
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Stercoral ulcer perforation mortality: A rare presentation
Syeda Amrah Hasmi1; Manzar Abbas2; Shanza Malik3; Sadaf Khan4*
1Aga Khan University, Karachi, Pakistan.
2Medical College, Aga Khan University, Karachi, Pakistan.
3Dow University of Health Sciences, Karachi, Pakistan.
4Department of Surgery, Aga Khan University, Karachi, Pakistan.
*Corresponding Author : Sadaf Khan
Associate Dean, UGME, Associate Professor, Surgery Director, Centre of Global Surgical Care Medical College, Aga Khan University, Karachi, Pakistan.
Tel: +9221-3486-4751;
Email: sadaf.khan@aku.edu
Received : Aug 26, 2022
Accepted : Sep 15, 2022
Published : Sep 22, 2022
Archived : www.jcimcr.org
Copyright : © Sadaf K (2022).
Abstract
Stercoral ulcers resulting from damage to the intestinal lining due to chronic constipation are rarely presented as perforations. The incidence of these perforations is 3.2% of all colonic perforations. Poor diet, anatomic factors, and certain medications increase the risk of perforations. The presentation of stercoral ulcers varies widely among patients. Immediate surgical intervention is required for these patients because of the increased risk of mortality due to severe intraperitoneal contamination. To the best of our knowledge, we report the first case from our region of patient mortality due to stercoral ulcer perforation.
Keywords: Stercoral ulcer; Rare mortality.
Citation: Hasmi SA, Abbas M, Malik S, Khan S, et al. Stercoral ulcer perforation mortality: A rare presentation. J Clin Images Med Case Rep. 2022; 3(9): 2068.
Background
Stercoral ulcers are a rare clinical entity. While the exact incidence of stercoral ulcers is unknown, the estimated postmortem stercoral ulcer incidence is reported to range from 0.04 to 2.3% [1]. Resulting of chronic constipation, these ulcerations of the intestinal tract occur with hard impacted stool damaging the intestinal lining [2]. Significant histologic and clinical variations in the presentation have been noted with this pathology. Ulcers of varying shapes and sizes, hyperemic mucosa, and broad-based polypoid lesions are some of the macroscopic features identified [3]. These ulcers are diagnosed histologically as tissue with a relatively mild degree of inflammation, with a lack of obvious crypt architectural abnormalities [4]. Clinically, they present with nonspecific symptoms such as fever, abdominal pain, and distension [5].
The incidence of stercoral perforation is 3.2% of all colonic perforations in the general population [6]. Multiple metabolic and neurogenic syndromes, poor diet, anatomic factors, and certain medications (such as narcotics, anticholinergics, and antacids) are noted to increase the risk of perforation [6]. There are many wide systemic complications that occur with perforation, of which, peritonitis is the most severe [7]. There is a high risk of morbidity and mortality (34-57%) due to severe intraperitoneal contamination caused by feces. Therefore, immediate surgical intervention as well as monitoring of possible complications is vital to optimizing the patient’s survival [8].
Here we report the case of a patient diagnosed with an intestinal stercoral ulcer. To the best of our knowledge, it is the first case of patient mortality by this disease in Pakistan.
Case presentation
An 86-year-old female, functional class III, presented to the emergency room with complaints of upper abdominal pain and abdominal distension for 8 hours. The pain was sudden in onset, increasing in severity, constant, throbbing in character, and non-radiating. It was temporarily relieved with NSAIDs and surface massage. The patient felt bloated but denied fever, nausea, or vomiting. She had a history of chronic constipation but reported a bowel movement a few hours prior to the presentation. There was no history of melena, hematochezia, ortenesmus. There were no urinary complaints and the patient’s appetite, and sleep was normal. Her weight was stable.
The patient underwent a colonoscopy 7 years prior to presentation to investigate her chronic constipation and post-prandial right lower quadrant pain. The examination was normal. She had also undergone a cystoscopy for recurrent urethral and left inguinal pain and dysuria. Her past medical history included a diagnosis of osteoarthritis, osteoporosis, and peripheral neuropathy for 10 years, for which she was prescribed NSAIDs, vitamin and calcium supplements, and Gabapentin 300 mg once a day. She was postmenopausal and did not have a history of substance abuse or any known allergies. Her family history was unremarkable for any significant pathology.
