
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Association of age with depth of invasion and extra capsular spread in patients with oral squamous cell carcinoma: A retrospective study
Shafqat Ali Shaikh1*; Syed Akbar Abbas2; Bushra Ayub3; Muhammad Ehteramul Haq3; Talha Ahmed Qureshi1; Amna Khalil4
1 Department of Otolaryngology and Head & Neck Surgery, Patel Hospital, Karachi, Karachi City, Sindh 75300, Pakistan.
2 Department of Otolaryngology and Head & Neck Surgery National Stadium Rd, Aga Khan University Hospital, Karachi, Karachi City, Sindh 74800, Pakistan.
3 Department of Surgery and Allied, Patel Hospital, ST-18, Block 4 Gulshan-e-Iqbal, Karachi, Karachi City, Sindh 75300, Pakistan.
4 Department of Otolaryngology and Head & Neck Surgery, Dow University of Health Sciences, Karachi, Karachi City, Sindh 74200, Pakistan.
*Corresponding Author: Shafqat Ali Shaikh
Department of Otolaryngology and Head & Neck
Surgery, Patel Hospital, ST-18, Block 4 Gulshan-e-Iqbal,
Karachi, Karachi City, Sindh 75300.
Email: alishafqat17@yahoo.com
Received : Nov 24, 2021
Accepted : Jan 12, 2022
Published : Jan 19, 2022
Archived : www.jcimcr.org
Copyright : © Shaikh SA (2022).
Abstract
Introduction: Oral malignancy is most common tumors in Pakistan. The age of the greater part of the patient’s reaches somewhere in the range of 50 and 70 years and old age is an indirect risk factor for malignant growths. It is challenging to treat the older patients with oral squamous cell carcinoma due to poor performance and the adjusted physiology and the additional comorbidities that may influence the decision of surgery and adjuvant treatment, whenever scheduled. Above mentioned factors in elderly group might affect the option of treatment and may vary from the ideal treatment. We aim to evaluate the association of age with depth of invasion and to assess the association of age with extra capsular spread and risk factors in patients with oral cancer.
Material/Methods: This is a retrospective study. Total 360 patients underwent the surgery from 2011 to 2017 of which 260 patients fulfilled the inclusion criteria for our study. The chi-square test was applied to check the association between ages with a depth of invasion of tumor.
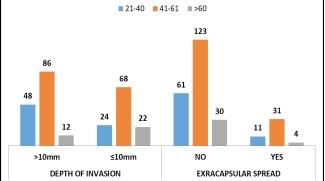
Results: There were 260 patients who underwent treatment for oral cancer it was subdivided in 3 age groups and multiple addictions are most common in every age group 51% (n=133). Majority of the patients had final stage III and IVA with 31% (n=80) and 35% (n=92). Age has a significant association with the depth of invasion, about 56% (n=144) has >10 mm depth of invasion of tumor with 95% of CI (P-value=0.01). There was no extracapsular spread in 82% (n=214) and yes in 18% (n=46) of the patients with 95% of CI (p-value= 0.149) which was insignificant in patients with oral cancer.
Conclusion: This study shows that oral cancer has increased depth of invasion in younger population as compared to elderly population and there is no association between age and extracapsular spread in patients. Majority of patients were found to have moderately differentiated oral cancer.
Keywords: oral squamous cell carcinoma; extra capsular spread; depth of invasion; head and neck neoplasms.
Citation: Shaikh SA, Abbas SK, Ayub B, Haq ME, Qureshi TA, et al. Association of age with depth of invasion and extra capsular spread in patients with oral squamous cell carcinoma: A retrospective study. J Clin Images Med Case Rep. 2022; 3(1): 1590.
Introduction
The incidence of cancer affecting different systems is rapidly rising. The epidemiology varies as per the site of disease. One such rapidly rising cancer is oral cancer. It is the most common cancer in Pakistan and in Asia; it is the sixth most frequent malignancies. According to the previous literature, each year around 274, 3000 cases of oral cancers arise [1]. There is a high incidence of oral cancers in our region due to easy availability and widely consumption of chewable tobacco [2].
