
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Nd:YAG laser hyaloidotomy for treatment of subhyaloid hemorrhage in pregnancy
Mojtaba Abrishami; Nasser Shoeibi; Hamid Reza Heidarzadeh; Ghodsieh Zamani*
Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author: Ghodsieh Zamani
Eye Research Center, Khatam-al-Anbia Eye Hospital, Qarani Blvd, Mashhad 9195965919, Iran.
Tel: +98-51- 37245363; Fax: +98-51- 37285290
Email: Zamanigh@mums.ac.ir
Received : Dec 16, 2021
Accepted : Feb 07, 2022
Published : Feb 14, 2022
Archived : www.jcimcr.org
Copyright : © Zamani G (2022).
Abstract
Background: To report a pregnant patient with impaired vision due to macular involvement of valsalva retinopathy associated with subhyaloid hemorrhage, who was effectively treated with Nd:YAG laser hyaloidotomy and led to successful visual recovery.
Case presentation: A thirty-year-old pregnant woman at 36- week gestational age was referred due to suddenly decreased visual acuity in her left eye following a severe vomiting. Left eye examination showed a dense large subhyaloid hemorrhage in front of macula extending from superior to inferior arcade with a clear media. With the diagnosis of subhyaloid hemorrhage she underwent Nd:YAG laser hyaloidotomy and visual acuity improved from hand motion to 20/20 after one week.
Conclusion: In this report, Nd:YAG laser hyaloidotomy was shown to be effective and safe in treatment of dense subhyaloid hemorrhage in pregnant patients with Valsalva retinopathy.
Keywords: Nd:YAG laser hyaloidotomy; subhyaloid hemorrhage; pregnancy; valsalva retinopathy.
Abbreviations: rtPA: Recombinant Tissue Plasminogen Activator; BCVA: Best Corrected Visual Acuity; SD-OCT: Spectral Domain Optical Coherence Tomography; NdYAG: NeodymiumDoped Yttrium Aluminium Garnet; mJ: Mill Joule; ILM: Internal Limiting Membrane; ERM: Epiretinal Membrane.
Citation: Abrishami M, Shoeibi N, Heidarzadeh HR, Zamani G. Nd:YAG laser hyaloidotomy for treatment of subhyaloid hemorrhage in pregnancy. J Clin Images Med Case Rep. 2022; 3(2): 1658.
Background
Valsalva retinopathy could be followed by emesis, strong coughing, tenesmus, final stage of labour, crush or compression injuries [1]. Pregnancy is known to be a predisposing factor for valsalva retinopathy [2]. It occurs when a rise in intrathoracic or intraabdominal pressure is transmitted to the venous pressure in the eye causing retinal capillaries rupture [1,2]. Valsalva retinopathy could have various degrees of premacular hemorrhage. Due to a still attached posterior hyaloid membrane, a premacular hemorrhagic patch will be formed that can lead to the formation of Epiretinal Membranes (ERM) and may also damage the photoreceptors from the iron ions or the retinal pigment epithelium [3-5]. Various therapeutic approaches may be used, such as observation, intravitreal administration of SF6 gas or Recombinant Tissue Plasminogen Activator (rtPA), pars plana vitrectomy or Nd:YAG (Neodymium-Doped: Yttrium Aluminium Garnet) laser hyaloidotomy [6-8].
Pregnancy exerts multiple alterations in the mother that may represent risk factors for Valsalva retinopathy such as anatomical, hormonal, metabolic, hematological and immunologica factors. Triggers in pregnant women are defecation, heavy lifting, vomiting and labour [1]. Due to special status of the mother and fetus, available treatment approaches are usually few.
Here we describe a pregnant woman with valsalva retinopathy whom treated successfully with Nd:YAG laser hyaloidotomy
Case presentation
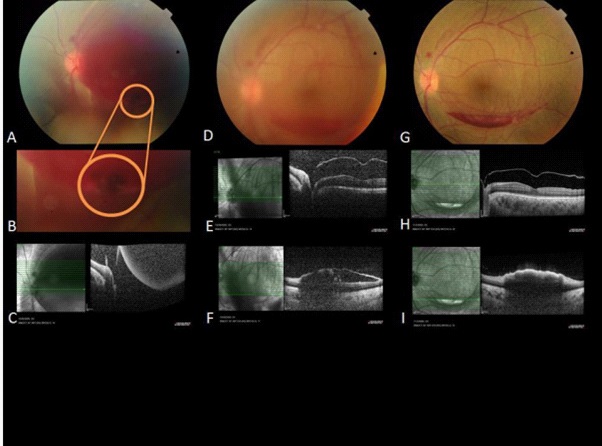
A thirty-year-old pregnant woman at 36-week gestational age referred due to painless, profound and sudden loss of vision in her left eye following a severe vomiting last night. She had no past medical history and took no regular medications. In her ophthalmic examination, her Best Corrected Visual Acuity (BCVA) was 20/20 and hand motion for right and left eyes, respectively. Relative afferent pupillary defect was absent. Anterior segment examination was normal. In her fundus examination, right eye was normal, but left eye showed a dense, large subhyaloid hemorrhage in front of the macula extending from superior to inferior arcade with a clear media. Fundus photograph and Spectral-Domain Optical Coherence Tomography (SD-OCT) performed (Figure C). Her blood pressure, complete blood count and couagulation state were all in normal ranges.