Investigations
On examination, the patient was tachycardic, with a pulse of 120 bpm. Her respiratory rate and blood pressures were 18/ min and 122/86 mmHg respectively. She was afebrile and maintained 99% oxygen saturation on room air. She did not have pallor, jaundice, edema, or lymphadenopathy. She had abdominal tenderness in the epigastric region with distention and generalized guarding. Gut sounds were audible, while DRE showed hard impacted stool within a normal rectum. There were no signs of visceromegaly, visible pulsations, or peristalsis. Her central nervous system was grossly intact, and her chest examination was unremarkable. Baseline investigations in the ER were completed (Table 1).
Table 1: Baseline Investigations in the ER.
| Hemoglobin | 13.6 g/dL |
| Hematocrit | 42.8% |
| White Blood Cells | 2.8 (×109 /L) |
| Platelet count | 160 (×109 /L) |
| PT/INR | 12.4 sec/1.2 |
| APTT | 25.3 sec |
| Procalcitonin | 3.92 ng/mL |
| Alkaline Phosphatase | 147 IU/L |
| Fasting Blood Glucose | 191 mg/dL |
| Creatinine | 0.9 mg/dL |
| BUN | 15 mg/dL |
| Sodium | 140 mmol/L |
| Potassium | 4.2 mmol/L |
Treatment
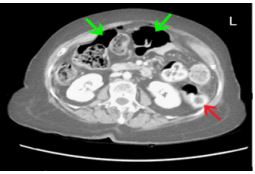
The patient was resuscitated with Ringers Lactate. A CT scan (Figure 1) was obtained. Numerous specks of air were identified in the peritoneal cavity, consistent with pneumoperitoneum. Perforation at the site of a mid-jejunal loop was considered because of a large loculus of air at the site. Significant large bowel fecal loading with minimal thickening of descending colon was also present. Based on the history and workup, she was diagdiagnosed as having peritonitis secondary to bowel perforation. Her family was counselled regarding the risks and benefits of surgical treatment and upon their request, she was planned for an emergency exploratory laparotomy, with possible bowel resection with anastomosis or stoma formation.
On entering the abdominal cavity, minimal free air was encountered. On exploration, the pelvis was full of small hard pellets of stool. Despite initial assessment suspecting a perforation at the level of jejunum, a 2 cm stercoral perforation was identified at the rectosigmoid junction. The colon was full of pellets of stool but was not distended and the wall appeared normal. A Hartmann’s procedure was performed with an end-stoma at the level of the mid-sigmoid colon.
Histopathologic evaluation of the resected colon at the site of the perforation (Figure 2) revealed eroded and ulcerated mucosa, consistent with the diagnosis of stercoral ulcer. Moderate transmural inflammation was seen with congested and dilated blood vessels. The muscularis propria was thinned out at the perforation site. There was dense inflammation with fecal material impacted in the colonic wall along with bacterial colonies. There was no evidence of malignancy or granuloma formation.
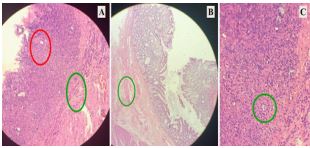
A – Dense inflammation along the serosal aspect (red outline). Thinned out muscularis propria showing perforation (green outline).
B – Congested blood vessel with edema.
C – Impacted fecal material.
Outcome and follow-up
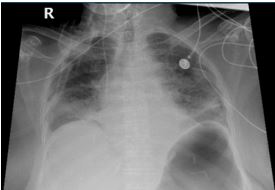
Post-operatively, the patient was extubated and was monitored in a high-dependency unit. A CVP line was inserted. On post-operative day 2, she had increasing hypoxia, requiring 5 lit oxygen to maintain adequate saturations. Bi Paptherapy was initiated in addition to Beclomethasone nebulization. Chest Xray (Figure 3) showed evidence of interstitial pulmonary edema, for which 20 mg of Furosemide twice daily was added to her regimen and she was kept in a negative balance. Tracheal culture indicated hospital-acquired pneumonia due to MDR Acinetobacter. Treatment with Meropenem 1 gram every 8 hours and Vancomycin 1 gram every 12 hours was initiated. She was hypotensive, tachycardiac, and maintaining a low urine outputso was managed as septic shock secondary to peritonitis and HAP. During this time, the patient was drowsy but arousable. Supportive treatment with beta-blockers and fluids was maintained.
