Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Transfemoral tricuspid valve-in-ring implantation: Approach to a challenging clinical scenario
Gabriel Saiydoun1,4*; Sovannarith San2; Jean-Francois Deux3; Madjid Boukantar2; Romain Gallet2; Emmanuel Teiger2,4
1 Department of Cardiac Surgery, Henri Mondor University Hospital, 94010 Créteil, France.
2 Department of Cardiology, Henri Mondor University Hospital, 94010 Créteil, France.
3 Department of Radiology, Henri Mondor University Hospital, 94010 Créteil, France.
4 Paris East Creteil University, School of Health, INSERM, U955, 94010 Créteil, France.
*Corresponding Author: Gabriel Saiydoun
Department of Cardiac Surgery, Henri Mondor University Hospital, APHP, 51 Avenue du Maréchal de
Lattre de Tassigny, 94010 Créteil, France.
Email: gabrielsaiydoun@gmail.com
Received : Mar 24, 2022
Accepted : Apr 21, 2022
Published : Apr 28, 2022
Archived : www.jcimcr.org
Copyright : © Saiydoun G (2022).
Citation: Saiydoun G, San S, Deux JF, Boukantar M, Gallet R, et al. Transfemoral tricuspid valve-in-ring implantation: Approach to a challenging clinical scenario. J Clin Images Med Case Rep. 2022; 3(4): 1812.
Clinical image description
Transcatheter tricuspid valve-in-ring (TVIR) implantation using balloon-expandable valve was an alternative technic to high-risk redo surgery for patients with tricuspid valve (TV) ring repair and symptomatic severe tricuspid regurgitation. In this case, we report a case of unsuccessful transfemoral TVIR implantation with a severe paravalvular leak (PVL) treated successfully with Amplatzer vascular plug.
A 68-year-old woman with rheumatic heart disease was admitted for heart failure symptoms in a context of recurrent symptomatic severe tricuspid regurgitation, due to a defect of coaptation at the level of the pacemaker wire, nine years after a surgical aortic valve replacement (21 mm, mechanic prosthesis, Saint-Jude), mitral valve replacement (25 mm, mechanic prosthesis, Saint-Jude) and tricuspid annuloplasty with a 26 mm Carpentier- Edwards ring (incomplete ring with an oblong C shape, open on the septal annulus, Edwards Lifesciences) that reduces the size of the annulus and improves leaflet coaptation. Transthoracic echocardiography showed severe tricuspid regurgitation associated to a restriction of the septal leaflet movement. After multidisciplinary heart team evaluation, the procedure was performed in the hybrid operating room under general anesthesia with transesophageal echocardiographic guidance. The right common femoral vein approach was used.
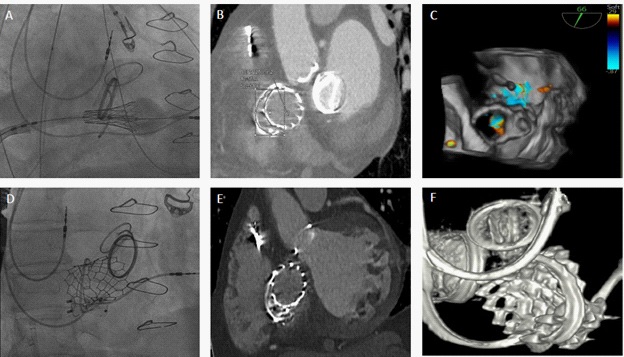
A 26 mm Edward SAPIEN3 (Edwards Lifesciences) valve was approached in an anterograde way and inflated in the tricuspid valve area (Figure 1A). Rapid pacing, via the existing pacing system, was performed to stabilize the heart for the deployment of the valve. We identified a severe PVL in the open medial aspect of the ring after TVIR (Figure 1B and 1C). The open shape and rigidity of this incomplete asymmetrical ring could lead to this imperfect positioning, resulting in severe PVL. Due to the increasing symptoms and persistent leak at the level of the prosthesis, we decided to implant two Amplatzer vascular plug II (St. Jude Medical, Minneapolis, Minnesota) 14 X 5 mm percutaneously (Figure 1D, 1E and 1F). No further leak was identified on echography and the patient was discharged from the hospital after 9 days. This case suggests that this PVL after TVIR can be treated successfully and safely with percutaneous occlusion device which might decrease significantly mortality and morbidity compared to surgical reintervention.
Conflict of interest: On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Sources of funding/Disclosures: On behalf of all authors, the corresponding author states that there are no sources of funding.
Informed Consent Statement: An informed written consent for the publication of the study was obtained.