symptoms were epigastric pain with or without radiation to the right shoulder and constipation. Some cases were presented with shortness of breath. Not surprisingly, other authors reported that Chilaiditi syndrome could be mistakenly diagnosed as acute abdomen (peritonitis, ileus), lung disease, even myocardial infarction. Physical findings were not specific although most cases reported abdominal tenderness. All case reports reported 100% favorable outcome with conservative treatment. The symptoms resolved in the range of 6 hours to 2 months. Among cases that required surgery were those which coincidentally occurred with other abnormalities.
Table 1:Worldwide reported cases of Chilaiditi syndrome in the last 10 years (2009-2019) [5,10-54].
Case report |
Country |
Number of cases |
Symptoms |
Physical findings |
Radiological findings |
Management |
Outcome |
Malavade (2010) |
India |
1 |
Abdominal pain, dyspepsia, chest pain with angina-like symptoms |
Sign of acute intestinal obstruction |
X-Ray: elevated right hemidiaphragm |
Conservative |
Favorable |
Okiro (2010) |
Ireland |
1 |
Abdominal pain, chronic constipation, respiratory distress |
Unremarkable |
X-Ray: elevated right hemidiaphragm |
Conservative with laxative and enema |
Favorable |
Blevins (2011) |
USA |
1 |
Abdominal pain, vomiting |
Unremarkable |
Laparoscopy diagnostic |
Conservative with laxative and dietary changes |
Favorable |
Nagem (2011) |
Brazil |
1 |
Epigastric pain, right shoulder pain |
Tense and painful abdomen |
X-Ray: air in subphrenic |
Conservative with intravenous fluid |
Favorable |
Lin (2012) |
Taiwan |
6 |
Unspecified abdominal pain, constipation |
Tenderness in the abdomen |
X-Ray: air in subphrenic |
5 were managed conservatively with decompression and laxatives |
Favorable |
Yin (2012) |
USA |
1 |
Abdominal pain |
Sign of intestinal obstruction |
CT Scan |
Laparoscopic management due to failed conservative treatment |
Favorable |
Choi (2013) |
Australia |
1 |
Abdominal discomfort, nausea, vomiting |
Unremarkable |
Gastroscopy |
Laparotomy due to coincidence with strangulated ileum |
Favorable |
Liu (2013) |
Taiwan |
1 |
RUQ pain |
Abdominal distention, RUQ tenderness |
X-Ray: elevated right hemidiaphragm |
Conservative with oxygenation, chest care, and pain control |
Favorable |
Chen (2014) |
Taiwan |
1 |
Chest pain |
Unremarkable |
X-Ray: increased intestinal gas |
Conservative for analgesic and intravenous fluid |
Favorable |
Ho (2014) |
Taiwan |
1 |
Epigastric pain |
Epigastric distention |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Mesquita (2014) |
Israel |
1 |
Abdominal pain, shortness of breath |
Extreme abdominal distention, bloating and respiratory distress. |
X-Ray: air in subphrenic |
Conservation with decompression |
Favorable |
Weng (2014) |
China |
7 |
Abdominal tenderness, constipation |
Abdominal pain |
X-Ray: air in subphrenic |
4 were managed conservatively with intravenous fluid and enema |
Favorable |
Zhou (2014) |
China |
1 |
RUQ pain |
Tenderness at RUQ, decreased bowel sound |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Erdem (2015) |
Turkey |
2 |
Abdominal pain, shortness of breath, coughing |
Unremarkable |
X-Ray: elevated right hemidiaphragm |
Conservative with laxative and high fiber diet. Respiratory tract infection was managed with antibiotics, oxygen, and analgesic |
Favorable |
Nayak (2015) |
India |
1 |
Pain at upper abdomen, constipation |
Diffuse tendered abdomen |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Quiroga (2015) |
Spain |
1 |
Epigastric pain, constipation |
Peritoneal irritation |
X-Ray: elevated right hemidiaphragm |
Laparotomy (no other findings), finally diagnosed with Ogilvie syndrome |
Favorable |
