
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Case of Geotrichum capitatum septicemia successfully resolved by the use of liposomal amphotericin B in a patient with acute myeloid leukemia
Ernesto Vigna1; Daniele Caracciolo1; Daniela Perugini2; Enrica Martino1; Francesco Mendicino1; Eugenio Lucia1; Cirino Botta1; Rosellina Morelli3; Angelo Barbato4; Francesca Greco2; Massimo Gentile1*
1 Hematology Unit, AO of Cosenza, Cosenza, Italy
2 Microbiology and Virology Unit, AO of Cosenza, Cosenza, Italy
3 Internal Medicine Department, AO of Cosenza, Cosenza, Italy.
4 Direzione Sanitaria, AO of Cosenza, Cosenza, Italy.
*Corresponding Author: Massimo Gentile
Hematology Unit, AO of Cosenza, Italy.
Email: massim.gentile@tiscali.it
Received : Dec 03, 2021
Accepted : Jan 11, 2022
Published : Jan 18, 2022
Archived : www.jcimcr.org
Copyright : © Gentile M (2022).
Abstract
Background: Geotrichum capitatum infection is a rare condition and it has only been reported in immune-compromised patients. The prognosis is poor, with a mortality rate between 50-90%.
Case presentation: Here we report a case of Geotrichum capitatum septicemia in a neutropenic patient undergoing induction chemotherapy for acute myeloblastic leukemia. At day +24 from the beginning of chemotherapy, the patient’s blood cultures were positive for Geotrichum capitatum. When we received the antimicogram a therapy with liposomal amphotericin B (3 mg/kg/day) was started. After 15 days of antifungal treatment, the patient’s clinical condition had dramatically improved and at the twenty-first day of antifungal treatment the blood culture was negative for Geotrichum capitatum. On day +47 from the start of induction, the patient died in hematological remission of AML due to sudden death. An autopsy was not performed.
Conclusion: This clinical case highlights the emergence of Geotrichum capitatum as an opportunistic fungus in Italian leukemia patients. Moreover, our case report shows how liposomal amphotericin B could represent an effective therapeutic approach for these infections. Further studies are needed to shed more light on these rare fungal infections, in order to define the best therapeutic approach towards invasive geotrichosis.
Keywords: geotrichum capitatum; fungemia; neutropenia; acute myeloid leukemia.
Citation: Vigna E, Caracciolo D, Perugini D, Martino E, Gentile M, et al. Case of Geotrichum capitatum septicemia successfully resolved by the use of liposomal amphotericin B in a patient with acute myeloid leukemia. J Clin Images Med Case Rep. 2022; 3(1): 1581.
Background
Invasive fungal infections are the major cause of morbidity and mortality in cancer patients treated with intensive chemotherapeutic regimens [1-3]. Although Candida and Aspergillus species are still the most frequent causes of invasive fungal infections in this setting of patients, less common fungi are becoming a real clinical emergency due to their increasing incidence and limited treatment options [4-7]. Invasive Geotrichum capitatum infection is relatively rare, as approximately 100 cases have been reported in patients with hematological malignancies [2,8-11]. It causes septicemia with occasional secondary localizations [2,11]. Despite adequate antifungal therapy, the disease has been associated with an unfavorable outcome and a mortality rate greater than 50% [6,7]. Here we report a case of Geotrichum capitatum septicemia successfully resolved by the use of liposomal amphotericin B in a patient with acute myeloid leukemia (AML) in complete hematological remission.