On post-operative day 3, her oxygen requirement increased to 10 L. BiPap support was increased. Nebulization with ipratropium was added. Hypoxic respiratory failure due to fluid overload vs hospital-acquired pneumonia was considered. There was a sudden alteration in mental status with GCS 7-9/15. Metabolic encephalopathy or encephalopathy secondary to sepsis was suspected. Her ECG showed new-onset atrial fibrillation with a rapid ventricular response. IV amiodarone infusion was started. The patient’s family was counselled regarding her poor prognosis and a decision not to resuscitate was made in consultation with the family. On the post-operative day 4, she continued to deteriorate and developed spontaneous cardiac arrest. After running the hospital protocol, death was declared.
Discussion
We report the first case from our region of patient mortality due to stercoral ulcer perforation. Stercoral colonic perforation, initially described by Berry in 1894 [9], poses a fatal consequence of chronic constipation with less than 150 cases reported until 2018 [10]. A single case of stercoral ulcer perforation has been reported previously in our country with good patient recovery [2]. However, this may be in part due to the paucity of reporting.
Table 2: Baseline investigations on post operative days 2-3.
| Post operative day 2 | |
| Hemoglobin | 9.7 g/dL |
| White Blood Cells | 6.3 (×109> /L) |
| Procalcitonin | >100 ng/mL |
| Post operative day 3 | |
| Arterial Blood Gas Test | 7.26/47.2 mmHg/125 mmHg/20.6 mEq/L/98% |
| Platelet count | 108 (×109 /L) |
| BUN | 31 mg/dl |
| Creatinine | 1.3 mg/dl |
| Sodium | 141 mmol/L |
| Potassium | 2.7 mmol/L |
| Calcium | 6.7 mg/dL |
| Magnesium | 1.3 mg/dL |
| PT/INR | 20.8 sec/2.1 |
| CRP | 123.93 mg/L |
A particular predisposing factor is a long standing use of Non-Steroidal Anti-Inflammatory Agents (NSAIDs) that were prescribed for our patient for the management of osteoarthritis. NSAIDs have been implicated in the development of constipation in recent studies and are notorious for inducing mucosal lesions throughout the GI tract [12]. This potential association is supported by a case addressed by Patel VG et al. [13] where a 45-year-old woman with significant comorbidities and regular use of NSAIDs was found to have a stercoral perforation of the bowel. Our case supports the possibility that NSAIDs may increase the risk of this dangerous sequela of constipation and must be advised with caution in individuals at risk.
As with most GI disorders, the signs and symptoms of stercoral ulceration are non-specific, such as generalized abdominal pain, discomfort, vomiting, fever, and abdominal distension. It mimics several intra-abdominal pathologies (neoplastic, diverticular, infectious, or traumatic) which are all more common conditions in the elderly [14,15]. However, the diagnosis of this entity should never be preemptively ruled out because while rare, the mortality of patients with stercoral perforation is considerably higher than that of colon perforation by other causes [16]. This is due to a larger size of perforation, more extensive contamination of the abdominal cavity with feces, and older patients with poor general performance status. Delay in diagnosis can lead to catastrophic complications of perforation and septic shock [17]. A study assessing multiple patient outcomes on the 7th post-operative day reported a higher incidence of mortality in patients with a 2-day delay in surgical treatment [18]. Computed Tomography is a sensitive diagnostic tool. In one study, the most sensitive CT findings in decreasing order were pericolonic stranding (80%), perfusion defects (70%), dense mucosa (62%), thickening of the colon wall (60%), abnormal gas (50%) and pericolonic abscess (20%) [19]. In our case, pneumoperitoneum was identified, while pericolonic fat stranding which has been noted as the most helpful imaging observation was not seen. This indicates variability between findings and should be further studied as a tool for pre-operative diagnosis [20].
Histopathologic evaluation of the resected colon showed that the muscularis propria was thinned out which predisposed to colonic wall perforation. This was also described by Facy O et al. in his case report [21]. The recommended intervention with lower mortality is a Hartmann procedure with drainage of the abdominal cavity [22]. A segmental resection with a primary anastomosis and proximal colostomy could be performed but is associated with worse outcomes [23]. Despite appropriate therapy, our patient had a complicated post-operative course, eventually leading to mortality. Among other causes of deterioration was the hospital acquired pneumonia. A possible contributor could also be the routine use of pregabalin, a neuroleptic medication, which has been described as a risk factor for post-operative pneumonia [24].