Uygungul (2015) |
Turkey |
1 |
Epigastric pain |
Epigastric tenderness |
X-Ray: air in subphrenic |
Conservative with pain management and intravenous fluid |
Favorable |
Watanabe (2015) |
Japan |
1 |
Upper abdominal pain, dyspnea |
Peritoneal irritation |
X-Ray: increased intestinal gas |
Laparotomy with coincidence finding of Bochdalek hernia |
Favorable |
Chen (2016) |
USA |
1 |
Epigastric pain, RUQ pain, nausea, vomiting |
Tenderness in the epigastrium and RUQ |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Everngul (2016) |
Turkey |
1 |
Upper abdominal pain, constipation |
Abdominal pain |
X-Ray: air in subphrenic |
Conservative with pain management and intravenous fluid |
Favorable |
Garg (2016) |
India |
1 |
Abdominal pain, respiratory symptoms |
Unremarkable |
X-Ray: air in the subphrenic |
Conservative |
Favorable |
Gurvits (2016) |
USA |
1 |
Bloating, constipation |
Abdominal distention |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Ittayachen (2016) |
India |
1 |
Cough and fever |
Decreased breath sound in the right infrascapular area |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Jangouk (2014) |
USA |
1 |
Abdominal pain, constipation, bloating |
Unremarkable |
CT Scan |
Conservative with intravenous fluid |
Favorable |
Takahashi (2016) |
Japan |
1 |
Right upper abdominal pain, vomiting |
Right upper abdominal tenderness |
X-Ray: air in subphrenic |
Laparotomy due to the development of ileus |
Favorable |
Zvezdin (2016) |
Russia |
1 |
Abdominal pain, respiratory distress |
Unremarkable |
X-Ray: elevated right hemidiaphragm |
Conservative with decompression |
Favorable |
Aquilar-Garcia (2017) |
Spain |
1 |
RUQ abdominal pain, nausea, vomiting, bloating, constipation |
Unremarkable |
X-Ray: elevated right hemidiaphragm |
Conservative with laxative and enema |
Favorable |
Cawich (2017) |
Trinidad & Tobago |
1 |
Upper abdomen pain |
Tenderness at RUQ |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Garcia (2017) |
USA |
1 |
Abdominal pain, diarrhea |
Abdominal distention |
CT Scan |
Robotic surgery laparotomy due to persistent abdominal pain |
Favorable |
Hountis (2017) |
Greece |
1 |
Abdominal pain, radiation to the shoulder |
Abdominal tenderness |
CT Scan |
Conservative |
Favorable |
Krzeminski (2017) |
Poland |
1 |
Epigastric pain radiating to the right side of the abdomen |
Abdominal pain |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Laharwani (2017) |
USA |
1 |
N/A |
Abdominal distention |
X-Ray: air in subphrenic |
Conservation with decompression |
Favorable |
Naji-amrani (2017) |
Morocco |
1 |
Abdominal pain, cough with mucopurulent sputum |
Bilateral bronchial rales |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Okiro (2017) |
Japan |
1 |
Abdominal and chest pain |
Unremarkable |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Shinha (2017) |
USA |
1 |
Abdominal pain, nausea, vomiting |
Diffuse tender abdomen, decrease bowel sound |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Taha (2017) |
Oman |
1 |
Epigastric and RUQ pain with radiation to right shoulder |
No abnormalities |
X-Ray: air in subphrenic |
Conservative with pain management and intravenous fluid |
Favorable |
Ali (2018) |
UAE |
1 |
Dyspnea, severe retrosternal chest pain |
Pericardial rub, abdominal tenderness |
X-Ray: elevated right hemidiaphragm |
Conservative |
Favorable |
Gad (2018) |
Egypt |
1 |
Abdominal pain, cough |
Abdominal distention |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Harpain (2018) |
Austria |
1 |
Epigastric pain, nausea |
Unremarkable |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Hussain (2018) |
UAE |
1 |
Abdominal pain, cough |
Abdominal distention, inspiratory, ronchi |