The vast majority of the HNSCC patient’s reaches somewhere in the range of 50 and 70 years, the mean age was 51 – 55 years. The malignancy registry of slovenia has shown a constant rise in the level of new HNSCC cases analyzed in the age group of 70 years: 17.9% in 1981–1990; 16.5% in 1991–2000; and 22.3% in 2001–2008 [3]. Age is an indirect risk factor for cancers [4]. Treating the older patients with oral cancers is challenging because of poor performance status, the altered physiology and the added comorbidities that might affect the choice of surgical procedure and adjuvant treatment if planned in these patients [5]. Above mentioned factors in elderly group might affect the option of treatment and may vary from the ideal treatment. We believe that there is no direct relation of prognosis in HNSCC with age and hence plan to conduct this study to analyze the impact of age on various clinic-pathological parameters, treatment completion and subsequent survival in older patients [5]. We aim to evaluate the association of age with depth of invasion in patients of squamous cell carcinoma of oral cavity and to assess the association of age with extracapsular spread and risk factors in oral squamous cell carcinoma patients.
Materials and methods
This is a retrospective study, led at the branch of otolaryngology, head and neck a medical procedure in a Tertiary consideration arrangement for length of a half year in which clinical graphs were surveyed of all patients conceded in medical clinic with an essential determination of oral squamous cell carcinoma from 2011 to 2017, patients were followed for till consummation of their therapy followed by no recurrence for 1 year or till mortality during the period.
Total 360 patients went through the surgical procedure of oral squamous cell carcinoma from 2011 to 2017 of which 260 patients satisfied the consideration standards for our investigation; we separated patients into three sub-groups old enough 21 to 40 years, 41 to 60 years and over 60 years. We chose patients of the both sex from age 20 to 80 years. Patients with biopsy-demonstrated oral squamous cell carcinoma that incorporate lips, tongue, hard palate, alveolar edge, retro-molar trigone, buccal mucosa and floor of the mouth were remembered for the investigation. Recurrence after therapy and those that didn’t survive until the completion of study were additionally included for the investigation. Patients with non-squamous cell carcinoma on histology or second primaries or recurrence of disease or squamous cell carcinoma of the site other than oral cavity or carcinoma in situ or beforehand disease treated outside Patel hospital and those with follow up of under a half year were eliminated from the study.
Patients after careful extraction of the tumor with the individuals who required radiotherapy or chemotherapy were shifted to another tertiary consideration clinic additionally included. Head and Neck Cancer library structure was utilized for information assortment after we survey the patient’s clinical record documents. Subtleties of the histopathology report (pathologist TNM stage, tumor type, tumor size, grade, and edge, profundity of intrusion, Perineural invasion, bony invasion, muscle involvement, and extra capsular spread) were noted for every understanding. Patients were arranged by AJCC eighth release TNM organizing.
The Information with respect to different segment information, surgical procedure, clinical elements, and tumor staging, radiation and chemotherapy contemplated. Follow up subtleties of the relative multitude of patients were recorded till December 2018. Observation will be made as far as the presence or nonappearance of local or distant metastasis.
Descriptive statistics were used to sum up the information. Demographic variables were summed up in expressions of mean ± standard deviation for quantitative factors. Percentages and frequencies were used to sum up qualitative variables. The chi-square test was applied to check the relationship of ages with depth of invasion of tumor. A p-value less than 0.05 were considered as significant. The examination was finished utilizing SPSS version 21. Study was directed after morals survey panel endorsement number 62.
Results
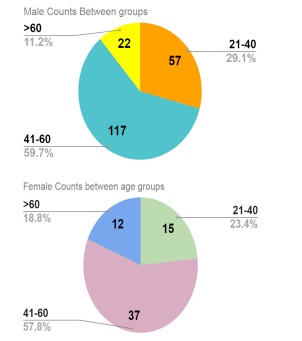
There were 260 patients who underwent treatment for oral squamous cell carcinoma of which 75% (n=196) were males and 25% (n=64) were females as shown in (Figure 1). It was subdivided in 3 age groups as seen in Table 1. It was found that multiple addictions are most common in every age group 51% (n=133) but in the sub age group of greater than 60 years people have almost equal prevalence of multiple addiction and Pan. Most common site of tumor in our patients was cheek 55% (n=143) followed by tongue 24% (n=62).
