
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Surgical outcome of septorhinoplasty using spreader graft in patients with nasal obstruction: An institutional study
Sabarirajan Ponnusamy1; Himani Lade2; Akriti Sharma3*; Mohammed Shareef PK4; Rohit Bhardwaj5
1 ENT, Consultant, SKS Hospital, Salem, Tamil Nadu, India.
2 ENT, Professor, Department of Otorhinolaryngology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
3 ENT, Assistant Professor, Department of Otorhinolaryngology, SGT Medical College, Hospital & Research Institute, Village Budhera, Gurugram, Haryana 122505, India.
4 ENT, Consultant, Aster MIMS, Kottakal, India.
5 ENT, Assistant Professor, Department of Otorhinolaryngology, Army college of medical sciences and Base Hospital, Delhi cantt-10, India.
*Corresponding Author: Akriti Sharma
Department of ENT, Faculty of Medicine and Health
Sciences, SGT Medical College, Hospital and Research Institute, Gurgaon, Haryana, India
Email: drakriti2709@gmail.com
Received : Jan 18, 2022
Accepted : Feb 23, 2022
Published : Mar 02, 2022
Archived : www.jcimcr.org
Copyright : © Sharma A (2022).
Citation: Ponnusamy S, Lade H, Sharma A, Shareef PKM, Bhardwaj R. Surgical outcome of septorhinoplasty using spreader graft in patients with nasal obstruction: An institutional study. J Clin Images Med Case Rep. 2022; 3(3): 1705.
Introduction
Nasal obstruction is one of the most common complaints of patients in the ENT OPD. The most common causes of nasal obstruction include septal deviation, turbinate hypertrophy, nasal masses and nasal valve narrowing. The nasal valve pathology is often overlooked and attributed wrongly to other factors such as adeviated septum or hypertrophy of turbinates even at the level of tertiary facility [1]. The under addressed problem of internal nasal valve remains a diagnostic and surgical challenge.
Nasal valve which is formed between the upper lateral cartilage and nasal septum is the narrowest part of the upper respiratory tract and thus acts as a primary regulator of airflow dynamics [2]. If the angle of nasal valve happens to be lesser than 10 degrees, it could result in cause significant nasal obstruction in a patient [3]. There are many surgical methods and approaches for addressing this nasal valve pathology [4] and many objective and subjective methods to evaluate the severity of nasal obstruction symptoms.
Numerous studies in literature advocate the use of subjective assessment tools over objective methods, as in their opinion, objective methods do not correlate well with the subjective symptoms of the patients, and the subjective methods are easier to use and cost effective [5,6]. Hence, in our study, we have used the NOSE scale which is a validated subjective scoring method for evaluation of the severity of nasal symptoms. In patients with nasal valve compromise and symptomatic nasal obstruction, the nasal valve angle can be surgically widened using a spreader graft [7,8]. Though other materials, such as nostril stents, flaring sutures and butterfly grafts can also be used for this purpose, spreader graft insertion is preferred for its high success rate [9].
This study was undertaken with the objective of studying the effectiveness of the spreader graft in improving the symptoms of nasal obstruction in patients undergoing septorhinoplasty with open approach.
Materials and methods
This was a prospective, study conducted in the Department of Otorhinolaryngology at Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi during the 18-month period from September 2017 to March 2019.
30 patients in the age group of 18-65 years were included in the study. Only patients with a deviated nasal symptom along with an external nasal deformity, with nasal obstruction being the primary symptom were further screened for the study. A detailed relevant history was taken followed by a thorough general physical and ENT examination in all such patients. A complete examination of nose was done by anterior rhinoscopy and every candidate was examined for the nasal valve compromise using cottle’s maneuver [10]. Patients with positive cottle’s sign were stepped up for a diagnostic nasal endocopy and those with endoscopic evidence of internal nasal valve collapse were shortlisted for the study. The patients finally selected for surgery and the study included those who remained symptomatic after four weeks of medical management.
