
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Multidisciplinary management of nasal
dermoid with intracranial extension
Kristen Briney1; Catrina Estrella2; Shaan Mody3; Evelyne Kalyoussef4; Esther A Nimchinsky5; Catherine A Mazzola6*
1Cornell University, USA.
2College of Mount Saint Vincent, USA.
3Rutgers University, USA.
4Department of Otolaryngology, Rutgers New Jersey Medical School, USA.
5Department of Neuroradiology, Rutgers New Jersey Medical School, USA.
6New Jersey Pediatric Neuroscience Institute, USA.
*Corresponding Author : Catherine A Mazzola
New Jersey Pediatric Neuroscience Institute, 131 Madison Ave 3rd Floor, Morristown, NJ 07960, USA. Tel: (973) 326-9000, Fax: (973) 326-9001;
Email: cmazzola@njpni.com
Received : Aug 22, 2022
Accepted : Sep 23, 2022
Published : Sep 30, 2022
Archived : www.jcimcr.org
Copyright : © Mazzola CA (2022).
Abstract
Nasal dermoids are rare congenital lesions present in 1/20,000 to 1/40,000 patients. Only about 10% of these congenital lesions have an associated tract or tail with an intracranial extension. The intracranial component of the mass predisposes the child to risks of meningitis and abscess formation. We aim to discuss the etiology of dermoid cysts as well as neurosurgical approaches for the management of cases with intracranial extension, which include both endoscopic and open surgical approaches. We present an 18-month-old boy who underwent a bifrontal craniotomy and resection of his nasal dermoid with intracranial extension. This case report and review of the literature exemplify the collaboration between pediatric otorhinolaryngologists and neurosurgeons to successfully remove nasal dermoids specifically presenting with intracranial extensions.
Keywords: Intracranial extension; Midline facial mass; Nasal dermoid cyst.
Abbreviations: CT: Computed Tomography; ENT: Ear, Nose, and Throat; MRI: Magnetic Resonance Imaging.
Citation: Briney K, Estrella C, Mody S, Kalyoussef E, Mazzola CA, et al. Multidisciplinary management of nasal dermoid with intracranial extension. J Clin Images Med Case Rep. 2022; 3(9): 2080.
Background
Nasal dermoids are slow-growing, benign lesions that represent approximately 60% of midline nasal masses in infants and children [1]. These growths are composed of mesodermal and ectodermal components lined by squamous epithelium and typically occur in isolation within the subcutaneous tissue [2]. They present with an equal gender distribution and are generally diagnosed by 3 years of age [3]. Dermoid cysts can appear anywhere on the skin with only 3% appearing along the nasal midline [4]. Nasal dermoids may lead to facial deformities, jeopardize the child’s airway, or obstruct the visual field and impact the development of sight. Cysts with an intracranial extension carry the risk of serious complications such as meningitis or brain abscess formation with rupture or fluid leakage, so timely surgical excision is imperative [3]. Removal of any connecting stalk is necessary to prevent cerebrospinal fluid leaks and reduce chances of recurrence [5]. Luckily, complications only occur in approximately 1.2% of nasal dermoid cases [6].
Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) may both be performed to diagnose and plan for the treatment of nasal dermoids [5]. The primary treatment modality is surgical resection, which is curative in most cases. Reportedly, the recurrence rate is between 5-12% after total resection [7]. Pediatric Otorhinolaryngologist (ENT) surgeons, neurosurgeons, and occasionally plastic surgeons may collaborate to achieve complete excision of the lesion as well as to leave the child with minimal residual scarring. The purpose of this case study is to present an 18-month-old boy who underwent a bifrontal craniotomy and resection of his nasal dermoid with intracranial extension, exemplifying the necessary collaboration of ENT surgeons and neurosurgeons to successfully remove intracranial nasal dermoids.
Case presentation
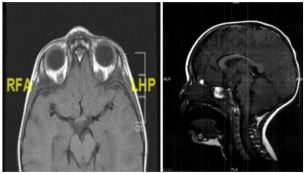
An 18-month-old baby boy presented with a nasal dermoid cyst extending into his anterior skull base. The patient was born full-term and met all developmental milestones. His parents reported no family history of nasal or neck masses. At birth, the infant presented with a small pit along the mid dorsum of his nose (Figure 1). The cystic extranasal lesion began to swell at around 14 months old without drainage or rupture, prompting referral to pediatric otorhinolaryngology at 18 months old. Facial MRI showed an extranasal mass measuring 0.9 cm x 0.8 cm x 0.6 cm and an additional intracranial lesion at the foramen cecum located anterior to the crista galli, measuring 0.8 cm x 0.4 cm x 0.7 cm. No fluid-filled tract was noted to extend from the extracranial to the intracranial compartment at this point in time (Figure 2). Surgical removal of both cysts was recommended to avoid the risk of rupture and meningitis.
After informed consent was obtained, the patient underwent a two part surgery to address both portions of the nasal dermoid. First, the ENT surgeon resected the intranasal component of the mass through a direct vertical incision. The intranasal cyst was intraoperatively confirmed to have a tail extending into the anterior skull base area.

After surgical completion by the otorhinolaryngologist, the neurosurgeon performed a bifrontal craniotomy to resect the anterior skull base portion of the dermoid cyst. No hair was shaved in the process. The anterior scalp flap was pulled away to expose the frontal bones of the skull and the dura was opened. The dermoid was carefully resected, revealing a stalk going through the anterior cribriform plate. The rootlets of the stalk were transected with microscissors. The surgical pathology examination concluded that both the midline nasal dorsal mass and the anterior skull base tumor were consistent with dermoid cysts based on microscopic examination. Post-operatively, the patient was left with extremely minimal residual scarring on the scalp. The incision on the nose and scalp was well-healed.