X-Ray: elevated right hemidiaphragm |
Conservative |
Favorable |
Kapania (2018) |
USA |
1 |
RUQ pain, severe cough |
RUQ distention |
CT Scan |
Laparoscopic exploration due to long pain duration and frequency |
Favorable |
Karaman (2018) |
Turkey |
1 |
Epigastric pain, hiccups, constipation |
Tenderness at the epigastric area and RUQ |
X-Ray: air in subphrenic |
Conservative with high fiber diet and laxatives |
Favorable |
Krishna (2018) |
India |
1 |
Respiratory distress, hemoptysis |
Sign of liver cirrhosis |
X-Ray: elevated right hemidiaphragm |
Conservative for chilaiditi and noninvasive ventilation, steroid, antibiotics for pneumonitis |
Favorable |
Luo (2018) |
China |
1 |
Abdominal pain constipation |
Abdominal distention |
X-Ray: air in subphrenic |
Conservative with decompression |
Favorable |
Ogasawara (2018) |
Japan |
1 |
Abdominal pain, constipation, respiratory distress |
Abdominal pain |
X-Ray: air in subphrenic |
Conservative with a laxative (relieve the respiratory distress) |
Favorable |
Sunkara (2018) |
USA |
1 |
Abdominal pain |
Abdominal pain |
X-Ray: air in subphrenic |
Laparotomy due to the presence of cecal perforation |
Favorable |
Vasileiadis (2018) |
Greece |
1 |
Epigastric and RUQ pain with radiation to right shoulder |
Unremarkable |
X-Ray: elevated right hemidiaphragm |
Conservative |
Favorable |
Virmani (2018) |
India |
1 |
Abdominal pain (unspecified), shortness of breath |
Tenderness of abdomen |
X-Ray: air in subphrenic |
Conservative with intravenous fluid and bronchodilators. Occur concomitantly with congenital diaphragmatic hernia |
Favorable |
The diagnosis of chilaiditi was only made with radiological evidence while in the absence of symptoms, the radiological finding just called chialiditi sign [55]. Criteria for Chilaiditi diagnosis were the elevation of right diaphragm above the liver by the intestine, the air in the subphrenic space, and depression of the superior margin of the liver below the left diaphragm [56]. The free air below diaphragm could lead to a conclusion of pneumoperitoneum if it were not confirmed by left lateral decubitus X-Ray which in Chilaiditi, the lucency did not shift upon the changing position [57]. Other imaging methods indicated for the differential diagnosis of Chilaiditi's syndrome include chest/abdominal computed tomography or MRI [58]. The trends from the analysis of the case was that, in pediatric patients, the workup diagnostics were made more carefully. Choi (2013) and Blevins (2011) even carried out laparoscopy and gastroscopy, respectively, to make sure that there were no other abnormalities that precipitate the abdominal pain [10,14].
Chilaiditi syndrome is managed conservatively with intravenous fluid, laxatives or enema, and nasogastric decompression. If it was complicated with inestinal obstruction, perforation, or strangulation, surgical intervention became mandatory. Patients with persistent recurring symptoms or failed to be managed conservatively were also managed surgically [59]. For the surgical approach, cecopexy was showed to be effective, unless gangrene or perforation necessitates bowel resection [60]. Although Saber et al. previously reported that 26% of patients require surgical management, the analysis of reported cases showed a lower number [4].
An interesting case reported by Quiroga et al. (2015) in Spain, which laparotomy was done for Chilaiditi syndrome in suspicious coincidence with peritonitis. The laparotomy showed no other abnormalities. Finally, the physicians revealed the use of psychotropic medications, which were then stopped, and the patient recovered uneventfully. The clinicians made a diagnosis of Oglieve syndrome, that happened in line with Chilaiditi syndrome [23].