Patients with chronic rhino sinusitis and sino nasal malignancies were excluded from the study. In addition to these, patients with medical contra indications for surgery, uncontrolled asthma and nasal allergies were also excluded. Institutional ethical committee approval was taken for the study and a detailed consent was obtained from all patients both for surgery and the study.
Facial photographs were taken and NOSE scale scoring was done pre-operatively for each case.
All patients underwent routine investigations including coagulation profile to rule out any contraindication for surgery.
Patients were taken up for surgery under general anaesthesia. Open -external rhinoplasty approach is used with gull wing trans collumellar incision and marginal incisions, exposing the alar and upper lateral cartilages. The cartilage graft was harvested from the septal cartilage leaving adequate dorsal and caudal struts. The upper lateral cartilages were separated from the dorsal septum, spreader grafts were introduced between the dorsal septum and upper lateral cartilage and secured with 5-0 vicryl sutures (Figure 1).
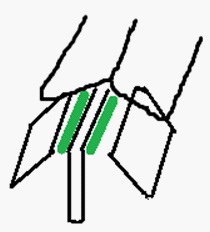
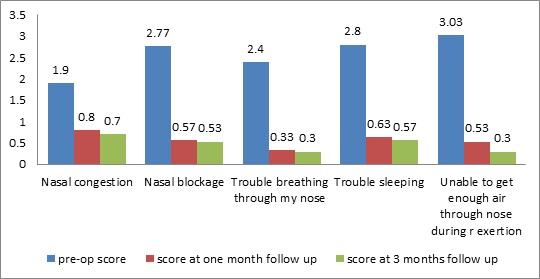
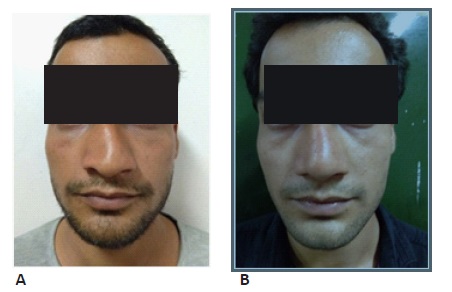
Table 1: depicts the Nasal Obstruction Symptom Evaluation (NOSE) scale. Each symptom is validated over 0 to 4 which is finally multiplied by 5 to give a maximum score of 100.
|
No |
Very mild problem |
Mild to Moderate Problem |
Moderate Problem |
Severe problem |
Nasal |
0 |
1 |
2 |
3 |
4 |
Nasal blockage or obstruction |
0 |
1 |
2 |
3 |
4 |
Trouble breathing through my nose |
0 |
1 |
2 |
3 |
4 |
Trouble sleeping |
0 |
1 |
2 |
3 |
4 |
Unble to get enough air through my nose during exercise or exertion |
0 |
1 |
2 |
3 |
4 |
The skin incisions closed with 5-0 prolene, external splint and dressing applied which were kept in situ for 10 days. After suture removal, patients were discharged with external nasal dressing on second post operative day and were kept in regular follow up.
During surgery, intra operative findings were documented and photographs were taken. The patients were asked to come for follow up visits after one and three months post surgery. The NOSE scale was given to be filled by the patient pre-operatively and on the post-operative visit at 1 and 3 months. The improvement in symptoms were analysed by comparing the post operative photographs, endoscopy and NOSE scale scores with that of the pre operative period. A comparison of pre and post-operative scores was drawn and statistical analysis was done.
The NOSE scale score taken post operatively at one month and three months and were compared with that of preoperative period using Wilcoxon signed rank test (as the data sets were not normally distributed). A ‘P’ value of <0.05 was considered statistically significant. The data was entered in MS EXCEL spreadsheet and analysis was done using Statistical Package for Social Sciences (SPSS) version 21.0.
Results
In this study, we chose patients between the age group of 18-65 of age years. Maximum number of patients in our study (86.6%) were less than 30 years of age, and only 13.4% of patients were between 30-60 years of age. Among 30 subjects, 28 were males and 2 were females.