Table 1:
|
21-40 n(72) |
41-60 (n=154) |
>60 (n=34) |
Total count (%) |
|
GENDER OF THE PATIENT |
MALE |
57 |
117 |
22 |
196(75%) |
FEMALE |
15 |
37 |
12 |
64(25%) |
|
HABITUAL HISTORY |
NONE |
8 |
18 |
3 |
29(11%) |
SMOKING |
2 |
10 |
1 |
13(5%) |
|
PAN |
5 |
35 |
13 |
53(20%) |
|
SUPARI/CHALIA |
9 |
8 |
2 |
19(7%) |
|
MULTIPLE |
43 |
76 |
14 |
133(51%) |
|
OTHERS |
5 |
7 |
1 |
13(5%) |
|
PRIMARY SITE OF TUMOR |
TONGUE |
22 |
30 |
10 |
62(24%) |
CHEEK |
39 |
91 |
13 |
143(55%) |
|
LOWER ALVEOLAR RIDGE |
2 |
13 |
4 |
19(7%) |
|
UPPER ALVEOLAR RIDGE |
3 |
3 |
1 |
7(3%) |
|
HARD PALATE |
1 |
3 |
0 |
4(1%) |
|
RETROMOLAR AREA |
0 |
7 |
1 |
8(3%) |
|
SOFT PALATE |
0 |
4 |
0 |
4(1%) |
|
MANDIBLE |
5 |
3 |
3 |
11(4%) |
|
FLOOR OF MOUTH |
0 |
0 |
2 |
2(0.8%) |
|
TUMOR GRADE |
WELL DIFFERENTIATED |
9 |
40 |
8 |
57(22%) |
MODERATELY DIFFERENTIATED |
54 |
100 |
25 |
179(69%) |
|
POORLY DIFFERENTIATED |
9 |
14 |
1 |
24(9%) |
|
DEPTH OF INVASION |
>10 mm |
48 |
86 |
12 |
146(56%) |
<=10 mm |
24 |
68 |
22 |
114(44%) |
|
EXRACAPSULARSPREAD |
NO |
61 |
123 |
30 |
214(82%) |
YES |
11 |
31 |
4 |
46(18%) |
|
FINAL_STAGE |
I |
1 |
9 |
1 |
11(4%) |
II |
13 |
19 |
9 |
41(16%) |
|
III |
22 |
47 |
11 |
80(31%) |
|
IVA |
26 |
56 |
10 |
92(35%) |
|
IVB |
10 |
23 |
3 |
36(14%) |
|
TREATMENT |
OPTIMAL |
44 |
94 |
20 |
158(61%) |
SUB-OPTIMAL |
28 |
60 |
14 |
102(39%) |
|
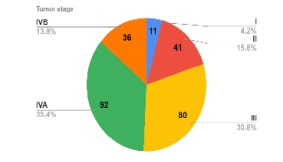
On final histopathological reports, tumor grade that was most prevalent in our study is moderately differentiated carcinoma 69% (n= 179) followed by well differentiated 22% (n=57). Majority of the patients in our study had final stage III and IVA with 31% (n=80) and 35% (n=92) respectively (Figure 2). According to our study we observed that patients who underwent complete treatment (surgery and completed adjuvant therapy course successfully) were 61% (n=158).
Table 2: Association of DOI and Extracapsular spread between age groups.
|
Count (%) |
P-Value |
|
DEPTH OF INVASION |
>10 mm |
146(56%) |
0.01 |
<=10 mm |
114(44%) |
||
EXRACAPSULARSPREAD |
NO |
214(82%) |
0.149 |
YES |
46(18%) |
||
Discussion
According to our study we observe that age has a significant association with the depth of invasion of tumors, from the data we can conclude that there is an increased depth of invasion of tumor in patients less than 60 years old. Oral squamous cell carcinoma in our demographics is more prevalent in males compared to females and the majority of the tumors were moderately differentiated with stage III and IV, this could be possibly due to increase in exposure of risk factors in males compared to females but further studies would be needed to show association.
Most common site of tumors is the cheek in our demographics followed by the tongue which is different from the studies conducted [6-10]. It can also be concluded that elderly population has almost equal prevalence of pan and multiple addiction as opposed to multiple addiction in younger population.
According to the study depth of tumor invasion is an important factor in determining the prognosis of patients [12,13] so increasing depth of invasion depicts poor prognosis in patients. According to our study we observed that patient younger than 60 years old have greater depth of invasion at the time of presentation as compared to elderly population which according to studies conducted showed that oral squamous cell carcinoma is more aggressive in younger population compared to elderly population [11,14] similar to our study which shows increase depth on invasion in younger population.
According to the study, the majority of the patients have no extracapsular spread be seen in a patient and there is no association of age with extracapsular spread in patients with oral squamous cell carcinoma.
