
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Transcranial color-coded doppler and digital subtraction angiography in the evaluation of middle cerebral artery abnormality in a patient with neurofibromatosis type 1
Ibrahim Acir1*; Maurizio A Leone1; Pietro Di Viesti1;Giovanni Ciccarese2; Vincenzo Strizzi2 ; Michele A Pacilli2; Vincenzo Inchingolo3
1 Neurology Unit, Bakirkoy Dr. Sadi Konuk Training and Research Hospital Istanbul, Turkey.
2 Radiology Unit3, Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Italy
3 Cardiology Unit4 Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Italy.
*Corresponding Author: İbrahim Acır
Başakşehir Çam and Sakura City Hospital Istanbul,
Turkey.
Email: iacir33@gmail.com
Received : Mar 30, 2022
Accepted : May 20, 2022
Published : May 27, 2022
Archived : www.jcimcr.org
Copyright : © Acır I (2022).
Abstract
In patients with neurofibromatosis type 1 (NF1), cerebral vascular abnormalities can manifest in the form of stenosis, occlusions and aneurysms. In case of arterial obstructions, cerebral perfusion is made possible by the compensation mechanisms of collaterals at different levels. Many imaging methods such as Magnetic Resonance Angiography (MR-A), Computed Tomography Angiography (CT-A), Digital Subtraction Angiography (DSA), and Transcranial Doppler or Transcranial Color-Coded Doppler (TCD/TCCD) can be used to detect structural and hemodynamic changes in the cerebral circulation in these patients. We present the case of a NF1 patient with an anomaly of the left middle cerebral artery. The use of vascular imaging methods allowed elucidating the pathogenetic mechanisms of the vascular disease and planning the follow-up.
Keywords: Neurofibromatosis type 1; Transcranial color-coded doppler; Flow-diversion; Case report.
Citation: Acir I, Leone MA, Viesti PD, Ciccarese G, Strizzi V, et al. Transcranial color-coded doppler and digital subtraction angiography in the evaluation of middle cerebral artery abnormality in a patient with neurofibromatosis type 1. J Clin Images Med Case Rep. 2022; 3(5): 1857.
Introduction
Neurofibromatosis type 1 (NF1) is a multisystemic disease involving the skin, peripheral nerves and the central nervous system [1,2]. In the central nervous system, both vascular structures and brain parenchyma can be affected. Cerebrovascular abnormalities can be asymptomatic or symptomatic and can include stenosis/occlusions, aneurysms, or both. In some cases, also extracranial arteries can be involved mainly with stenosis. Transcranial Doppler (TCD) is an ultrasound examination ideal for bedside noninvasive screening of stenosis or occlusions of cerebral vessels. Transcranial color-coded Doppler (TCCD), which combines imaging of parenchyma structures and a pointby-point measurement of velocity in the main intracranial arteries, allows detecting the vascular obstructive pathology and studying collateral circulation more accurately. The so-called “flow diversion”, in particular, is an indirect sign of activation of leptomeningeal collaterals and also a sign of blood flow compensation for stenosis or occlusions. The ultrasound examination revealed that it is characterized by a low-resistance and high-velocity flow pattern in one or more arteries of the circle of Willis on the same side of the obstructive pathology [3-5].
We present the case of a young woman with NF1 who underwent a complete vascular study with TCCD and DSA following a previous diagnosis of “hypoplasia” of the left middle cerebral artery with MR Angiography (MR-A).
Case presentation
We present the case of a 20 years old woman affected by neurofibromatosis with skin cafe-au-lait spots on the skin, one ankle neurofibroma and a history of dyslexia and dysgraphia.
The diagnosis of neurofibromatosis for the patient was confirmed by genetic testing. Later, the genetic test was performed also on the patient’s mother, who resulted to be affected, too. The neurological examination was normal. The flair-Magnetic Resonance Imaging (flair MRI) of the patient’s brain showed point-like gliosis in the subcortical white matter. Vascular imaging was performed firstly with TCCD: with an appropriate axial mesencephalic scan plane through the temporal bone window of both sides in B-Mode, the middle cerebral artery (MCA) in M1 and origin of M2 segments and parenchymal structures were visualised (Figure 1A). With the Microvascularization (MicroV) mode imaging, the vessels of the circle of Willis became visible (Figure 1B). On the left side, with the color-mode, aliasing was detected in the A1 segment of the anterior cerebral artery (ACA) and in the P1 segment of the posterior cerebral artery (PCA), while a low-flow velocity pattern was seen on the M1 segment of MCA (Figure 1C). On the right side, there were normal flow velocity patterns. The MCA M1 segment with lowflow velocity, the ACA A1 segment and the PCA P1 segment with high-flow velocity were confirmed on the left side with Doppler spectrum (Figures 2,3). The peak systolic velocity (PSV) of the ACA A1 on the left side was 30% higher than the contralateral one (Table 1). Subsequently, the patient underwent DSA. After selective catheterism of the left internal carotid artery (ICA), the lack of M1-MCA with local small collaterals from the terminal ICA was seen (Figure 1D). Also, a rich network of leptomeningeal collaterals was detected mainly in the left ACA vascular territory to supply MCA. The remaining cerebral arteries were normal.