After obtaining the NOSE score, a grading of all patients was done based on the score. Patients with a pre-operative NOSE score between 30 and 50 were in the moderately severe grade, those with a score between 55-75 were in the severe grade and the ones with a score ranging from 80-100 were in the extremely severe grade.
When we categorized the patients in to moderately severe, severe and extremely severe groups according to the severity of preoperative NOSE scores as suggested in the study by Lipan et al [11], The ‘moderately severe’ group, had a mean three months post operative NOSE score of 7.14 (0 -15 minimum and maximum) with a ‘p’ value of 0.017. The ‘severe’ group, had a mean three months post operative NOSE score of 13.82 (0 -30 minimum and maximum) with a ‘p’ value of 0.0003. The ‘extremely severe’ group, had a mean three months post operative NOSE score of 11.67 (0 -25 minimum and maximum) with a ‘p’ value of 0.027.
We could observe a significant improvement in the NOSE scores in all the groups post operatively, and all the candidates fell in to the ‘mild’ category in the in the post operative period.
Finally, after post-operative values of the NOSE scores were obtained, a comparison was drawn between the pre-operative and post-operative NOSE score values at 1 and 3 months post surgery and data was subjected to statistical analysis.
The mean NOSE score was calculated and was found to be 64.5 preoperatively which reduced to 14.33 and 11.83 post operatively at 1 and 3 months respectively. On analysis, the results were found to be statistically significant (P value <0.001).
In our follow up one patient was found to develop post operative synechae at one month and had to undergo synaechae release.
Discussion
Various studies in literature have proved that Nasal valve collapse contributes significantly to nasal obstruction [1,7]. Numerous objective and subjective methods have been used for its assessment in the past. The NOSE scale, a subjective scoring method validated by Stewart MG et al, is used for assessment of the outcome of Septoplasty [5,12]. Poiseuille’s law states that resistance is inversely proportional to the fourth power of radius and the flow is directly proportional to it. Therefore, a small change in the nasal valve causes a significant impact in the airway resistance and nasal airflow. Also, air flowing through an already narrowed space accelerating to the point of turbulence creating a negative pressure as per Bernoulli principle, leads to dynamic nasal valve collapse. Thus, a collapsed nasal valve is caught in the vicious cycle of cause and effect of nasal obstruction.
Nasal valve repair using spreader graft restores the internal nasal valve to a wider, better anatomy [8] and improves the nasal patency tremendously.
In our study, on comparing the pre-operative NOSE scale scores with the post-operative values noted at 1 month and 3 months post surgery and on analysing the data statistically, we found that the reduction in symptomatic score was found to be statistically significant (P value <0.001) for all five parameters of the NOSE scale including nasal congestion or stuffiness, nasal blockage or obstruction, trouble breathing through my nose, trouble sleeping and unable to get enough air through my nose during exertion or exercise. Among these the difficulty to breathe through nose during exertion was found to be most improved symptom following spreader graft insertion. The improvement in symptoms was noted as early as one month after surgery and remained so on further follow up visits.
Results of our study also revealed that the mean preoperative NOSE score was 64.5 which reduced to 14.33 and 11.83 in the follow up visits after one and three months of surgery respectively. On comparing the values and on analysis the results were found to be statistically significant (p value < 0.001). These findings were similar to the ones in the study conducted by Gerreci et al [13] where the preoperative mean score was found to be 71.4 and the early post operative score was 24.2 at 1- 3 months. Another study of this kind was carried out by Standlee et al [14] who reported a pre operative mean score of 69 and post operative mean of 23.
The duration of follow up was taken as three months in our study considering the practical difficulty in long term follow up including the problem of attrition. In the study conducted by Gerreci et al [13], they found that there was no significant improvement in NOSE scores at 10 months when compared tothe score at three months post-surgery.