After considering of the therapeutic options and status of the mother and fetus, patient underwent Nd:YAG laser hyaloidotomy. Nd:YAG laser (LIGHTL as YAG, LIGHTMED Corporation, San Clemente, CA) was applied using the Volk Area centralis (Volk Optical Inc., Mentor, OH) lens. The laser settings used were single burst, Q switched mode started with 1.6 Mill Joules (mJ). The laser was employed just above the inferior apex of subhyaloid hemorrhage, near the inferior temporal arcade. In first effort, laser beam hit vitreous and in the second effort with 3.2 mJ energy, a rupture was finally achieved in the posterior hyaloid. Immediately, the blood started to spread slowly into the vitreous body space (Figure A,B). After two days, her BCVA improved to 20/100 and only one third of the subhyaloid hemorrhage remained (Figure D,E,F). One week later, she had 20/20 BCVA for both eyes, and hemorrhage was subtotally drained into the vitreous cavity (Figure G,H,I).
Discussion & conclusion
We represent a pregnant woman with a dense subhyaloid hemorrhage due to valsalva retinopathy following emesis, whose BCVA improved from hand motion to 20/20 with successful Nd:YAG laser hyaloidotomy. This method of treatment was done without any complication [9].
Subhyaloid hemorrhage is defined as bleeding into viteroretinal interface [9,10]. Because of the toxic effects of premacular hemorrhage, an immediate intervention is needed for management of this condition [3-5]. Proper and timely management of these diseases can achieve an excellent visual outcome. The primary treatment modalities include observation, intravitreal injection of antiangiogenic drugs, Nd:YAG hyaloidotomy, intravitreal injection of gas with or without tPA, as monotherapy or combined with surgery. The best option depends on the characteristics of each case [11]. The size, volume and duration of hemorrhage are the most crucial factors for treatment of choice, success rate and complications occurrence [12]. For large subhyaloid hemorrhage or sub Internal Limiting Membrane (ILM) hemorrhage obscuring macula of less than three weeks duration, Nd:YAG (pulsed/ Q switched/ frequency-doubled) krypton laser membranotomy can be used to make an opening in the posterior hyaloid or ILM, so that blood escapes into the vitreous cavity and settles inferiorly [13]. This action clears the visual axis and helps to improve vision. Most studies have used Nd-YAG laser (1064 nm) with a power of 2.2 to 9.7 mJ (cumulative energies of up to 180 mJ), and the central part of the Goldmann 3-mirror lens was used to focus the laser beam [13]. Site of membranotomy must be away from large blood vessels and fovea, at the inferior margin of the hemorrhage and at the site of maximum underlying hemorrhage [13]. During this treatment, the patient must be cooperative, and the surgeon should be sure of sufficient pupil dilation. This reduces the danger of incidental laser complications and the viewing conditions can be improved as well. The laser beam should be directed through the center of the pupil. Thereby, the laser energy can be reduced [14,15]. This treatment option is an inexpensive method that leads a rapid increase in vision. Complications such as full thickness retinal defects, macular hole as well as vitreal, intraretinal or subretinal and choroidal hemorrhages, ERM formation, retinal detachment, and permanent vision loss have rarely been reported [15]. In one article on the use of Nd:YAG laser for subhyaloid hemorrhage, 2 out of 21 patients developed complications. One developed a macular hole (although no macular hole was observed in the other eye with more extended hemorrhage that was treated as well), and the other a retinal break in a myopic eye (with retinal breaks occurring in the untreated eye as well) [16]. Others reported ERM formation with ILM wrinkling after Nd: YAG laser membranotomy in valsalva retinopathy [17]. These complications are associated with the energy of laser used and the level at which the laser beam is targeted [18].
Because spontaneous reabsorption of the hemorrhage may take several weeks to months and during this period permanent visual loss secondary to proliferative vitreoretinopathy may occur, as well as ERM formation and toxic effects of the long standing hemorrhage, we couldn’t observe this patient. We needed special consideration to choose treatment option due to pregnancy. As the paucity of good safety data, we didn’t use intravitreal injection of tissue plasminogen activator. Surgical treatment should also be avoided as much as possible during pregnancy [19]. So, we carried out Nd: YAG laser hyaloidotomy just above the inferior apex of subhyaloid hemorrhage, near the inferior temporal arcade for draining subhyaloid hemorrhage and avoiding photodisruptive effect on macular center. No complication occurred and vision improved rapidly.