Chilaiditi could be mistakenly diagnosed or found additionally with a variety of pulmonary and gastrointestinal disease. In this case, the author showed that Chilaiditi could be either presented with abdominal or respiratory symptoms. When evaluating asymptomatic patient, other abnormalities should be ruled out carefully [30]. The author recommended doing a CT Scan should be done to make sure the diagnosis of Chilaiditi syndrome. In the patient with persistent symptoms of the chilaiditi syndrome, attention needs to be given because this syndrome can be a precipitate factor for the additional condition of intestinal strangulation or obstruction. Therefore, a tight observation was needed to early diagnosis any sign of intestinal obstruction which resulted from the presence of Chilaiditi syndrome.
Conclusion
Clinicians should be more aware of the diagnosis of Chilaiditi syndrome with its various symptoms. Radiological evidence should be obtained for the confirmed diagnosis and conservative management was the modality choice.
References
- Chilaiditi D. [Zur frage der hepatoptose und ptose im allgemeinen im Anschluss an drei Falle von temporarer, partieller Leberverlagerung] [Article in German]. Fortcshr Geb Rontgenstr Nuklearmed Erganzongsband 1910; 16: 173-208.
- Okus A, Ay S, Çarpraz M. Chilaiditi syndrome. Eur J Gen Med 2013; 10: 79-82.
- Alva S, Shetty N, Longo W. Chilaiditi sign or syndrome. Arch Surg 2008; 143: 93-4.
- Saber A, Boros M. Chilaiditi’s syndrome: What Should Every Surgeon Know? Am J Surg 2005; 71: 261-3.
- Okiro JO. Chilaiditi syndrome mimicking congestive heart failure. BMJ Case Rep 2017; 2017: bcr-2017-220811.
- Macchi, V, Feltrin, G, Parenti, A. Diaphragmatic sulci and portal fissures. J Anat 2003; 202: 303–308.
- Joshi, SD, Joshi, SS, Athavale, SA. Some interesting observations on the surface features of the liver and their clinical implications. Singap Med J. 2009; 50: 715–719.
- Gardner, MT, Cawich, SO, Shetty, R. Hepatic surface grooves in an Afro-Caribbean population: a cadaver study. Ital J Anat Embryol. 2015; 120(2): 117–126.
- Malavade V, Udyavar A. Chilaiditi syndrome with associated angina. J Assoc Physicians India. 2010; 58: 44-5.
- Blevins WA, Cafasso DE, Fernandez M, Edwards MJ. Minimally invasive colopexy for pediatric Chilaiditi syndrome. J Pediatr Surg. 2011; 46(3): e33-5.
- Nagem RG, Freitas HL. Chilaiditi’s syndrome: a case report. Radiol Bras. 2011; 44(5): 1-3.
- Lin CH, Yu JC, Ou JJ, Lee YT, Huang M, Wu HS. Chilaiditi syndrome: The pitfalls of diagnosis. Surg Science. 2012; 3: 141-4.
- Yin AX, Park GH, Gamett GM, Balfour JF. Chilaiditi syndrome precipitated by colonoscopy: A case report and review of the literature. Hawaii J Med Public Health. 2012; 71: 158-62.
- Choi SD, Choi KS, Choi YS. Unusual case of a closed-loop small bowel obstruction caused by Chilaiditi syndrome. ANZ J Surg. 2013; 83(9): 694-5.
- Liu WC, Hsiang CW, Liu CH, Huang GS. Chilaiditi’s syndrome with interposed sigmoid colon mimicking traumatic pneumoperitoneum. Can J Gastroenterol. 2013; 27(7): 389-93.
- Chen YY, Chang H, Lee SC, Huang TW. Chilaiditi syndrome presenting as chest pain in an adult patient: a case report. J Med Case Rep. 2014; 8: 97-9.
- Ho MP, Cheung WK, Tsai KC, Chou AH. Chilaiditi Syndrome Mimicking Subdiaphragmatic Free Air in an Elderly Adult. J Am Geriatrics Society. 2014; 62(10): 1-3.
- Mesquita MB, Lubertzky R, Cohen S. Chilaiditi Syndrome as A Cause of Respiratory Distress: A Case Report and Review of the Literature. J Gastrointestinal & Diges Sys. 2014; 44: 188-90.
- Weng WH, Lie D, Feng CC, Que RS. Colonic interposition between the liver and left diaphragm - management of Chilaiditi syndrome: A case report and literature review. Oncol Lett. 2014; 7: 1657-60.
