
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Radiologic diagnosis of an atypical multilocular Stafne bone lesion
T Lang1*; A Gahleitner2; A Moritz3; C Ulm1
1 Clinical Division of Oral Surgery, University Clinic of Dentistry, Medical University of Vienna, Vienna, Austria.
2 Clinical Division of Radiology, University Clinic of Dentistry, Medical University of Vienna, Vienna, Austria.
3 Clinical Division Unit, University Clinic of Dentistry, Medical University of Vienna, Vienna, Austria.
*Corresponding Author: Tobias Lang
Clinical Division of Oral Surgery, University Clinic of
Dentistry, Medical University of Vienna, Sensengasse
2a, 1090 Vienna, Austria.
Email: tobias.lang@meduniwien.ac.at
Received : Oct 07, 2021
Accepted : Nov 24, 2021
Published : Nov 30, 2021
Archived : www.jcimcr.org
Copyright : © Lang T (2021).
Abstract
Background: The typical patient diagnosed with a Stafne cyst is male and 40 to 60 years old. The ovoid cavities are usually located lingual in the molar region of the lower jaw underneath the inferior alveolar nerve and appear unilateral. The bone lesion is most probably caused by the pressure of the submandibular gland against the lower jaw bone.
Case presentation: A 48-year old patient was referred to the department of oral surgery of the dental university clinic in Vienna by a local dentist, following a diagnosis of two apparent cavities identified by a panoramic x-ray. The findings in the panoramic x-ray and CT scan were inconclusive.
The surface of the two lingual open, ovoid cavities in the left mandibula exposed plain cortical bone. In the MRI-scan, adipose, lymphatic and gland tissues were found which are characteristic features of Stafne cyst bone cavities.
Conclusion: Diagnosing a Stafne cyst on a panoramic x-ray is almost impossible. Further radiologic investigation is essential in order to exclude differential diagnoses. A CT scan can verify the typical lingual opening of the cavity. The diagnosis of a Stafne cyst can only be made by assessing the soft tissue contained in the cavity, therefore a MRI scan is highly recommended.
Keywords: bone lesion; stafne; MRI; radiology; oral surgery; dentistry.
Citation: Lang T, Gahleitner A, Moritz A, Ulm C. Radiologic diagnosis of an atypical multilocular Stafne bone lesion. J Clin Images Med Case Rep. 2021; 2(6): 1444.
Introduction
Edward C. Stafne first described 35 cases of unilateral, asymptomatic, ovoid radiolucencies in 1942 [1]. In panoramic radiographs, these lesions are typically located in the posterior region of the mandible, distal to the third molar and caudal of the inferior alveolar nerve, limited by the mandibular border and the mandibular angle. The borders of the lesion shown in a panoramic radiograph can be either sharply defined or indistinct. Due to the missing epithelial lining a Stafne cyst is also called a “pseudocyst”. Due to the prevalence of 0,5%, the Stafne bone cavity (SBC) is a rare lesion of the mandible [2]. The highest prevalence is reported in 40 to 60 year old males years [3]. The etiology of SBC is still under debatebut studies suggest that persistinglocalized mechanical pressure exerted by the submandibular or sublingual glands is responsible for the bone defect [2,4,5]. Due to the wide range of possible differential diagnoses– from benign to malign lesions - further radiologic investigation such as computer tomography (CT) or even a surgical biopsy is necessary in order to set a definite diagnosis [2,6]. Histologic analysis showed that SBC lesions contain adipose, lymphatic and gland tissues [7]. In order to evaluate the soft tissue without surgical intervention or other invasive treatment modalities including endodontic therapy, bone trephination and bone exploration surgery, a magnetic resonance imaging (MRI) scan has been suggested in the diagnostic algorithm for SBC [2,8]. The case report below details a rare case of multilocular SBC and its diagnostic challenges at the dental university clinic in Vienna.
Case presentation
A 48-year-old male patient was referred to the department of oral surgery of the dental university clinic in Vienna for further evaluation of two ovoid radiolucencies found in the left mandible by his local dentist on a panoramic radiograph. The patient showed no relevant medical history and had no complaints in the area of the questionable osteolysis. Alcohol and tobacco were only consumed occasionally.
Neither intraoral nor extraoral clinical examination showed any mentionable findings. First and second left lower molars reacted positively to pulp sensitivity testing with CO2 -snow. In the region of the mental nerve no paresthesia or hypoesthesia was recorded.