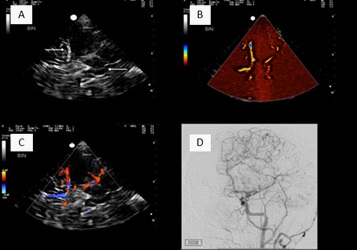
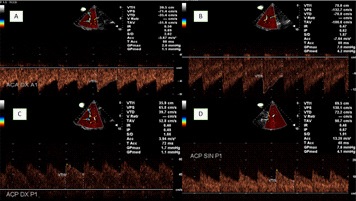
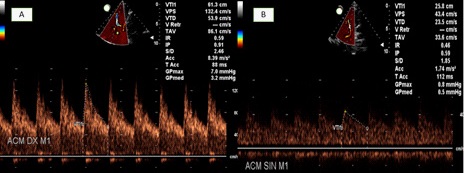
Table 1: Comparison of ACA A1, PCA P1, MCA M1 flow velocities (PSV: Peak Systolic Velocity, EDV: End Diastolic Velocity, IP: Pulsatility Index, R: Right, L: Left)
ACA-A1 |
PCA-P1 |
MCA-M1 |
||||
R |
L |
R |
L |
R |
L |
|
PSV (cm/s) |
71,4 |
132,7 |
66,4 |
136,9 |
132,4 |
43,4 |
EDV (cm/s) |
35,4 |
70,8 |
35,2 |
78,6 |
53,9 |
23,5 |
IP |
0,69 |
0,62 |
0,61 |
0,56 |
0,91 |
0,59 |
Discussion and conclusions
Cerebral ischemia can occur more often in NF1 patients than the general population [6]. In these patients arteries of any size can be affected and multiple stenosis or occlusions can occur in the same patient [7]. Due to their high susceptibility to occlusions, NF1 patients can have a stroke at any age and mostly at an early age. In our patient, after comparing TCCD and DSA images, our diagnostic hypothesis was an occlusion of the left MCA occurred at a very early age followed by progressive activation of collaterals, at various levels, and slow partial recanalization. The process was probably slow considering the presence, as evidenced on DSA, of a dense network of microvessels around the MCA M1 segment, reminiscent of that of the Moya-Moya disease, and the presence of a rich network of leptomeningeal collaterals mainly in the ACA territory. The haemodynamic consequence of activated leptomeningeal collaterals was detected with TCCD as high flow velocity and low resistance pattern in ACA A1 and PCA P1. In this phenomenon, called “flow-diversion” (FD) [3], the blood flow is pushed into the leptomeningeal collaterals because of the arterial obstruction [8,9]. According to an autopsy study, the vessel obstructing pathology in NF1 patients is due to the infiltration of smooth muscle cells in the intima layer [10]. As a consequence, cerebral arteries can be affected by progressive stenosis, and ischemia can occur at any time. In our patient, there were multiple small gliosis in the subcortical white matter in the MCA territory on flair MRI. The patient has always been healthy but had dyslexia and dysgraphia during the early school years, which could be related to the arterial pathology.
Although DSA is considered the “gold standard” for the detection of arterial pathologies, in a diagnostic setting, when the standard procedure requires catheterization not beyond the ICA, this diagnostic method may not display low-flow velocity in MCA because the contrast agent, injected into the ICA, follows the pathway of low-resistance territories. This condition occurred also in our case: the contrast agent behaved like blood flow, then reached mostly the ACA and PCA territories. This limit of DSA can be overcome by using TCCD, which, through multimodal ultrasound imaging, displays both morphology and haemodynamic clearly. One limit of our diagnostic procedure was that we did not perform MR-A with contrast agent before performing DSA and, therefore, we could not compare TCCD and DSA with MR-A. In a similar case it could also be interesting to combine ultrasound imaging and MR imaging with Fusion technology. Since TCCD is well tolerated and repeatable, we aim to use it also for the follow-up of our patient. In conclusion, TCCD is a complementary diagnostic test in the study of vascular brain pathologies and is also a suitable tool for follow-up.
References
- Hirbe AC, Gutmann DH. Neurofibromatosis type 1: a multidisciplinary approach to care. Lancet Neurol. 2014; 13(8): 834-43.
- Dunning-Davies BM, Parker AP. Annual review of children with neurofibromatosis type 1. Arch Dis Child Educ Pract Ed. 2016; 101(2): 102-11.
- Mattle H, Grolimund P, Huber P, Sturzenegger M, Zurbrugg HR. Transcranial Doppler sonographic findings in middle cerebral artery disease. Arch Neurol. 1988; 45: 289-295.
- Zanette EM, Fieschi C, Bozzao L, Roberti C, Toni D, Argentin C, et al. Comparison of cerebral angiography and transcranial Doppler sonography in acute stroke. Stroke. 1989; 20: 899-903.
- Brass LM, Duterte DL, Mohr JP. Anterior cerebral artery velocity changes in disease of the middle cerebral artery stem. Stroke 1989; 20: 1737-1740.
- Terry AR, Jordan JT, Schwamm L, Plotkin SR. Increased risk of cerebrovascular disease among patients with neurofibromatosis type 1: Population-based approach. Stroke. 2016; 47: 60-5.
- Gebarski SS, Gabrielsern TO, Knake J, Latack JT. Posterior circulation intracranial arterial occlusive disease in neurofibromatosis. Am J Neuroradiol. 1983; 4: 1245-6.
- Kucinski T, Koch C, Eckert B, Becker V, Kromer H, Heesen C, et al. Collateral circulation is an independent radiological predictor of outcome after thrombolysis in acute ischemic stroke. Neuroradiology. 2003; 45: 11-18.
- Koss M, Scott RM, Irons MB, Smith ER, Ullrich NJ. Moyamoya syndrome associated with neurofibromatosis Type 1: perioperative and long-term outcome after surgical revascularization. J Neurosurg Pediatr, 2013;11,417-25.
- Okazaki K, Kakita A, Tanaka H, et al. Widespread ischemic brain lesions caused by vasculopathy associated with neurofibromatosis type 1. Neuropathology. 2010; 30(6): 627-633.