
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A moderna mRNA-1273 COVID-19 vaccine induced pityriasis rubra pilaris
Lydia Tang-Lin*; Hui Yi Chia; Hazel H Oon
National Skin Centre, Singapore.
*Corresponding Author : Lydia Tang-Lin
National Skin Centre, Singapore.
Email: Lydia_tang@cgh.com.sg
Received : Jul 10, 2022
Accepted : Aug 04, 2022
Published : Aug 11, 2022
Archived : www.jcimcr.org
Copyright : © Tang-Lin L (2022).
Abstract
Pityriasis rubra pilaris (PRP) is a papulosquamous disorder of unknown aetiology. We report the first case of PRP induced by the Moderna mRNA-1273 COVID-19 vaccine.
A 63 year old male presented with a new onset papulosquamous eruption 2 weeks after his second dose of the Moderna COVID-19 vaccine. He underwent a skin biopsy which showed psoriasiform dermatitis but continued to progress despite topical corticosteroid treatment. A clinical diagnosis was made 4 months later when he developed a classic looking confluent orangey-red plaque over the left knee with nutmeg grater-like perifollicular hyperkeratosis. The biopsy confirmed the clinical diagnosis of PRP.
Whilst clinical trials for the COVID-19 vaccines have consistently reported early-onset reactions, reactive dermatosis have become a significant clinical issue for dermatologists. With the push for mass COVID-19 vaccination, it would be important as dermatologists to recognise emerging delayed reactions that may not have been reported in clinical trials.
Keywords: COVID-19 Vaccine; Moderna; mRNA vaccine; Pityriasis Rubra Pilaris
Abbreviations: Moderna vaccine: Moderna mRNA-1273 COVID-19 vaccine; PRP: Pityriasis Rubra Pilaris; CCARD14: aspase recruitment domain family member 14; PAS: Periodic-Acid Schiff; HIV: Human immunodeficiency virus.
Citation: Tang-Lin L, Chia HY, Oon HH. A moderna mRNA-1273 COVID-19 vaccine induced pityriasis rubra pilaris. J Clin Images Med Case Rep. 2022; 3(8): 1994.
Introduction
Pityriasis rubra pilaris (PRP) is a papulosquamous disorder of unknown aetiology. Most cases are acquired, although familial forms have been described to be associated with a gain-of-function mutation in the caspase recruitment domain family member 14 (CARD14) gene [1].
PRP is characterized by hyperkeratotic follicular papules coalescing into orange-red scaly plaques with islands of sparing and palmoplantar keratoderma. It is subdivided into six clinical subtypes according to Griffith’s classification which is based on age of onset, disease extent, prognosis and other associated features [2].
We report a case of PRP following administration of the Moderna mRNA-1273 COVID-19 vaccine.
Case report
A 63-year-old Chinese male, who works as a food vendor, presented to our centre with an itchy scaly rash over the bilateral inner thighs and abdomen. He reported that it had started 2 weeks after the administration of the second dose of the Moderna mRNA-1273 COVID-19 vaccine. He was particularly bothered by the itch that was aggravated by heat and sweat whilst working. He had no significant dermatological issues prior to this presentation. He was otherwise in good health and was not on any regular medications. He was also not on any supplement or traditional Chinese medications. His only significant past medical history was that of childhood asthma.
On initial examination, there were erythematous papules with a fine central scale distributed over the bilateral thighs, abdomen and lower back. He was also noted to have scaly plaques over the bilateral feet dorsum. His nails, palms and soles were unaffected.
A skin biopsy from the right thigh showed parakeratotic mounds with entrapped serous locules and neutrophils, overlying subcorneal collections of neutrophils and eosinophils. The epidermis showed psoriasiform hyperplasia and mild spongiosis with exocytosis of some lymphocytes, neutrophils and eosinophils. There was a superficial perivascular infiltrate of lymphocytes, histiocytes, occasional plasma cells, eosinophils and neutrophils. An overall diagnosis of psoriasiform dermatitis was made and the patient was treated with topical betamethasone valerate 0.1% cream.
