
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Incidence of surgery after gamma knife radiosurgery for
parasagittaland parafalcine meningiomas is higher than
meningiomas in other locations: A 10-year institutional
analysis and review of the literature
Andrew J Montoure1; Akram M Eraky1; Eduardo Martinez del Campo1; Joseph Bovi2; Jennifer Connelly3; Nathan T Zwagerman1*
1Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, Wisconsin, USA.
2Department of Radiation Oncology, Medical College of Wisconsin, Wisconsin, USA.
3Department of Translational Brain Tumor Research Program and Neurology, Medical College of Wisconsin, Wisconsin, USA.
*Corresponding Author : Nathan T Zwagerman
Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, Wisconsin, USA.
Email: nzwagerman@mcw.edu
Received : Sep 07, 2022
Accepted : Oct 05, 2022
Published : Oct 12, 2022
Archived : www.jcimcr.org
Copyright : © Zwagerman NT (2022).
Abstract
Background: Parasagittal and Parafalcine Meningiomas (PSPF) have a higher rate of recurrence, increased risk of postoperative morbidities, and less favorable outcomes after stereotactic radiosurgery compared to other ocations. Herein, we try to find factors associated with treatment failure after radiosurgery in patients with PSPF meningiomas.
Methods: We retrospectively reviewed records of 104 patients with 130 Gamma Knife® Radiosurgery (GKRS) treatments for individual meningiomas at a single institution. 38 were PSPF compared to 92 in non-PSPF locations.
Results: The PSPF group showed a significantly higher rate of surgical intervention after radiosurgery compared to the non-PSPF group (18.4% vs 4.4, p = 0.008 in univariate analysis). The relative risk for a PSPF tumor requiring surgery after GKRS was 4.24, with an odds ratio of 4.97 (95% CI: [1.32-13.63], p = 0.015). The average tumor size between the PSPF group and the non-PSPF group was 3.53 cm3 and 2.28 cm3, respectively; this difference was statistically significant (p = 0.035) on univariant analysis, but not multivariate (p = 0.125). In the whole sample, for tumors >5 cm3, the relative risk ratio for needing surgery after GKRS was 6.23 with an odds ratio of 8.32 (95% CI: [2.25-30.67], p = 0.0015). Both PSPF and non-PSPF meningiomas were similar in gender, follow-up length, prior surgical intervention, and WHO grades.
Conclusion: Meningiomas’ outcome and response to radiosurgery depend on their location. We have two possible explanations. First, PSPF tumors are located near sensitive cerebral cortex areas. Second, the tumor’s mutational profile affects meningiomas’ location and prognosis.
Keywords: Parasagittal meningiomas; Parafalcine meningiomas; Gamma knife radiosurgery.
Abbreviations: SRS: Stereotactic Radiosurgery; IRB: Institutional Review Board; GKRS: Gamma Knife® Radiosurgery; PSPF: Parasagittal/Parafalcine; CNS: Central Nervous System; Gy: Gray; WHO: World Health Organization; PFS: Progression Free Survival; CI: Confidence Interval; OR: Odds Ratio.
Citation: Montoure AJ, Eraky AM, Campo EMD, Bovi J, Zwagerman NT, et al. Incidence of surgery after gamma knife radiosurgery for parasagittal and parafalcine meningiomas is higher than meningiomas in other locations: A 10-year institutional analysis and review of the literature. J Clin Images Med Case Rep. 2022; 3(10): 2099.
Introduction
Meningiomas are the most common benign primary brain tumor with an increasing incidence in our aging patient population. Surgical resection, Stereotactic Radiosurgery (SRS), and observation are acceptable and established first-line treatment options [1]. Without treatment, many meningiomas can continue to show growth at both linear and exponential rates [2-9]. Tumors that have demonstrated growth are more prone to develop progressive neurological symptoms prompting further treatment [9,10].