Discussion and Conclusion
Differential diagnosis for midline congenital nasal masses includes nasal dermoids as well as nasal gliomas, encephaloceles, teratomas, lipomas, vascular anomalies, neurofibromas, and epidermoid cysts [2]. Detection of intracranial extensions is of utmost importance to avoid complications that could result in irreversible brain damage, which demonstrates why excision of nasal dermoids serves more than just an aesthetic purpose.
While planning a surgical approach, MRI is considered better for visualizing the soft tissue while CT is considered the best option to visualize bony deformities including defects of the cribriform plate [2]. In terms of predictive value in diagnosing intracranial extensions, MRI produces less false positives, which reduces the chance of an unnecessary intracranial surgical approach [8]. In our patient, MRI detected the intracranial portion of the nasal dermoid which was sufficient for surgical planning, though the fine tract connecting the nasal and intracranial areas was not clearly visualized. Considering the high dosage of radiation that comes with CT scans, using MRI alone as a diagnostic tool is suitable for cases with intracranial extension [8].
Prenatal imaging may allow for detection of midline facial masses as a fetus, which can help with early counseling for couples on pre and postnatal management [9]. Three dimensional reconstruction of ultrasound images can provide obstetricians and radiologists with early visualization of the face in order to diagnose masses such as nasal dermoids and obtain referral for neurosurgical consultation [7].
In terms of the optimal age for undergoing surgical removal of nasal dermoids, most authors advocate that the soonest possible treatment is best. As these lesions gradually increase in size, they can compress the nasal bones making for a more complex repair [5]. Successful excision has been achieved in children as young as 77 days old, indicating that age should not be a restricting factor in surgical treatment [7]. In situations where the lesion is showing no signs of rapid growth and the child is neurologically intact without complications, the family may elect to monitor the child and postpone surgical intervention.
Depending on the placement of the nasal dermoid, surgical approaches can include direct excision, open rhinoplasty, nasal endoscopy, and craniotomy. For cases with intracranial extension, the traditional approach includes a bifrontal or small window craniotomy in order to properly visualize the lesion. However, a large incision provides risks of potential blood transfusion and unfavorable scarring. Transnasal endoscopic approaches are emerging as a minimally invasive alternative to replace craniotomy as long as the anatomy is favourable [10].
Midline exposure and nasal bone osteotomy is also being pioneered as a surgical alternative to coronal incision [1]. Our patient underwent a traditional approach via a bicoronal incision and had no complications. Early intervention and multidisciplinary management of nasal dermoids with intracranial extension can contribute to the achievement of successful excision and aesthetic results.
Declarations
Conflict of interest statement: The authors declare that the article content was composed in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgment: The author thanks the New Jersey Pediatric Neuroscience Institute for supporting and supplying clinical information.
References
- Purnell C, Skladman R, Alden TD, Corcoran JF, Rastatter JC, et al. Nasal Dermoid Cysts with Intracranial Extension: Avoiding Coronal Incision through Midline Exposure and Nasal Bone Osteotomy. Journal of Neurosurgery: Pediatrics. 2020; 25: 298–304. https://doi.org/10.3171/2019.9.peds19132.
- Kotowski M, Adamczyk P and Szydlowski J. Nasal Dermoids in Children: Factors Influencing the Distant Result. Indian J Otolaryngol Head Neck Surg. 2021. https://doi.org/10.1007/s12070-021-02568-y
- Opsomer D, Allaeys T, Alderweireldt A, Baert E, Roche N, et al. Intracranial complications of midline nasal dermoid cysts. Acta chirurgica Belgica. 2019; 119: 125–128. https://doi.org/10.1080/00015458.2017.1411552
- Tatar EC, Selçuk OT, Saylam G, Ozdek A, Korkmaz H, et al. The management of rare nasal mass-nasal dermoid sinus cysts: open rhinoplasty. Rare tumors. 2009; 1: e40. https://doi.org/10.4081/rt.2009.e40
- Ni K, Li X, Zhao L, Wu J, Liu X, Shi H, et al. Diagnosis and Treatment of Congenital Nasal Dermoid and Sinus Cysts in 11 Infants. Medicine. 2020; 99. https://doi.org/10.1097/md.0000000000019435
- Kalmar CL, Patel VA, Taylor JA. Analysis of National Outcomes for Simple Versus Complex Nasal Dermoid Cyst Excision. The Journal of craniofacial surgery. 2021; 32: e281–e283. https://doi.org/10.1097/SCS.0000000000007160
- Ajose Popoola O, Harrison LW, Silvera M, Teot LA , Madsen J, Rahbar R, et al. “Nasal Glioma: Prenatal Diagnosis and Multidisciplinary Surgical Approach.” Skull Base Reports. 2011; 1: 083–088., https://doi.org/10.1055/s-0031-1284210
- Bloom DC, Carvalho DS, Dory C, Brewster DF, Wickersham JK, Kearns DB, et al. Imaging and surgical approach of nasal dermoids. International Journal of Pediatric Otorhinolaryngology. 2002; 62: 111–122. https://doi.org/10.1016/S0165-5876(01)00590-0
- Tonni, Gabriele, et al. Prenatal Ultrasound and Histological Diagnosis of Fetal Nasal Glioma (Heterotopic Central Nervous System Tissue): Report of a New Case and Review of the Literature. Archives of Gynecology and Obstetrics. 2011; 283: 55–59. https://doi.org/10.1007/s00404-011-1856-3.
- Seidel DU and Sesterhenn AM. Intracranial Nasal Dermoid Sinus Cyst: Transnasal Endoscopic Resection by Open Rhinoplasty Approach, With Intraoperative Video. The Journal of craniofacial surgery. 2016; 27: 2110–2112. https://doi.org/10.1097/SCS.0000000000003107