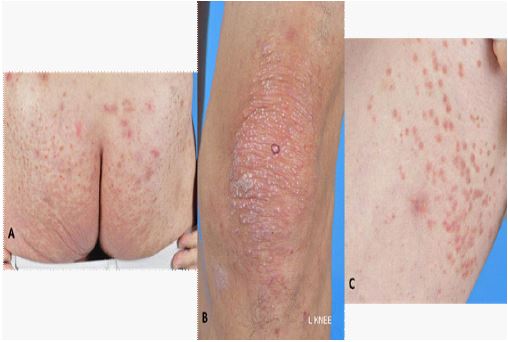
The patient returned 4 months post vaccination with reported progression. On examination, he was noted to have a confluent orangey-red plaque over the left knee with perifollicular hyperkeratosis. Discrete hyperkeratotic follicular papules over the medial thighs and abdomen were seen. Similar scaly papules that became confluent over the buttock area were also seen. His palms and soles were still unaffected (Figure 1).
In view of the clinical presentation, a skin biopsy was repeated to confirm the clinical diagnosis of an evolving pityriasis rubra pilaris.
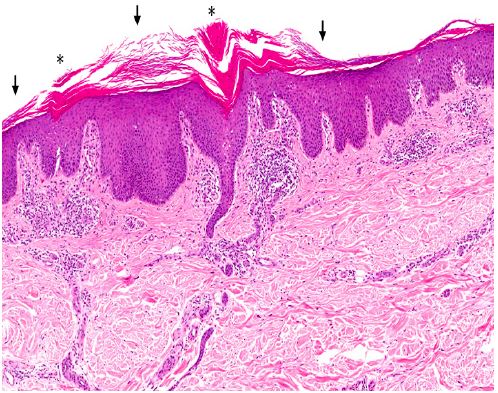
Histology confirmed the presence of alternating orthokeratosis and parakeratosis in a horizontal fashion with focally entrapped serous locules. The epidermis showed psoriasiform hyperplasia with a largely preserved granular layer. There was a superficial perivascular infiltrate of lymphocytes, histiocytes and occasional eosinophils (Figure 2). These features favoured the clinical assessment of an evolving pityriasis rubra pilaris.
The patient decided to continue with topical treatment under close monitoring keeping in view oral retinoids should his condition continue to progress.
Discussion
Whilst clinical trials for the COVID-19 vaccines have consistently reported early-onset reactions, reactive dermatosis to these vaccines have become a significant clinical issue for dermatologists in the past year.
Sun et al. reviewed the literature for reports on cutaneous manifestations to COVID-19 vaccines and found reports on a wide range of reactive dermatosis including morbilliform exanthem, urticaria and pityriasis rosea [3].
Niebel et al. then postulated that cutaneous adverse drug reactions may be divided according to their cytokine profi le, based on the preponderance of specifi c T-cell subsets [4]. Activation of the Th17/Th22 pathway can give rise to psoriasiform and PRP-like dermatosis. Logically speaking, different vaccine types (e.g. mRNA vs viral vector) will activate different toll-like receptors and hence lead to activation of different immune pathways.
We reviewed the literature and found that to date, there have been only 3 reported cases of PRP-like eruptions following COVID-19 vaccinations (Table 1).
Aside from the association with Human Immunodeficiency virus (HIV), no other viral or bacterial infection has been found to be a convincing trigger for PRP. Similarly, multiple drugs have been reported to trigger PRP-like eruptions. However, these too are largely confined to isolated case reports.
Our patient reported the onset of the dermatosis 2 weeks after the COVID-19 vaccination. He had otherwise no change of medications or any other acute illness. The temporal relationship makes the association between the two events highly suspect. The unusual aspect of this case was that contrary to the usual cephalocaudal spread of the lesions, our patient presented with truncal follicular papules extending to the peripheries. The diagnosis of PRP was not considered until he developed a more classic looking lesion over the left knee.
