
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Adult intussusception: Do we always have a lead point lesion?
Valentina Bianchi; Gilda Pepe*; Federica Marzi; Giuseppe Brisinda
Emergency and Trauma Surgery, Fondazione Policlinico Universitario A. Gemelli IRRCS, 00168 Roma, Italy.
*Corresponding Author : Gilda Pepe
Fondazione Policlinico Universitario A. Gemelli IRRCS, Largo A. Gemelli 8 00168 Roma, Italy.
Ph: +39 0630153225;
Email: gilda.pepepoliclinicogemelli.it
Received : Jun 21, 2022
Accepted : Jul 20, 2022
Published : Jul 27, 2022
Archived : www.jcimcr.org
Copyright : © Pepe G (2022).
Citation: Bianchi V, Pepe G, Marzi F, Brisinda G. Adult intussusception: Do we always have a lead point lesion? J Clin Images Med Case Rep. 2022; 3(7): 1971.
Case report
A 21-year-old woman presented to our hospital Accident & Emergency department (A&E) with a 6-week history of vomiting, abdominal pain, constipation and weight loss (12 kg in 2 months).
She had access to A&E for abdominal pain and vomiting twice in the previous month, but her Blood Tests (BT) were unremarkable and she was discharged home.
On examination, the patient looked sick. Her blood pressure was normal, but she was tachycardic (160 bpm). She had no fever and the abdomen was tender in the right quadrants where a mass was palpable. BT revealed an increase in White Blood Cells (14.3x109/L) and C-Reactive Protein (134 mg/L).
She underwent a CT scan showing a bowel obstruction with a target/doughnut sign involving the distal ileum and ileocecal valve [1,2] (Figure 1). So, indication to an exploratory laparoscopy was given.
We found a consistent thickening of the last two ileal loops with a long ileocecal intussusception which confirmed the radiology report. A conversion to open surgery was necessary. It was impossible to reduce the invagination, manually. Moreover, there were enlarged lymph nodes in the mesentery (lymph node frozen section negative for neoplasia). We decided to proceed with a right hemicolectomy including the last two ileal loops, because of the suspect of a possible neoplasm causing the invagination. A side-to-side mechanical ileotransverse anastomosis was performed, positioning a pelvic and a para-anastomotic drain.
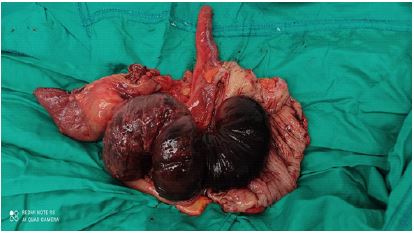
A first macroscopic examination of the surgical specimen revealed an intussusception of about 40 cm of ischemic ileum (Figure 2). The histology confirmed this finding and was negative for neoplasia.
The following hospital stay was uneventful, but for a postoperative ileum that resolved in postoperative day (POD) 5. The patient was discharged home on POD 9.
Intussusception in adults is uncommon and usually due to a lead point lesion [3]. Then, a malignancy has to be suspected especially when associated to symptoms such as chronic pain, palpable mass and weight loss. However, functional conditions are also possible.

Declarations
Author contributions: We all provided care for the patients. VB prepared and wrote the original draft of the manuscript. GP, FM, VB reviewed and edited the article. VB, GB supervised the writing and the production of the paper.
Consent: Written consent for the surgical treatment and future possible publication was obtained from the patient before the operation.
Conflicts of interest: The authors declare that they have no conflicts of interest.
References
- Gorospe EC. Adult intussusception presenting with target sign. Scientific World Journal. 2008; 8: 1154-1155.
- Curcio CM, Feinstein RS, Humphrey RL, Jones B, Siegelman SS. Computed tomography of entero-enteric intussusception. J Comput Assist Tomogr. 1982; 6: 969-974.
- Honjo H, Mike M, Kusanagi H, Kano N. Adult intussusception: A retrospective review. World J Surg. 2015; 39: 134-138.