
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Infective endocarditis misdiagnosed as cANCA – associated vasculitis
Jakub Strzelczyk1*; Cezary Szmigielski1; Radosław Wilimski2; Adam Arendarczyk2; Grzegorz Styczyński1
1 Department of Internal Medicine, Hypertension and Angiology, Medical University of Warsaw, Stefana Banacha Street 1A, 02-097, Warsaw, Poland
2 Department of Cardiac Surgery, Medical University of Warsaw, Stefana Banacha Street 1A, 02-097, Warsaw, Poland.
*Corresponding Author: Jakub Strzelczyk
Department of Internal Medicine, Hypertension and
Angiology, Medical University of Warsaw, Stefana
Banacha Street 1A, 02-097, Warsaw, Poland.
Email: jakub.strzelczyk@uckwum.pl
Received : Nov 24, 2021
Accepted : Feb 04, 2022
Published : Feb 11, 2022
Archived : www.jcimcr.org
Copyright : © Strzelczyk J (2022).
Keywords: infective endocarditis; vasculitis; cANCA
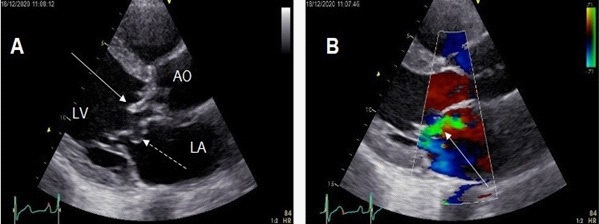
Abbreviations: AO: Aorta; LA: Left Atrium; LV: Left Ventricle; RA: Right Atrium.
Citation: Strzelczyk J, Szmigielski C, Wilimski R, Arendarczyk A, Styczyński G. Infective endocarditis misdiagnosed as cANCA – associated vasculitis. J Clin Images Med Case Rep. 2022; 3(2): 1651.
Description
A previously healthy 37-year-old man was admitted to a nephrology clinic due to the left-sided abdominal pain, petechiae and recurring hematuria. Laboratory tests revealed high levels of C-reactive protein and Antineutrophil Cytoplasmic Antibodies (cANCA). On this basis, vasculitis was suspected and prednisone in high doses was administered. After 30 days of immunosuppressive treatment, due to persistence of symptoms, the patient was referred for an ambulatory echocardiographic study, and because of the abnormal result, he was admitted to our department.
On admission, the patient was clinically in good condition. However, the physical examination revealed a systolic-diastolic heart murmur. Transthoracic echocardiography demonstrated a vegetation attached to the non-coronary aortic leaflet and severe aortic insufficiency. Additionally, an abnormal, perforated, bulging of the anterior mitral leaflet was present, with severe mitral insufficiency (Figure 1). Three blood cultures were positive for Streptoccocus sanguinis. Therefore, the patient was diagnosed with IE according to the modified Duke criteria. Subsequently, the treatment was adjusted to include intravenous antibiotic therapy with vancomycin and ceftriaxone. Afterwards, the patient was qualified for the replacement of the aortic and mitral valves with mechanical valve prostheses. The procedure was uneventful and the patient was discharged home in good condition.
The medical history of this patients is an outstanding example of how complex and misleading the IE diagnosis can be. A selected laboratory test, like cANCA is indeed an important diagnostic marker for vasculitis [1,2]. However, several infectious diseases have been reported to stimulate positive cANCA tests and therefore to mimic vasculitis. One of them is infective endocarditis, which is known to initiate the immune complex disease in about 25% of patients [3,4]. One could speculate that an immunosuppressive treatment, in our patient might have led to a blunted antibacterial response, and potentially to the expansion of the endocardial infection with the bivalvular involvement, while reducing clinical symptoms. Our patient can be a reminder of the clinical rule, that before the definitive diagnosis and treatment of suspected vasculitis, an active infection, especially IE must be excluded [5].
Declarations
Acknowledgments: None
Conflict of interest statement: The authors confirm that they have no conflict of interests.
Funding: The authors received no financial support for the research, authorship or publication of this article.
Ethical approval: Not applicable.
Consent: Informed consent was obtained from the patient.
Guarantor: Grzegorz Styczyński is the guarantor of the content of this manuscript.
References
- Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. 2016; 387: 882-893.
- Bosch X, Guilabert A, Font J. Antineutrophil cytoplasmic antibodies. Lancet. 2006; 368: 404-418.
- Langlois V, Lesourd A, Girszyn N, Ménard JF, Levesque H, Caron F, et al. Antineutrophil Cytoplasmic Antibodies Associated With Infective Endocarditis. Medicine (Baltimore). 2016; 95: e2564.
- Zhou Z, Ye J, Teng J, Liu H, Cheng X, Sun Y, et al. Clinical characteristics of infective endocarditis in patients with antineutrophil cytoplasmic antibody or antiphospholipid antibody: A retrospective study in Shanghai. BMJ Open. 2020; 10: e031512.
- Zarka F, Veillette C, Makhzoum JP. A Review of Primary Vasculitis Mimickers Based on the Chapel Hill Consensus Classification. Int J Rheumatol. 2020; 2020: 8392542.