In this report Nd: YAG laser hyaloidotomy was shown to be effective and safe in treatment of dense subhyaloid hemorrhage in pregnancy.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials: The datasets used during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: The authors received no funding. It is the authors’ own work, not funded by government or academicals institutes.
Authors’ contributions: All authors (MA, NSh, HRH, GhZ) contributed significantly to this report and agree to be account able for all aspects of the work. MA, NSh, HRH and GhZ read and approved the final manuscript.
Acknowledgements: We thank Research Square that presented the manuscript as preprint with the following link: https://www.researchsquare.com/article/rs-126626/v1 20
Running head: Laser Hyaloidotomy in Subhyaloid Hemorrhage in Pregnancy.
Setting: Khatam-al-Anbia Eye Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
Setting: Khatam-al-Anbia Eye Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
References
- Duane TD. Valsalva hemorrhagic retinopathy. Trans Am Ophthalmol Soc. 1972; 70: 298-313.
- Defrawy H, Sallam A, McKechnie CJ, et al. Valsalva retinopathy in pregnancy. Should we treat? J R Soc Med Sh Rep. 2011; 2: 1–3.
- O’Hanley GP, Canny CL. Diabetic dense premacular hemorrhage. A possible indication for prompt vitrectomy. Ophthalmology. 1985; 92: 507–511.
- Iijima H, Satoh S, Tsukahara S. Nd:YAG laser photodisruption for preretinal hemorrhage due to retinal macroaneurysm. Retina. 1998; 18: 430–434.
- Kroll P, Busse H. Therapy of preretinal macular hemorrhages. Klin Monbl Augenheilkd. 1986; 188: 610–612.
- Brent BD, Gonce M, Diamond JG. Pars plana vitrectomy for complications of retinal arterial macroaneurysms—a case series. Ophthalmic Surg. 1993; 24: 534–536.
- Schmitz K, Kreutzer B, Hitzer S, Behrens-Bauman W. Therapy of subhyaloidal hemorrhage by intravitreal application of rtPA and SF (6) gas. Br J Ophthalmol. 2000; 84: 1324–1325.
- Heydenreich A. Treatment of preretinal haemorrhages by means of photocoagulation (author’s transl). Klin Monbl Augenheilkd. 1973; 163: 671–676
- Shashidhar S, Manasa Penumetcha. ND YAG Posterior Hyaloidotomy: A Safe and Cost-Effective Approach for the Management of Pre-Macular Haemorrhage in Valsalva Retinopathy. Journal of Evidence based Medicine and Healthcare; 2015; 10.18410.
- Spraul CW, Grossniklaus HE. Vitreous hemorrhage. Surv Ophthalmol. 1997; 42: 3– 39.
- Quiroz-Mendoza JL, Valera-Cornejo DA, García-Roa M, RamírezNeria P, Villalpando-Gómez Y, et al. Different approaches in the management of macular hemorrhage: Case reports and a literature review. Medwave. 2020; 20: e7831.
- Dulger SC, Ozdal PC, Teke MY. Valsalva retinopathy: Long-term results and management strategies. Eur J ophthalmol. 2020; 25; 1120672120936175.
- Simakurthy S, Tripathy K. Valsalva retinopathy. Statpearls. 2020.
- Nili-Ahmadabadi M, Lashay AR, Karkhaneh R, Manaviat MR, Amini A, et al. Nd:YAG laser application in premacular subhyaloid hemorrhage. Arch Iranian Med. 2004; 7: 206–209.
- Rennie CA, Newman DK, Snead MP, Flanagan DW. Nd:YAG laser treatment for premacular subhyaloid haemorrhage. Eye (Lond). 2001; 15: 519–524.
- Ulbig MW, Mangouristas G, Rothbacher HH, Hamilton AMP, McHugh JD, et al. Longterm results after drainage of premacular subhyaloid hemorrhage into the vitreous with pulsed Nd:YAG laser. Arch Ophthalmol. 1998; 116: 1465–1469.
- Alvin KH, Timothy YY, Nongnart R. Epiretinal membrane formation with internal limiting membrane wrinkling after Nd:YAG laser membranotomy in Valsalva retinopathy. Am J Ophthalmol. 2003; 136: 763–766.
- Khairallah M, Ladjimi A, Messaoud R, Ben Yahia S, Hmidi K, et al. Retinal venous macroaneurysm associated with premacular hemorrhage. Ophthalmic Surg Lasers. 1999; 30: 226 228.
- Rosenthal JM, Johnson MW. Management of Retinal Diseases in Pregnant Patients. J Ophthalmic Vis Res. 2018; 13: 62–65.