This study is unique as there has been no study conducted in our demographics which shows the association of age with depth of invasion of tumor and extracapsular spread. It also shows that younger patients are at increased risk of aggressive squamous cell carcinoma and should be aggressively treated. This study was conducted in one of the tertiary care setup with majority of population representation from Sindh, Baluchistan and Afghanistan with low to mid socioeconomic status so data about higher socioeconomic status and other parts of the country cannot be predicted from the study. It is a retrospective study. Further studies are needed to be conducted in different regions and with population representation from higher socioeconomic status, prospective studies are needed to determine various factors for association of age with increase depth of invasion including genetics and other risk factors. Study needs to be conducted in a wider population with large sample size to have precision in results.
This study highlights the importance of setting up an early screening guideline for oral squamous cell carcinoma in younger population as tumor behavior is aggressive in young compared to elderly. It also shows that tumors in younger populations should be resected with wide margins due to increased depth of invasion. Younger patients should have aggressive management of oral squamous cell carcinoma to prevent further morbidity and mortality in patients.
Conclusion
This study shows that oral squamous cell carcinoma has increased depth of invasion in younger population as compared to elderly population. It also shows that there is no association between age and extracapsular spread in patients. Majority of patients were found to have moderately differentiated oral squamous cell carcinoma with increased prevalence in the male gender.
References
- Rao SVK, Mejia G, Roberts Thomson K, Logan R. Epidemiology of oral cancer in Asia in the past decade-an update (2000-2012). Asian Pacific journal of cancer prevention. 2013; 14: 5567-5577.
- Akshat Malik AM, Prashant Chopda, Hitesh Singhvi, Sudhir Nair, Deepa Nair, et al. Impact of age on elderly patients with oral cancer. European Archives of Oto-Rhino-Laryngology. 2018; 9.
- Koch WM, Patel H, Brennan J, Boyle JO, Sidransky D. Squamous cell carcinoma of the head and neck in the elderly. Archives of Otolaryngology Head & Neck Surgery. 1995; 121: 262-265.
- Swaminathan D, Swaminathan V. Geriatric oncology: Problems with under-treatment within this population. Cancer biology & medicine. 2015; 12: 275.
- Malik A, Mishra A, Chopda P, Singhvi H, Nair S, Nair D, et al. Impact of age on elderly patients with oral cancer. European Archives of Oto-Rhino-Laryngology. 2019; 276: 223-231.
- Viana TSA, de Barros Silva PG, Pereira KMA, Mota MRL, Alves APNN, de Souza EF, et al. Prospective evaluation of quality of life in patients undergoing primary surgery for oral cancer: Preoperative and postoperative analysis. Asian Pacific journal of cancer prevention: APJCP. 2017; 18: 2093.
- Müller S, Pan Y, Li R, Chi AC. Changing trends in oral squamous cell carcinoma with particular reference to young patients: 1971-2006. The Emory University experience. Head Neck Pathol. 2008; 2: 60–66.
- Abdulla R, Adyanthaya S, Kini P, Mohanty V, D’Souza N, Subbannayya Y. Clinicopathological analysis of oral squamous cell carcinoma among the younger age group in coastal Karnataka, India: A retrospective study. J Oral Maxillofac Pathol. 2018; 22: 180–187.
- Pires FR, Ramos AB, Oliveira JB, Tavares AS, Luz PS, Santos TC, et al. Oral squamous cell carcinoma: Clinicopathological features from 346 cases from a single oral pathology service during an 8-year period. J Appl Oral Sci. 2013; 21: 460–467.
- Jerjes W, Upile T, Petrie A, et al. Clinicopathological parameters, recurrence, locoregional and distant metastasis in 115 T1-T2 oral squamous cell carcinoma patients. Head Neck Oncol. 2010; 2: 9.
- Jones J, Lampe H, Cheung H. Carcinoma of the tongue in young patients. The Journal of otolaryngology. 1989; 18: 105-108.
- Caldeira PC, Soto AML, de Aguiar MCF, Martins CC. Tumor depth of invasion and prognosis of early-stage oral squamous cell carcinoma: A meta-analysis [published online ahead of print, 2019 Sep 14]. Oral Dis. 2019; 10.
- Németh Z, Velich N, Bogdan S, Ujpál M, Szabó G, Suba ZS. The prognostic role of clinical, morphological and molecular markers in oral squamous cell tumors. Neoplasma. 2005; 52: 95–102.
- Hilly O, Shkedy Y, Hod R, Soudry E, Mizrachi A, Hamzany Y, et al. Carcinoma of the oral tongue in patients younger than 30 years: Comparison with patients older than 60 years. Oral oncology. 2013; 49: 987-990.