Historically, microsurgical resection has been the mainstay of meningioma treatment. Complication rates, Progression Free Survival (PFS), and recurrence rates are heavily dependent on tumor location, the extent of resection [11], patient age, [6,9,12] and tumor grade [13]. Complication rates can range from 4.4%-23.3% [6,9,14]. With long-term follow up, recurrence rates following surgery for grade I meningiomas can range from 20-32% [12,15]. Grade II and III meningiomas fair much worse with 5-year PFS of 50% and 13%, respectively [13].
SRS has been shown to be an acceptable primary and adjuvant treatment for meningiomas over the last two decades with well-established results [16-30]. For Grade I tumors, overall tumor control rates range from 85-97% [18,19,24,27-30], with 5-year PFS found to be between 86-98% and 10-year PFS ranging from 70-97%. As with microsurgery, higher grade meningiomas have worse results with 5-year PFS of 59% in grade II and 13% in grade III lesions [31]. Treatment-related side effects, such as increased peritumoral edema, can range from 8-25% following SRS [29,32-36], and have been documented to be as high as 43% in some studies [37].
As discussed above, upfront microsurgical resection and SRS demonstrate favorable tumor control rates and acceptable treatment-related side effects. However, the published data have demonstrated there are a minority of patients treated with upfront SRS continues to show tumor progression (3-15%) [18,19,24,27-30]. Unfortunately, there is a paucity of data in the published literature to suggest tumor and treatment-related characteristics that can predict failure of primary treatment.
In order to better define tumor and treatment-related characteristics that can predict failure following upfront SRS, we retrospectively evaluated meningiomas receiving Gamma Knife® Radiosurgery (GKRS) at a single institution between 2009-2019.
Methods
This study was performed with previous approval from our Institutional Review Board (IRB). This retrospective chart review evaluated meningiomas receiving Gamma Knife® Radiosurgery (GKRS) at a single institution between 2009-2019. Inclusion criteria required at least 12 months of documented follow up. As we discuss the incidence of surgery after Gamma Knife radiosurgery, tumors with prior GKRS retreatment were also excluded from the primary dataset. Eighteen GKRS treatments during this time were eliminated due to lack of follow up, and three were retreatments to the same lesion. The patient’s charts and relevant imaging were reviewed. Statistical analysis was performed using the IBM SPSS software to run a general linear model, both univariate and multivariate as well as Kaplan-Meier survival with log-rank Mantel-Cox analysis. A P-value of
Results
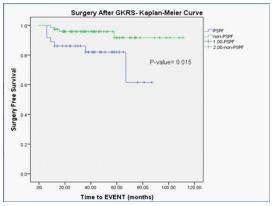
There were 130 GKRS treatments for individual meningiomas in 104 unique patients from 2009-2019 that met inclusion criteria. Seventy-six (73.1%) were female (F) and 28 (26.9%) were male (M), with an F:M ratio of 2.7:1. The average age at GKRS treatment was 57.2 years, with a range of 18-88. The mean follow up was 43.4 months, with a range of 12-111 months. Thirty-eight (29.2%) meningiomas were Parasagittal or Parafalcine (PSPF) compared to 92 (70.8%) in non-PSPF locations. Of all patients, 11/104 (10.6%) required surgical intervention after GKRS. When we evaluated only those patients where the tumor was in the PSPF location, 7/38 (18.4%) required surgery, compared to 4/92 (4.4%) from the non-PSPF group; this was a statistically significant finding in both univariate and multivariate analysis (P-value=0.008 and 0.050, respectively). The relative risk for a PSPF tumor requiring surgery after GKRS was 4.24, with an odds ratio of 4.97 (95% CI: [1.32-13.63], P-value= 0.015, z statistic 2.43). A Kaplan-Meier surgery-free survival analysis was performed (Figure 1); this was statistically significant (P-value= 0.015, Log Rank Mantel-Cox). Skull base tumors and non-skull base tumors were compared in the same manner. Fifty-eight (44.6%) were skull base and seventy-two (55.4%) were non-skull base. 3.4% (2/58) skull base tumors required surgery post GKRS compared to 12.5% (9/72) of non-skull base lesions. This approached, but did not reach, statistical significance (P-value= 0.066).
