
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Liver dysfunction in norovirus gastroenteritis in a child with cerebral palsy: A case report
Jee Hyun Suh
Department of Rehabilitation Medicine, College of Medicine, Ewha Womans University, 1071 An-YangCheon Ro, Yang-Cheon Gu, Seoul, 07985, Republic of Korea.
*Corresponding Author: Jee Hyun Suh
Department of Rehabilitation Medicine, College of
Medicine, Ewha Womans University, 1071 An-YangCheon Ro, Yang-Cheon Gu, Seoul, 07985, Republic of
Korea.
Email: suhtwins@hanmail.net
Received : Oct 13, 2021
Accepted : Nov 26, 2021
Published : Dec 03, 2021
Archived : www.jcimcr.org
Copyright : © Suh JH (2021).
Abstract
Norovirus is the common cause of gastroenteritis in humans. There is no report of liver dysfunction in children caused by norovirus infection. Baclofen has been used mainly to treat spasticity in children with cerebral palsy. Hepatotoxicity of baclofen has not been previously described in children.This report describes the case of acute liver dysfunction in the course of norovirus gastroenteritis in a child with cerebral palsy (CP) on baclofen. A 7-year 7 month-old child who diagnosed spastic quadriplegic cerebral palsy showed mild fever and diarrhea. He started taking baclofen a week before the symptom started. His illness was diagnosed as norovirus gastroenteritis, but liver dysfunction accompanied this gastroenteritis (AST/ALT 589/401 (IU/L)). He recovered completely within 2 weeks without any damage left. When a child with cerebral palsy gets norovirus enteritis while taking baclofen, it would be necessary to close monitoring for liver failure.
Keywords: norovirus; baclofen; cerebral palsy; liver dysfunction.
Citation: Suh JH. Liver dysfunction in norovirus gastroenteritis in a child with cerebral palsy: A case report. J Clin Images Med Case Rep. 2021; 2(6): 1452.
Introduction
Human norovirus, previously known as the Norwalk virus was the first virus that was identified as causing gastroenteritis in humans. Although norovirus gastroenteritis is generally mild and of short duration, new evidence suggests that the illness can be severe and sometimes fatal, especially among vulnerable populations - young children and the elderly - and is a common cause of hospitalization for gastroenteritis [1]. Its infectious potential is estimated to be very high compared to other enteroviruses such as rotavirus, adenovirus and astrovirus. The virus is sometimes thought to lead to whole-body infection. Previous case report showed a 48-year-old female with norovirus gastroenteritis underwent acute liver dysfunction [2]. And the other case report showed the liver damage caused by rotavirus infection in a child [3]. However, there is no report of liver dysfunction in children caused by norovirus infection.
Baclofen has been used mainly to treat spasticity in children with cerebral palsy. 80 to 85% of baclofen is thought to be eliminated via the kidneys without liver metabolism [4]. There are few reports about the hepatic side effects of baclofen in patients with normal hepatic and renal function. Baclofen is known as a drug with low liver toxicity to the extent that it is used to reduce alcohol dependency in patients with liver cirrhosis. Addolorato et al. [5] reported the absence of hepatotoxic effects by the significant decreased of serum transaminases in 84 alcohol-dependent adult patients with liver cirrhosis under baclofen. Furthermore, the hepatotoxicity of baclofen has not been previously described in children.
This report describes the case of acute liver dysfunction in the course of norovirus gastroenteritis in a child with cerebral palsy (CP) on baclofen. The objective of this clinical case report is to highlight this unusual liver dysfunction to avoid the delayed diagnosis and management.
This case report was approved by ethics committee of our hospital (Institutional Review Board of Bundang Jesaeng General Hospital, DMC 2020-04-002).
Case report
A 7-year 7 month-old boy who diagnosed spastic quadriplegic CP admitted to the department of rehabilitation medicine for the intensive physical therapy. The patient was born at the gestational age of 39+5 weeks, with a weight of 3.6 kg through spontaneous delivery. He had received intensive care in the neonatal intensive care unit for respiratory syncytial viral pneumonia on the 25th day of birth, and had been occurred the sudden cardiac arrest. At that time, 10 minutes of cardiopulmonary resuscitation had been performed, and there had been a return of spontaneous circulation. He had a myoclonic seizure at that time. And his brain magnetic resonance imaging had showed a bilateral basal ganglia infarction. He was given the percutaneous endoscopic gastrostomy (PEG) at 7 months of age due to dysphagia and frequent vomiting. He fed on the enteral nutrition fluid by PEG tube. The patient weighed 22.4 kg for a height of 115 cm when he admitted. He had severe limitations in head and trunk control, and required total physical assistance (Gross Motor Function Classification System level V).