Case report
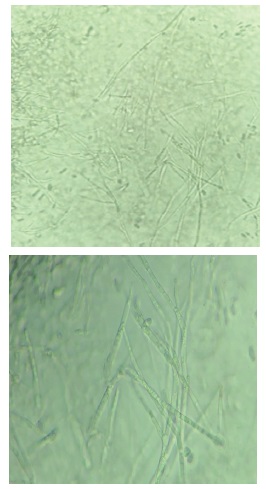
A 69-year-old woman is hospitalized in October 2017 in our Onco-Hematology department for worsening asthenia and repeated episodes of epistaxis. On the advice of the general practitioner, she performed a hemogram that documented a severe leukocytosis, anemia and thrombocytopenia. The careful collection of the patient’s anamnestic data had highlighted many comorbidities such as hypertension, previous hepatitis B infection and type 2 diabetes. The cytomorphological examination of peripheral venous blood smear, performed at the entrance to the department, documented about 30% of myeloid blasts. For these reasons, a bone marrow aspirate was performed, allowing to formulate the diagnosis of AML; indeed, about 80% of myeloid blasts were evident at the morphologic examination. Immunophenotyping by flow cytometry revealed blast cells expressing myeloid markers CD33+ CD117+ CD34+/- CD56-/+ HLADR+. Preliminary routine examinations before induction chemotherapy, were performed: 1) X-ray of the chest was negative; 2) electrocardiogram showed a sinus rhythm; 3) echocardiogram showed a left ventricular ejection fraction of 75%. Therefore, the patient started induction chemotherapy according to the “3 + 7” protocol (idarubicin 12 mg/m2 /day for 3 days and cytarabine 100 mg/m2 / day for 7 days). During the induction patient received 200 mg three times a day of posaconazole as antifungal prophylaxis. On day +16 from the start of induction therapy, the patient presented many febrile episodes (39°C) without further clinical signs; at that time, the patient showed a severe neutropenia [polymorphonuclear neutrophils (PMNs) 0/mm3 ). In consideration of the clinical case, empiric therapy was set up with piperacillin/tazobactam and amikacin. After 4 days of antibiotic therapy the patient did not show any clinical improvement, moreover she presented a new clinical sign such as dry cough. Thus, the empiric antibiotic therapy was implemented, and the glycopeptide (teicoplanin) was added. High resolution computed tomography (HRTC) did not show pleuro-parenchymal anomalies, serial blood culture as well as Aspergillus galactomannan antigenemia were both negative. Therefore, in consideration of the severity of patient’s clinical conditions and due to the persistence of fever (39°C), we decided to stop therapy with piperacillin/tazobactam and amikacin and carbapenem infusion (meropenem, 1 gr 3 times a day) was started. On day +23 from the start of induction chemotherapy, the patient continued to remain persistently febrile, but there was an initial hematological improvement (PMNs 500/mm3 ). HRTC of the chest was repeated, showing a pleural biliary effusion. At day +24, when patient showed a hematological recovery, (WBC 2700/mm3 , with PMNs 1700/mm3 ), the positivity of the blood cultures for Enterococcus faecium and Geotrichum capitatum (Figures 1-3) was communicated by the microbiology laboratory (see supplementary data). In light of these data liposomal amphotericin B (3 mg/kg/day) was added to therapy and antifungal prophylactic therapy with posaconozole was stopped.

At day +25 on the basis of both the antibiogram for Enterococcus faecium and the antimicrogram for Geotrichum capitatum (see Table 1&2) the antibiotic therapy was modified by adding tigecycline to liposomal amphotericin B.
On day +32 from the start of induction corresponding to day +7 of the antifungal treatment, blood cultures were still positive for Geotrichum capitatum and Enterecoccus faecium. After 15 days of antifungal treatment, the patient’s clinical condition had dramatically improved. On day +38 from the start of induction, corresponding to the twenty-first day of antifungal treatment, the blood cultures were still positive for Enterococcus faecium, but negative for Geotrichum capitatum. The patient continued to receive tigecycline, meropenem and amphotericin B. The dose of amphotericin B was reduced at 1 mg/Kg/day for the comparison of hyperbilirubinemia, which was rapidly resolved. On day +47 from the start of induction, the patient died in hematological remission of AML due to sudden death. An autopsy was not performed.
Table 1: The sensitivity spectrum for Enterococcus faecium isolate with interpretation according to European Committee on Antimicrobial Susceptibility Testing (EUCAST).
Antifungal agent tested |
MIC (mg/mL) |
Judgement |
ampicillin |
>32 |
resistant |
ampicillin/sulbactam |
>32 |
resistant |
vancomycin |
32 |
resistant |
teicoplanin |
32 |
resistant |
imipenem |
>16 |
resistant |
gentamicin (high dose) |
|
resistant |
streptomycin (high dose) |
|
resistant |
linezolid |
2 |
sensitive |
tigecycline |
<=0.12 |
sensitive |
quinupristin/dalfopristins |
0.5 |
sensitive |
Table 2: Susceptibility testing for Geotrichum capitatum isolate.