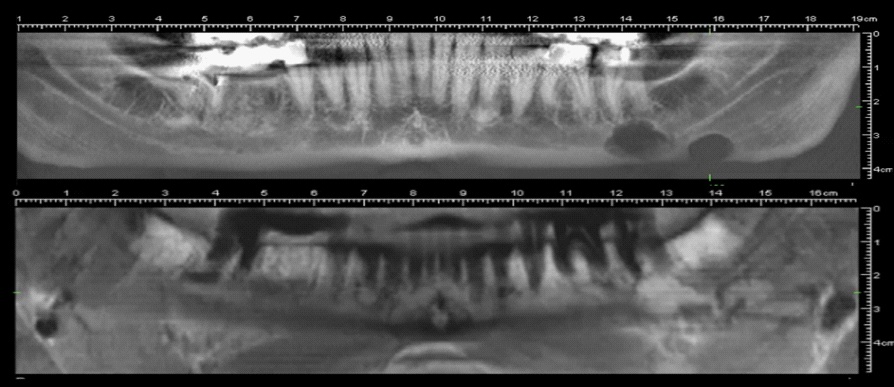
The panoramic radiograph showed two ovoid radiolucencies with well-defined peripheral borders in the lower left jaw, one apical of the second left lower molar overlaying the inferior alveolar nerve and one in area of the third left lower molar caudal of the inferior alveolar nerve.
Based on the findings in the panoramic radiograph and the positive pulp sensitivity test of the teeth in the area, the preliminary diagnosis of SBC with untypical multilocalisation was made. Differential diagnosis included traumatic or solitary bone cysts, odontogenic cyst and odontogenic tumor
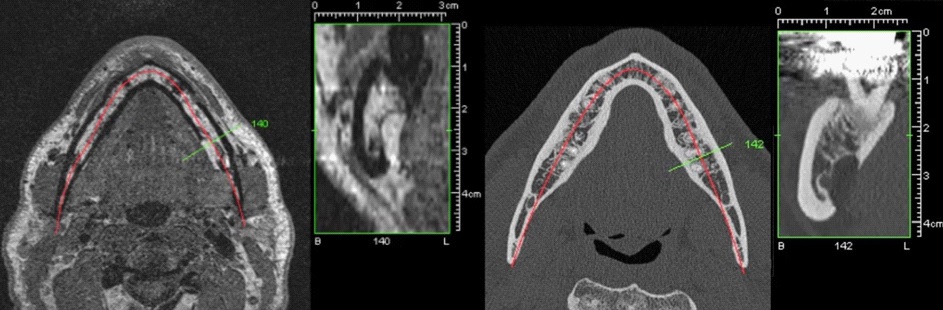
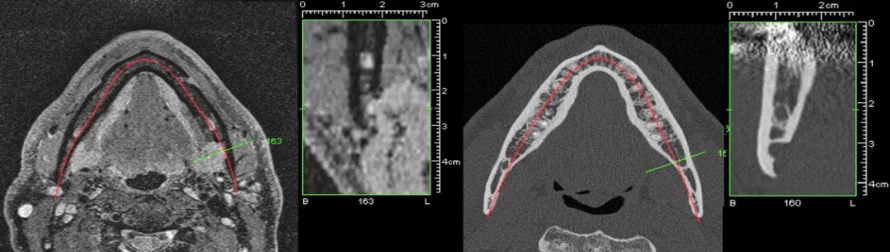
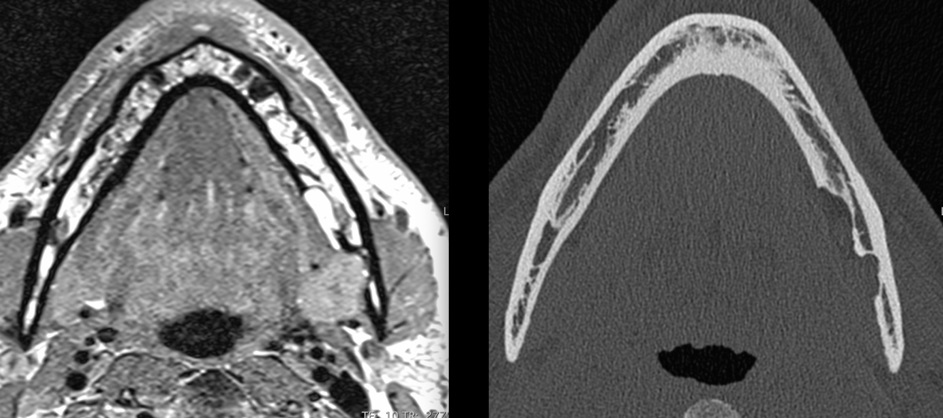
The next diagnostic step was to perform amultislice-CT scan (Definition AS, Siemens Healthineers Group, Erlangen, Germany) of the lower jaw with 0,5 mm axial slice thickness. The scan revealed two bone pits on the lingual side of the described area of the left mandible. The anterior lesion showed no cortical limitation of the inferior alveolar nerve. Due to the highly spongeous bone structure around the anterior lesion, its appearance seemed “soap bubbly”. The distal lesion showed a well-defined cortical outline without direct contact to the lower alveolar nerve. Both cavities contained soft tissue but further assessment could not be made by analyzing the CT scan.