Table 1: The course of endoscopic treatments.
| Author | Vaccine name | Vaccine type | Summary of case | Outcome |
|---|---|---|---|---|
| Liado et al. (August 2021)5 | Oxford-AstraZeneca COVID-19 vaccine ChAdOx1-S n-CoV19 (Vaxzevria, AstraZeneca) |
Viral Vector vaccine | 63 year old Caucasian women developed orange-red waxy plaques over the palms, elbows dorsal aspects of the hands and feet 9 days after the 1st dose of the Vaxzevria vaccine | Skin biopsy was consistent with clinical picture of PRP. She was treated with oral acitretin |
| Hunja et al. (August 2021)6 | Pfizer-BioNTech COVID-19 vaccine | mRNA vaccine | 51 years old male developed a psoriasiform papules 3 days after the 1st dose of the Pfizer-BioNTech COVID-19 vaccine. This worsened a few days after the 2nd dose of the vaccine leading to 60% of his total body surface area affected. | Skin biopsy was consistent with the clinical picture of PRP. He was treated with oral acitretin and topical mometasone furoate 0.1% onitment |
| Sahni et al (August 2021)7 | Coviishield COVID-19 vaccine (ChAdOx1 nCoV-19) | Viral vector Vaccine | 72 year old male developed a papulosquamous eruption on the face, trunk and limbs with Palmoplantar thickening 2 weeks after 1st dose of the Covishield vaccine | Skin biopsy was consistent with the clinical picture of PRP. He was treated with potent topical corticosteroids and emollients. No recurrence was reported after the 2nd does of the COVID-19 vaccine was administered 6 weeks from the first dose. |
In the ongoing evolution of the COVID-19 pandemic, there has been a global push for mass vaccination in a bid to establish herd immunity. It would be important as dermatologists to recognise emerging delayed reactions that may not have been reported in clinical trials. Such knowledge can ensure that patients are accurately investigated and treated appropriately for these reactions. There is still uncertainty as to whether specifi c vaccine types are associated with certain types of cutaneous adverse reactions. We also wonder whether a certain vaccine type may pose a higher risk to a certain subset of patients by triggering its immune pathway.
In view of these clinical questions, it is important to actively report and monitor post-COVID-19 vaccine reactive dermatosis so that we may hopefully find an answer.
The long-term prognosis of our patient is still yet to be determined. Nonetheless, a marriage of what is already known and what is emerging would be the strategy forward in such cases.
Declarations
Funding: This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Patient’s consent: The patient in this manuscript has given written informed consent for the publication of his photographs and case details.
Authorship declaration: All authors had access to data and contributed to the writing and creation of this manuscript.
References
- Vanderhooft SL, Francis JS, Holbrook KA, Dale BA, Fleckman P. Familial pityriasis rubra pilaris. Arch Dermatol. 1995; 131: 448–53.
- Griffiths W. Pityriasis rubra pilaris. Clin Exp Dermatol. 1980; 5: 105-12.
- Sun Q, Fathy R, McMahon DE, Freeman EE. Covid-19 Vaccines and the Skin: The Landscape of Cutaneous Vaccine Reactions Worldwide. Dermatol Clin. 2021; 39(4): 653-673.
- Niebel, D.; Novak, N.; Wilhelmi, J.; Ziob, J.; Wilsmann-Theis, D.; Bieber, T.; Wenzel, J.; Braegelmann, C. Cutaneous Adverse Reactions to COVID-19 Vaccines: Insights from an Immuno-Dermatological Perspective. Vaccines. 2021: 9: 944.
- Lladó I, Butrón B, Sampedro-Ruiz R, Fraga J, de Argila D. Pityriasis rubra pilaris after Vaxzevria® COVID-19 vaccine. J Eur Acad Dermatol Venereol. 2021; 35(12):e833-e835.
- Hunjan MK, Roberts C, Karim S, Hague J. Pityriasis rubra pilaris-like eruption following administration of the BNT163b2 (Pfizer-BioNTech) mRNA COVID-19 vaccine. Clin Exp Dermatol. 2021 Aug 11:10.1111/ced.14878.
- Sahni MK, Roy K, Asati DP, Khurana U. An old entity, a new trigger: Post COVID-19 vaccine pityriasis rubra pilaris. Int J Risk Saf Med. 2021; 32(4): 261-264.