Antifungal agent tested |
MIC (mg/mL) |
anidulafungin |
8 |
caspofungin |
32 |
amphotericin B |
1 |
fluconazole |
1.5 |
itraconazole |
0.5 |
micafungin |
32 |
posaconazole |
0.5 |
voriconazole |
2 |
Discussion
Geotrichum capitatum systemic infections in patients with hematological malignancies are rare compared to invasive aspergillosis and candidiasis [1,2,6,8]. Risk factors include deep and prolonged neutropenia, the use of broad-spectrum antibiotics, cytotoxic chemotherapy and various venous access devices [1,4,9]. Most of these predisposing factors were present in our patient; in fact, for her AML she received chemotherapy which determined a prolonged and profound neutropenia. She had also been treated with broad-spectrum antibiotics for presumed bacterial sepsis.
Geotrichum capitatum (previously identified as Trichosporon capitatum or Blastoschizomyces capitatus) is known to be a saprophyte of the digestive and respiratory tract and human skin, which can be potential gates of entry for the germ capable of generating a septic state [1-3]. However, in our patient it was not possible to define which was the possible way of entry of the germ. Overall, the clinical presentation of geotrichosis is very similar to that of other invasive fungal infections. Most often, geotrichosis starts as a fever that does not respond to antibiotics [5,6]. Involvement of deep organs, such as skin and digestive mucosa, occurs in 60-80% of patients [10-12]. In our patient, the diagnosis of the disease was made through the positivity of 2 blood cultures. The treatment and outcome of Geotrichum capitatum infection depend both on extension of the infection and on the functional capacity of the host’s immune system [8,9,11]. In early publications, the rarity of the disseminated disease of Geotrichum capitatum has been attributed at least in part to the low virulence of the fungus [8,9,11]. A further study has shown that the prognosis of disseminated Geotrichum capitatum infection is very poor, with a mortality rate of over 50% despite antifungal therapy [6,7,13,14]. Treatment of Geotrichum capitatum infection is not completely clear, although the combination of amphotericin B and flucytosine are apparently the most effective regimens. Voriconazole and micafungine have been found to be effective in some case reports [8,15-17]. In our case, the patient, who had achieved a complete hematological recovery and the remission of AML, was treated with liposomal amphotericin B for 3 consecutive weeks. This antifungal treatment was found to be effective in resolving the infection.
Conclusion
This clinical case highlights the emergence of Geotrichum capitatum as an opportunistic fungus in Italian leukemia patients. Moreover, although caspofungin has been established as the empirical antifungal therapy, particular attention should be given to management of cases with infections due to newly evolving pathogens.
Furthermore, this case also shows how important is the hematological recovery in resolving the infection. Finally, our case report shows how liposomal amphotericin B could represent an effective therapeutic approach for these infections. Further studies are needed to shed more light on these rare fungal infections, in order to define the best therapeutic approach to invasive geotrichosis.
Declarations
Availability of data and material: All available information is contained within the manuscript.
Acknowledgements: We thank the patient for granting us permission to publish this information.
Author contributions : EV and MG had full access to all of the data of this case and take responsibility for the integrity and accuracy of the data. Concept and design: EV, MG, DB, FG and DC. Acquisition, analysis, or interpretation of data: all authors. Drafting of the manuscript: EV, MG, DB, FG and DC. Critical revision of the manuscript for important intellectual content: all authors. Supervision: EV and MG.
Funding: This manuscript was not funded.
Conflict of interest: On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Consent for publication: Written informed consent was obtained from the patient for publication of this case and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
References
- Martino P, Venditti M, Micozzi A, Morace G, Polonelli L, Mantovani MP, et al. Blastoschizomyces capitatus: an emerging cause of invasive fungal disease in leukemia patients. Rev. Infect. Dis. 1990; 12: 570-582. https://doi.org/10.1093/clinids/12.4.570.
- Shiemann R, Glasmacher A, Bailly E, Horré R, Molitor E, Leutner C. et al. Geotrichum capitatumsepticaemia in neutropenic patients: case report and review of the literature. Mycoses. 1998; 41: 113-116. https://doi.org/10.1016/S0248-8663(98)80868-0.
- Fouassier M, Joly ., Cambon M, Peigue-Lafeuille H, Condat P. Geotrichum capitatum infection in a neutropenic patient, case report and review of the literature. Rev Med Interne. 1998; 19: 431-433. https://doi.org/10.1016/S0248-8663(98)80868-0.