He had severe spasticity (Modified Ashworth scale grade IV), and was taking dantrolene sodium (Anorex○RR) 12.5 mg and clonazepam (Rivotril○RR) 0.25 mg twice (Figure 1). These drugs had been taken for more than 6 months before the patient was hospitalized. Because the patient’s spasticity was not controlled, dantrolene sodium was cut off and baclofen (Bacron○RR) was added on the 5th day of admission. After adding baclofen, the spasticity was controlled. On the laboratory tests at the time of hospitalization, the results of the liver function test and the renal function test showed no significant abnormalities (aspartate aminotransferase (AST) 24 IU/L, Alanine aminotransferase (ALT) 15 IU/L, estimated glomerular filtration rate (eGFR) 287.50 ml/ min/1.73 m2 , Blood Urea Nitrogen (BUN) 17.8 ml/dL, creatinine 0.28 mg/dL) (Figure 1).
Table 1:Laboratory data.
|
Day 2 |
Day 14 |
Day 15 |
Day 23 |
AST (IU/L) |
24 |
589 |
159 |
28 |
ALT (IU/L) |
15 |
401 |
289 |
32 |
ESR (mm/h) |
8 |
21 |
|
6 |
CRP (mg/dL) |
<0.1 |
16.93 |
8.92 |
<0.1 |
BUN (mg/dL) |
17.8 |
31.3 |
|
14.4 |
Creatinine (mg/dL) |
0.28 |
0.62 |
|
0.30 |
eGFR (mL/min/1.73m2) |
287.50 |
129.84 |
|
268.33 |
eGFR (estimated GFR) by Original Schwartz=k * height (xm)/ Serum Cr (sCR, mg/dL)
k in adolescent boy: 0.70
AST: aspartate aminotransferase; ALT: Alanine aminotransferase; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; BUN: Blood Urea Nitrogen; eGFR: estimated glomerular filtration rate.
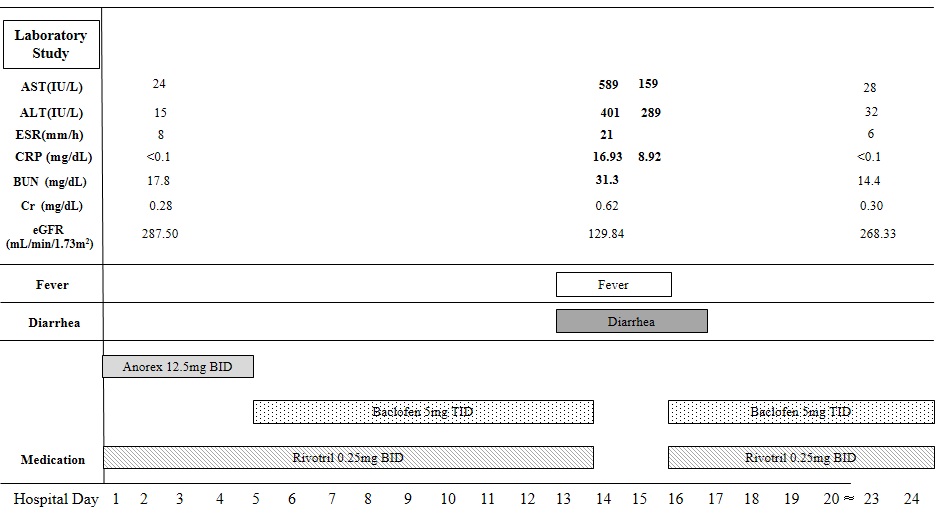
He had diarrhea with fever on the 13th day of hospitalization (Figure 1). The next day (day 14), he had a fever with 20 times of diarrhea, and conducted laboratory tests (Figure 1). Blood tests showed an increase in AST/ALT from 24/15 (IU/L) to 589/401 (IU/L) and an increase in inflammation levels from erythrocyte sedimentation rate (ESR) 21 (mm/h), C-reactive protein (CRP) 16.93 (mg/dL). No abnormalities were observed in the abdomen sonography. A nasopharyngeal swab was negative for Influenza A and B antigen. Test results for anti- Hepatitis A (HAV) immunoglobulin M (IgM), Hepatitis B surface antigen (HBs Ag), anti-Epstein-Barr virus capsid antigen (EBV VCA) IgM, Cytomegalovirus antibody (CMV Ab) IgM were negative. The result for Anti-HBs was reactive.The culture of a fecal specimen was negative for salmonella and shigella. The fecal specimen was assayed for the bacterial and viral genomes using reverse transcription–polymerase chain reaction (RT-PCR), and Norovirus G II was detected.