To ensure the correct diagnosis of SBC and enable evaluation of the soft tissue contained in the cavities without surgical intervention, a MRI scan was carried out and the proton-weighted and T1 -weighted sequences were assessed. Results indicated that the soft tissue - consisting of adipose-, lymphatic- and gland-tissue was part of the left submandibular gland.
Due to the findings presented by the CT and MRI scan, differential diagnoses like cystic processes or neoplastic formations were excluded and the final diagnosis of SBC with untypical multilocular configuration without any need of surgical treatment was made.
Conclusion
In order to ensure the diagnosis of SBC after a panoramic radiograph and well performed clinical intra- and extraoral examination including sensitivity testing of the bordering teeth, a MRI scan is highly recommended to avoid invasive intervention and decrease the patient’s exposure to radiation. In case of a possible identification of a further progressed lesion, radiographic follow-up is recommended.
Declaration
Ethics approval and consent to participate: For writing and publishing this case report no ethics approval was necessary. The patient gave consent to publish his case and radiologic examinations.
Funding: This case report received no funding.
Availability of data and materials: Further information and material are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Author’s contributions: TL was involved in the design of the case report, investigation and writing the manuscript. AG, CU and AM were involved in the design of the case report, investigation and submission of the manuscript. All authors read and approved the final manuscript.
Consent for publication: Not applicable.
Acknowledgements: The authors thank Helge Schöchtner, Nadine Krier and Christopher Kerlin for their help and support with preparation of the images.
References
- Stafne EC. Bone cavities situated near the angle of the mandible. The Journal of the American Dental Association. 1942; 29: 1969– 72.
- Sisman Y, Miloglu O, Sekerci AE, Yilmaz AB, Demirtas O, Tokmak TT. Radiographic evaluation on prevalence of Stafne bone defect: a study from two centres in Turkey. Dentomaxillofac Radiol. 2012; 41: 152–8.
- Philipsen HP, Takata T, Reichart PA, Sato S, Suei Y. Lingual and buccal mandibular bone depressions: a review based on 583 cases from a world-wide literature survey, including 69 new cases from Japan. Dentomaxillofac Radiol. 2002; 31: 281–90.
- Segev Y, Puterman M, Bodner L. Stafne bone cavity--magnetic resonance imaging. Med Oral Patol Oral Cir Bucal. 2006; 11: E345-7.
- Grellner TJ, Frost DE, Brannon RB. Lingual mandibular bone defect: Report of three cases. J Oral Maxillofac Surg. 1990; 48: 288–96.
- Kopp S, Ihde S, Bienengraber V. Differential diagnosis of stafne idiopathic bone cyst with Digital Volume Tomography (DVT). J Maxillofac Oral Surg. 2010; 9: 80–1.
- Taysi M, Ozden C, Cankaya B, Olgac V, Yıldırım S. Stafne bone defect in the anterior mandible. Dentomaxillofac Radiol. 2014; 43: 20140075.
- Probst FA, Probst M, Maistreli I-Z, Otto S, Troeltzsch M. Imaging characteristics of a Stafne bone cavity--panoramic radiography, computed tomography and magnetic resonance imaging. Oral Maxillofac Surg. 2014; 18: 351–3.
- Shimizu M, Osa N, Okamura K, Yoshiura K. CT analysis of the Stafne’s bone defects of the mandible. Dentomaxillofac Radiol. 2006; 35: 95–102.
- Saglam M, Salihoglu M, Sivrioglu AK, Kara K. Multimodality imaging of Stafne bone defect. BMJ Case Rep. 2013; 2013.
- Davies RP, Whyte AM, Lui CL. Interventional sialography: a single-center experience. Cardiovasc Intervent Radiol. 1997; 20: 331–6.
- Oikarinen VJ, Kilpinen E. Developmental mandibular bone defect (Stafne) and the submandibular salivary gland. A case report with a stereosialographic study. Proc Finn Dent Soc. 1976; 72: 53–55.
- Oikarinen VJ, Wolf J, Julku M. A stereosialographic study of developmental mandibular bone defects (Stafne’s idiopathic bone cavities). Int J Oral Surg. 1975; 4: 51–4.
- Branstetter BF, Weissman JL, Kaplan SB. Imaging of a Stafne bone cavity: what MR adds and why a new name is needed. AJNR Am J Neuroradiol. 1999; 20: 587–9.
- Bornstein MM, Wiest R, Balsiger R, Reichart PA. Anterior Stafne’s bone cavity mimicking a periapical lesion of endodontic origin: report of two cases. J Endod. 2009; 35: 1598–602.
- Ozdede M. An unusual case of double stafne bone cavities. Surg Radiol Anat. 2020; 42: 543–6.
- Schneider T, Filo K, Stadlinger B, Locher M, Kruse AL, Lübbers H-T. [An atypical Stafne cavity-multi-chamber bone lesion with bucal expansion. A case report]. Swiss Dent J. 2014; 124: 545– 55.