Stercoral perforation is not purely a surgical condition as it is often complicated by medical illnesses which impact prognosis. A multidisciplinary approach should be under taken with an inter professional group of physicians, gastroenterologists, surgeons, pharmacists, and radiologists involved. We suggest that a favorable outcome in stercoral perforation depends on early diagnosis, thorough resection of ulcerated tissue and fecaloma, aggressive therapy of any underlying sepsis, and most importantly the surgical team’s holistic assessment of the patient pre and post-operation. We hope that prompt employment of these measures will enhance clinical outcomes and improve survival, preventing mortality.
Conclusion
Our case report suggests that while stercoral ulcer is a rare pathology, it has significant complications with perforation being the most important cause of mortality. Therefore, it is imperative to have a greater understanding of this disease and of patient-specific predisposing factors. This is essential to not only to monitor patients at risk to have stercoral ulcerprevention but to also have timely detection and intervention for better patient outcomes.
References
- Gan S, YK Liew, SJAM Pothiawala. A case of colonic obstruction combined with ischemic colitis. 2021; 4: 58-60.
- Yasin MMA, et al. Stercolith Perforation. 2012; 22: 455-457.
- Forootan M, et al. Biofeedback efficacy to improve clinical symptoms and endoscopic signs of solitary rectal ulcer syndrome. 2018; 28.
- Tanaka M, et al. Simple mucosal biopsy criteria differentiating among Crohn disease, ulcerative colitis, and other forms of colitis: Measurement of validity. 2000; 35: 281-286.
- Marget M, HJCR Ammar. Not your usual constipation: Stercoral perforation. 2017; 2017: bcr2016218283.
- Brown CD, et al. Stercoral perforation of the colon in a heroin addict. 2017; 2017: bcr-2016-218875.
- Serpell J, RJJoBS Nicholls, Stercoral perforation of the colon. 1990; 77: 1325-1329.
- Ryu CG, et al. Clinical analysis of stercoral perforation without mortality. 2017; 34: 253-259.
- Berry JJBMJ. Dilation and rupture of the sigmoid flexure. 1894; 1: 301.
- Poitras R, SJIjoscr Oyogoa. Opioid drugs and stercoral perforation of the colon: Case report and review of literature. 2018; 42: 94-97.
- Morano C, TJS Sharman. Stercoral Colitis. 2021.
- Philpott H, et al. Republished: Drug-induced gastrointestinal disorders. 2014; 90: 411-419.
- Patel VG, et al. Stercoral perforation of the Sigmoid colon: Report of a rare case and its possible association with nonsteroidal anti-inflammatory drugs/Discussion. 2002. 68: 62.
- Huang WS. et al. Management of patients with stercoral perforation of the sigmoid colon: Report of five cases. 2006; 12: 500.
- Tsung Chih T, C Chien Ming, Stercoral colitis. Resuscitation & Intensive Care Med. 2017; 4: 231-232.
- Nam JK, et al. Clinical analysis of stercoral perforation of the colon. 2010; 55: 46-51.
- Hsiao TF, YHJTAjoem. Chou, Stercoral perforation of colon: A rare but important mimicker of acute appendicitis. 2010; 28: 112. e1-112. e2.
- Rozenblit A, et al. Stercoral perforation of the sigmoid colon: Computed tomography findings. 2000; 55: 727-729.
- Wu CH, et al. Necrotic stercoral colitis: importance of computed tomography findings. 2011; 17: 379.
- Maurer CA, et al. Use of accurate diagnostic criteria may increase incidence of stercoral perforation of the colon. 2000; 43: 991-998.
- Facy O, et al. [Stercoral perforation of the colon. Physiopathology and treatment strategy]. Gastroenterol Clin Biol. 2007; 31: 1069-1070.
- Gekas P, MMJG Schuster. Stercoral perforation of the colon: Case report and review of the literature. 1981; 80: 1054-1058.
- Chakravartty S, A Chang, JJCd. Nunoo, Mensah. A systematic review of stercoral perforation. 2013; 15: 930-935.
- Holubar SD, et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on prevention of postoperative infection within an enhanced recovery pathway for elective colorectal surgery. 2017; 6: 1-18.