- Zhou H, Hu Z. Man with air below the right diaphragm. Annals of Emergency Med. 2014; 63(1): 13-7.
- Erdem SB, Nacaroglu HT, Karkiner CS, Alper H, Can D. Chilaiditi Syndrome in Two Cases Presented with Respiratory Distress Symptoms. Turk Thorac J. 2015; 16(2): 97–100.
- Nayak TK, Sahoo TK , Mishra BB. Chilaiditi Syndrome: A Case Report And Review of Literature. Int J Dent Med Res. 2015; 1(5): 119-120.
- Quiroga LB, Togores PT, Casajus JM, Villadoniga A, Pena MI, Munoz AS. Ogilvie Syndrome and Chilaiditi Syndrome: a Strange Association. Indian J Surg. 2015 ; 77(Suppl 2): 742–743.
- Uygungul E, Uygungul D, Ayrik , Narci H, Bozkurt S, Kose A. Chilaiditi sign: why are clinical findings more important in ED? The Am J Emerg Med. 2015; 33(5): 731-3.
- Watanabe M, Ishibashi O, Watanabe M, Kondo T, Ohkohchi N. Complicated adult right-sided Bochdalek hernia with Chilaiditi’s syndrome: a case report. Surg Case Rep. 2015; 1: 95-9.
- Chen SY, Chen NF, Lu CS. Chilaiditi syndrome. QJM. 2016; 1: 1-3.
- Evrengul H, Yuksel S, Orpak S, Ozhan B, Agladioglui K. Chilaiditi syndrome. J Pediatr. 2016; 173: 260-3.
- Garg K, Mohapatra PR, Aggarwal D, Gupta R, Jamnmeja AK. Interstitial Lung Disease with Chilaiditi Syndrome. J Clin Diagn Res. 2016; 10(2): 4-15.
- Gurvits GE, Lau N. Air under the right diaphragm: Colonoscopy in the diagnosis of Chilaiditi syndrome. Gastrointest Endosc. 2016; 69: 758-759.
- Ittyachen AM, Eapen M, Kumar R. Chilaiditi’s sign. Eur J Int Med. 2016; 28: 5-6.
- Jangouk P, Zaidi F, Hashash JG. Chilaiditi’s Sign: A Rare Cause of Abdominal Pain. ACG Case Rep J. 2014; 1(2): 70-1.
- Takahashi K, Ito H, Katsube T, Tsuboi A, Hashimoto M, Ota E, et al. Treatment of Chilaiditi syndrome using laparoscopic surgery. Asian J Endoscopic Surg. 2016; 1: 1-3.
- Zvezdin B, Savic N, Hromis S, Kolarov V, Tausan D, Krjajic B. Chilaiditi’s sign and syndrome: theoretical facts and a case report. Vojnosanit Pregl. 2016; 73(3): 277–279.
- Aguilar-Garcia CR, Garcia-Acosta J. Chilaiditi’s sign and syndrome. Case report. Rev Med Inst Mex Seguro Soc. 2017; 55(1): 114-7.
- Cawich SO, Spence R, Mohammed F, Gardner M, Sinanan A, Naraynsingh V. The liver and Chilaiditi’s syndrome: Significance of hepatic surface grooves. SAGE Open Med Case Rep. 2017; 5:-9.
- Garcia O, Rayhrer C. Surgical management of Chilaiditi syndrome with da Vinci® robotic system. Int J Surg Case Rep. 2017; 41: 450–452.
- Hountis P, Chounti M. Chilaiditi’s sign or syndrome? Diagnostic question in two patients with concurrent cardiovascular diseases.Monaldi Arch Chest Dis. 2017; 87(2): 775-9.
- Krzeminski S. Chilaiditi syndrome - A case report. Pol Merkur Lekarski. 2017; 42: 170-172.
- Laharwani H, Nookala V, Cheriyath P. Chilaiditi Syndrome - Air Under Diaphragm Not Always a Surgical Emergency. Journal of Emergency and Internal Medicine. 2017; 1:1-5.