- Koll BS, Brown AE. Changing patterns of infections in the immuno-compromised patient with cancer. Hematol Oncol Clin North Am. 1993; 7: 753-769. PMID: 8354655.
- Martino R., Subirà, .M. Invasive fungal infections in hematology: new trends. Ann Hematol. 2002; 81: 233–243. https://doi. org/10.1007/s00277-002-0466-3.
- Krcmery V, Krupova I, Denning D.W. Invasive yeast infections other than Candida spp in acute leukaemia. J Hosp Infect. 1999; 41: 181-194. https://doi.org/10.1016/S0195-6701(99)90015-4.
- Rolston K. Overview of systemic fungal infections. Oncology (Huntingt). 2001; 15: 11-14. PMID: 11757845.
- Pérez-Sanchez I, Anguita J, Martín-Rabadan P, Muñoz P, Serrano D, Escudero A. et al. Blastoschizomyces capitatus infection in acute leukemia patients. Leuk Lymphoma. 2000; 39: 209-212. https://doi.org/10.3109/10428190009053556.
- Gadea I, Cuenca-Estrella M, Prieto E, Diaz-Guerra TM, GarciaCia JI, Mellado E. et al. Genotyping and antifungal susceptibility profile of Dipodascus capitatus isolates causing disseminated infection in seven hematological patients of a tertiary hospital. J. Clin. Microbiol. 2004; 42: 1832-1836. 10.1128/jcm.42.4.1832- 1836.2004.
- Viscoli C, Girmenia C, Marinus A, Collette L, Martino P, Vandercam B. et al. Candidemia in cancer patients: a prospective, multicenter surveillance study by the invasive fungal infection group (IFIG) of the european organization for research and treatment of cancer (EORTC). Clin Infect Dis. 1999; 28: 1071- 1079. https://doi.org/10.1086/514731.
- Martino R, Salavert M, Parody R, Tomás JF, de la Cámara R, Vázquez L. et al. Blastoschizomyces capitatus infection in patients with leukemia: report of 26 cases. Clin Infect Dis. 2004; 38: 335-341. https://doi.org/10.1086/380643.
- Arnold AG, Gribbin B, Deleval M, Mac Artney F, Slack M. Trichosporon capitatum causing fungal endocarditis. Thorax. 1981; 36: 478-480. PMID: 7198299.
- Krcmery V, Jr, Mateicka F, Kunová A, Spánik S, Gyarfás J, Sycová Z. et al. Hematogenous trichosporonosis in cancer patients: report of 12 cases including 5 during prophylaxis with itraconazole. Supportive Care in Cancer. 1999; 7: 39-43. https://doi. org/10.1007/s005200050221.
- Segal BH, Bow EJ, Menichetti F. Fungal infections in nontransplant patients with hematologic malignancies. Infectious Disease Clinics of North America. 2002; 16: 935-964. https://doi. org/10.1016/S0891-5520(02)00043-0.
- Ikuta K, Torimoto Y, Yamamoto M, Okamura N, Hosoki T, Sato K. et al. Successful treatment of systemic Geotrichum capitatum infection by liposomal amphotericin-B, itraconazole, and voriconazole in a Japanese man. Intern. Med. 2010; 49: 2499- 2503. https://doi.org/10.2169/internalmedicine.49.3887.
- Etienne A, Datry A, Gaspar N, Morel V, Delabesse E, Lmimouni B. et al. Successful treatment of disseminated Geotrichum capitatum infection with a combination of caspofungin and voriconazole in an immunocompromise patient. Mycoses. 2008; 51: 270-272. https://doi.org/10.1111/j.1439-0507.2007.01484.x.
- Fianchi L, Montini L, Caira M, Voso MT, Maviglia R, Posteraro B, et al. Combined voriconazole plus caspofungin therapy for the treatment of probable Geotrichum pneumonia in a leukemia patient. Infection. 2008; 36: 65-67. https://doi.org/10.1007/ s15010-007-6235-4.
- Salih Z, Cavet J, Dennis M, Somervaille T, Bloor A, Kulkarni S. Prognostic factors for mortality with fungal blood stream infections in patients with hematological and non-hematological malignancies. South Asian J. Cancer. 2013; 220-224.