
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Emphysematous cystitis: A rare cause for urosepsis
Milan Gunawardene*; Madura Ambegoda; Munipriya Willaraarachchi; Anuruddha Abeygunasekera
Department of Urology, Colombo South Teaching Hospital, Dehiwala, Sri Lanka.
*Corresponding Author: Milan Gunawardene
Department of Urology, Colombo South Teaching
Hospital, Dehiwala, Sri Lanka.
Email: milangunawardena@yahoo.com
Received : Feb 01, 2022
Accepted : Feb 22, 2022
Published : Mar 01, 2022
Archived : www.jcimcr.org
Copyright : © Gunawardene M (2022).
Keywords: emphysematous cystitis; urosepsis; urinary bladder; intramural air.
Abbreviations: AMH: Austin Moore Hemiarthroplasty; E. coli: Escherichia coli; CT: Computed Tomography; EC: Emphysematous Cystitis; IV: Intravenous.
Citation: Gunawardene M, Ambegoda M, Willaraarachchi M, Abeygunasekera A. Emphysematous cystitis: A rare cause for urosepsis. J Clin Images Med Case Rep. 2022; 3(3): 1701.
Clinical image description
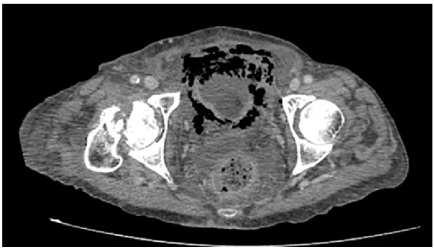
An 89 year old female with diabetes mellitus, dyslipidemia, hypertension and ischemic heart disease admitted to orthopedic department following intra-capsular neck of femur fracture. While awaiting Austin Moore Hemiarthroplasty (AMH), she developed lower abdominal pain, fever, features of acute cystitis, hematuria and pneumaturia. Her urine culture was positive for Escherichia coli (E. coli) and blood culture for gram negative bacilli. Further evaluation with abdominal X-ray (Figure 1) and Computed Tomography (CT) (Figure 2) showed evidence of Emphysematous Cystitis (EC). Her urosepsis was treated with Intravenous (IV) Meropenem 500 mg eight hourly for 14 days. She recovered from sepsis and subsequently underwent AMH.
EC is a rare necrotizing infection of the urinary bladder [1]. Presence of intramural and intraluminal air is pathognomonic for the condition. It is most common in elderly females with multiple comorbidities. Their clinical presentation can vary from asymptomatic to life-threatening severe sepsis. As in this case, E.coli is the main uro-pathogen found in 60-70% of patients [2].
Imaging is essential for the definitive diagnosis as hematological and biochemical investigations are non-diagnostic. Plain abdominal X-ray is highly sensitive (97.4%) and diagnostic in majority (80%) of patients [2]. Intramural air in X-ray delineate the bladder wall giving it the characteristic beaded neck lace configuration (Figure 1). Air-fluid level in X-ray indicates the presence of intraluminal air. Gold standard imaging modality to confirm EC is CT (Figure 2). It helps to determine the severity while differentiating EC from pelvic gas due to other causes [1].
Immediate treatment with extended spectrum IV antibiotics, bladder drainage and tight control of other comorbidities will reduce the mortality in 90% of patients [2]. Others require surgical therapy in the form of partial or total cystectomy [3].

Declarations
Author contribution statement: All authors participated in the treatment of this case, and the first author drafted the manuscript. All authors read and approved the final manuscript.
Conflict of interest: The authors declare no conflicts of interest.
Funding statement: This study has no funding.
References
- Amano M, Shimizu T. Emphysematous Cystitis: A Review of the Literature. Intern Med. 2014; 53: 79-82.
- Rajaian S, Murugavaithianathan P, Krishnamurthy K. Emphysematous cystitis: Diagnosed only if suspected. BMJ Case Rep. 2019; 12: 230715.
- Thomas AA, Lane BR, Thomas AZ, Remer EM, Campbell SC, Shoskes DA. Emphysematous cystitis: A review of 135 cases. BJU Int. 2007; 100: 17-20.