- Naji-amrani H, Ouarssani A. Chilaiditi syndrome. Pan Afr Med J. 2017; 26: 129.Okiro. 2017.
- Shinha T. Chilaiditi syndrome. Intern Med. 2017; 56: 1125–1126.
- Taha TA. Chilaiditi`s syndrome: correct diagnosis can save the patient from unnecessary and life threatening surgery. J Advanced Surg Res. 2018; 2: 1-5.
- Ali MI, Essawy BE, Menakuru S. Undiagnosed Chilaiditi syndrome presenting with pericarditis in a patient with congenital anomalies.
- Gad MM, Al-Husseini MJ, Salahia S, Saad AM, Amin R. Chilaiditi syndrome – a rare case of pneumoperitoneum in the emergency department: A case report. J Med Case Rep. 2018; 12: 263-5.
- Harpain F, Gasche C, Prager G, Silberhumer GR. A siphon-like retrogastric transverse colon: A case report. Int J Surg Case Rep. 2018; 44: 110-3.
- Hussain S. Chilaiditi Syndrome-What’s Air Doing There?. J Emerg Med. 2018; 55: e131-e132.
- Kapania EM, Link C, Eberhardt JM. Chilaiditi Syndrome: A Case Report Highlighting the Intermittent Nature of the Disease. Case Rep in Med. 2018; 1: 1-3.
- Karaman O, Kahyaoglu M, Alpay E, Kalayci A, Gecmen C. Chilaiditi syndrome. Korean J Intern Med 2018; 33: 1255-30.
- Krishna P, Panda PK, Hariprasad S, Singh SS, Gedela SR. A case of liver cirrhosis and Chilaiditi syndrome with atypical pneumonitis. JFMPC 2018; 7: 471-4.
- Luo XG, Wang J, Wang WL, Yu CZ. Intermittent abdominal pain accompanied by defecation difficulties caused by Chilaiditi syndrome: A case report. World J Clin Cases. 2018; 6: 1042-6.
- Ogasawara M, Ishiyama A, Sugiura A, Segawa K, Nonaka I, Takeshita E, et al..Duchenne muscular dystrophy with platypnea-orthodeoxia from Chilaiditi syndrome. Brain Dev. 2018; 40: 339-342.
- Sunkara T, Rawla P, Yarlagadda KS, Baltazar GA, Gaduputi V. Chilaiditi Syndrome Complicated by Cecal Perforation in the Setting of Scleroderma. J Investig Med High Impact Case Rep. 2018; 6: 1-3.
- Vasileiadis P, Mavridis G, Keramidas A, Chardalidou D, Pervos I, Charalampous C. Psychiatric patient with Chilaiditi’s syndrome. Clin Schizophr Relat Psychoses. 2018; 26: 1-5.
- Virmani S, Saluja S. Chilaiditi syndrome: An unusual post-operative complication of congenital diaphragmatic hernia. Indian J Case Reports. 2018; 4: 1-2.
- Fisher AA, Davis M W. An elderly man with chest pain, shortness of breath, and constipation. Postgrad Med J. 2003; 180;79: 183–184.
- Yagnik VD. Chilaiditi syndrome with carcinoma rectum: rare entity. Saudi J Gastroenterol. 2011; 17: 85–86.
- Moaven O, Hodin A. Chilaiditi syndrome: A rare entity with important differential diagnoses. Gastroentero & Hepat. 2012; 8: 276–8.
- Farkas R, Moalem J, Hammond J. Chilaiditi’s sign in a blunt trauma patient: a case report and review of the literature. J Trauma. 2008; 65: 1540–2.
- Caglayan K, Dogan H, Sögüt O, Ozgönül A. Chilaiditi Syndrome: A Report of Two Cases. Internet J Emerg Med. 2008; 6: 105-8.
- Flores N, Ingar C, Sánchez J, et al. The Chilaiditi syndrome and associated volvulus of the transverse colon, Rev Gastroenterol Peru. 2005; 25: 279-8.