He was applied heptatonics and intravenous hydration, and stopped taking the anti-spasticity medications. Conservative treatment improved his clinical symptoms.And AST/ALT improved to 159/289(IU/L) on Day 11 and 28/32(IU/L) on Day 19 (Figure 1). He recovered completely within 2 weeks without any damage left.
Discussion
Norovirus gastroenteritis is known to have no serious effect on the liver function. It is also known that baclofen excretes 85% of the kidneys, and therefore does not raise AST/ALT seriously. Although each of these situations may not be able to cause significant liver dysfunction, it can cause a serious AST/ ALT elevation when two situations overlap. From this point of view, this case report has great implications. This case report suggests that when norovirus enteritis occurs in children taking baclofen, the AST/ALT level must be checked and prompt management taken.
The hypertransaminasaemia in this case can be thought of as two mechanisms. The first hypothesis is that pre-renal dysfunction was caused by multiple diarrheas due to norovirus gastroenteritis, and this may cause liver damage as the baclofen underwent the hepatic metabolism instead of the renal metabolism. The second hypothesis is that the norovirus gastroenteritis and baclofen may cause the synergic effects and cause liver dysfunction. Norovirus infection occasionally develops into pre-renal acute renal failure (ARF) as a result of the dehydration caused by severe diarrhea and vomiting. In the previous case report, there was a norovirus-associated renal ARF in a previously healthy individual [6]. Therefore, it should be noted that, even when a drug that is excreted via the kidneys is used, the flow of metabolism may be changed when renal function decrease due to norovirus infection. As mentioned in the introduction, baclofen absorption after oral administration occurs mainly in the proximal small intestine, and the kidney normally excretes the baclofen essentially unchanged, but the liver can metabolize as much as 15% of a given dose. This is why the liver function test is advisable during baclofen administration in patients with impaired renal function. In this case, eGFR was 287.50 mL/min/1.73m2 at day 2, and was reduced to 129.84 mL/min/1.73m2 at day 13 when the gastroenteritis occurred. This suggests the possibility of pre-renal dysfunction has occurred, which may have caused problems with renal metabolism of baclofen. This would have led to the hepatic metabolism of baclofen. The pre-renal dysfunction would have been resolved by intravenous rehydration, which would have improved the liver dysfunction. However, the level of eGFR on Day 13 is 129.84 mL/min/1.73m2 , which is in the normal range. So, the first hypothesis does not fully explain the cause of the liver dysfunction. Therefore, the second hypothesis, norovirus gastroenteritis and baclofen caused the synergistic effect, which is not negligible.
Conclusion
In conclusion, the present case alerts us to the presence of liver dysfunction with norovirus gastroenteritis in a cerebral palsy child on baclofen. If a child with cerebral palsy gets norovirus enteritis while taking baclofen, it will be necessary to check for liver failure.
Declarations
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.
References
- Glass RI, Parashar UD, Estes MK. Norovirus gastroenteritis. N Engl J Med. 2009; 361: 1776-1785.
- Nakajima H, Watanabe T, Miyazaki T, et al. Acute liver dysfunction in the course of norovirus gastroenteritis. Case Rep Gastroenterol. 2012; 6: 69-73.
- Venuta A, Bertolani P, Mazzali E, Berri R, Balli F. Acute hepatitis in course of rotavirus gastroenteritis: a case report. Pediatr Med Chir. 2005; 27: 41-42.
- Anton RF, O’Malley SS, Ciraulo DA, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006; 295: 2003-2017.
- Addolorato G, Leggio L, Ferrulli A, et al. Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver cirrhosis: randomised, double-blind controlled study. Lancet. 2007; 370: 1915-1922.
- Kanai T, Yotsumoto S, Momoi MY. Norovirus-associated renal acute renal failure with nephrotic syndrome. Pediatr Int. 2010; 52: e23-25.Figure 1: Laboratory data, drug history and clinical course of the case.