Also, in the subgroup analysis done in their study [13], it was seen that the improvement of NOSE score in ‘extremely severe’ subgroup was lesser than the other groups. Hence, counselling of this subgroup candidates preoperatively for the expected results was suggested by them. However, contradictory to this observation we saw significant improvement in the NOSE score of all the subgroups in our study
Hence it was observed that the spreader graft technique used in septorhinoplasty to reconstruct the nasal valve area improved the nasal patency significantly
Limitations of study
The limitation in our study is lack of a control group. But the statistical significance of the effect of intervention, biological plausibility, consistency in the effect of intervention among various subgroups and the association between the spreader graft placement and improvement in nasal patency have been established.
Conclusion
In our study, it was observed that spreader graft insertion done to reconstruct the internal nasal valve in Open Approach Septorhinoplasty, resulted in reduction of post-operative values of all the parameters of the NOSE scale along with the mean NOSE scale score after 1 and 3 months of surgery. The improvement in symptoms started as early as one month and attained a plateau in three month follow up period.
The surgical correction of nasal valve with spreader graft was found to be very effective in improving the nasal patency in improving the symptoms of nasal obstruction, provided the patient selection for the surgery is done well and the procedure executed meticulously
Declarations
Funding: No Funding was received.
Compliance with ethical standards: All the research included in this manuscript meet the ethical guidelines, including adherence to the legal requirements of the study country. The study protocol complied with the 1964 Helsinki declaration and its later amendments. I confirm that the manuscript has not been published or submitted for publication to any other journal.
Conflicts of interest: The authors declare that they have no conflicts of interests.
Informed consent: Informed consent was obtained from all patients included in the study.
References
- Constantian MB, Clardy RB. The relative importance of septal and nasal valvular surgery in correcting airway obstruction in primary and secondary rhinoplasty. Plast Reconstr Surg. 1996; 98: 38-54.
- Apaydin F. Nasal valve surgery. Facial Plastic Surgery. 2011; 27: 179-191.
- Ozturan O, Miman MC, Kizilay A. Bending of the Upper Lateral Cartilages for Nasal Valve Collapse. Archives of Facial Plastic Surgery. 2002; 4: 258-261.
- Cheng PP, Atfeh MS, Khalil SS. Nasal Valve Surgery for Nasal Obstruction: A Systematic Review. The Otorhinolaryngologist. 2014; 7: 80–88.
- Stewart MG, Witsell DL, Smith TL, Weaver EM, Yueh B, et al. Development and validation of the Nasal Obstruction Symptom Evaluation (NOSE) scale. Otolaryngol Head Neck Surg. 2004; 130: 283-290.
- Chisholm E, Jallali N. Rhinoplasty and septorhinoplasty outcome evaluation. Ear Nose Throat J. 2012; 91: E10-E12.
- Sheen JH. Spreader graft: A method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 1984; 73: 230-239.
- Rhee JS, Poetker DM, Smith TL, Bustillo A, Burzynski M, Davis RE. Nasal valve surgery improves disease-specific quality of life. Laryngoscope. 2005; 115: 437-440.
- Sun WH, Wang PC, Hsu SY. Spreader graft to correct nasal valve stenosis with high septal deviation. B-ENT. 2018; 14: 287-293.
- Heinberg CE, Kern EB. The Cottle sign: An aid in the physical diagnosis of nasal airflow disturbances. Rhinology. 1973; 11: 89 -94.
- Lipan MJ, Most SP. Development of a severity classification system for subjective nasal obstruction. JAMA Facial Plast Surg. 2013; 15: 358-361.
- Stewart MG, Smith TL, Weaver EM. Outcomes after nasal septoplasty: Results from the nasal obstruction septoplasty effectiveness (nose) study. Otolaryngol Head Neck Surg. 2004; 130: 283–290.
- Gerecci D, Casanueva FJ, Mace JC, Annen A, Barrett DM, et al. Nasal obstruction symptom evaluation (NOSE) score outcomes after septorhinoplasty. The Laryngoscope. 2019; 129: 841-846.
- Standlee AG, Hohman MH. Evaluating the effect of spreader grafting on nasal obstruction using the NOSE scale. Ann Otol Rhinol Laryngol. 2017; 126: 219–223.