Total treatment failure, those who required surgery in addition to those who required re-radiation to the same lesion, was also statistically significant between the PSPF group and the non-PSPF group on univariate and multivariate analysis, with P-values 0.002 and 0.016, respectively (Table 1). Additional patient demographics and tumor location characteristics can be seen in Tables 1, 2, and 3. The two cohorts, PSPF, and non-PSPF were similar in terms of gender, follow-up length, and prior surgical intervention. Age and tumor size were statistically significant on univariate analysis but did not hold true on multivariate evaluation (Table 4).
Table 1: Incidence of treatment failure.
| Total treatment failureb | Patients (n) | Patients (%) | P-value (univariate) | P-value (Multivariate) |
|---|---|---|---|---|
| PSPF | 9 | 23.7 | 0.002* | 0.016* |
| Non-PSPF | 5 | 4.3 |
a.PSPF: Parasagittal/Parafalcine; GKRS: Gamma Knife Radio Surgery. b.Surgery + Repeat Gamma Knife Radio Surgery After Initial Gamma Knife. *Statistically Significant.
Table 2: Incidence of Surgery after Gamma Knife Radio Surgery.
| Patients (n) | Patients (%) | Surgery After GKRS (n) | Surgery After GKRS (%) | P-value (univariate) | P-value (Multivariate) | |
|---|---|---|---|---|---|---|
| PSPF | 38 | 29.2 | 7 | 18.4 | 0.008* | 0.05* |
| Non-PSPF | 92 | 70.8 | 4 | 4.4 | ||
| Skull base | 58 | 44.6 | 2 | 3.4 | 0.066 | .077 |
| Non-skull base | 72 | 55.4 | 9 | 12.5 |
a.PSPF: Parasagittal/Parafalcine; GKRS: Gamma Knife Radio Surgery. *Statistically Significant.
Table 3: Patient Demographics.
| Sex | Patient (n) Total Cohort | % | P-Value Univariate | P-Value Multivariate | Mean(Range) |
|---|---|---|---|---|---|
| Male | 28 | 26.9 | 0.150 | 0.142 | |
| Female | 76 | 73.1 | |||
| Age | 0.260 | 0.194 | 57.2 (18-88) | ||
| Follow up (months) | 0.101 | 0.074 | 43.4 (12-111) | ||
| Location | 0.709 | 0.911 | |||
| Parasagittal/Falcine | 38 | 29.2 | |||
| Convexity | 24 | 18.5 | |||
| Parasellar/Sellar | 18 | 13.8 | |||
| Sphenoid Wing | 12 | 9.2 | |||
| Posterior Fossa | 11 | 8.5 | |||
| Anterior Skull Base | 11 | 8.5 | |||
| entorial | 8 | 6.2 | |||
| Clival | 6 | 4.6 | |||
| Pineal | 1 | 0.8 | |||
| Intraventricular | 1 | 0.8 | |||
| Symptoms Prompting GKRS | 0.779 | 0.894 | |||
| Continued Tumor Growth | 74 | 56.8 | |||
| Neurological Deficit | 18 | 13.8 | |||
| Recurrence | 15 | 11.5 | |||
| Incidental | 13 | 10.2 | |||
| Residual | 10 | 7.7 | |||
| Surgery Prior to GKRS | 27 | 20.8 | 0.035* | 0.053 | |
| Surgical Cohort | 5 | 45.5 | |||
| Non-surgical Cohort | 22 | 18.5 | |||
| Gamma Knife Treatment Dose (Gy,50% isodose line) | 0.673 | 0.430 | 13.6 | ||
| Surgery after GKRS Cohort | 13.8 | ||||
| Non-surgical Cohort | 13.6 | ||||
| Gamma Knife Treatment Dose (Gy, Max) | 0.500 | 0.460 | 27.1 | ||
| Surgery after GKRS Cohort | 28.0 | ||||
| Non-surgical Cohort | Non-surgical Cohort | ||||
| Gamma Knife Complications | |||||
| None | 105 | 80.8 | |||
| Symptomatic Edema | 17 | 13.1 | |||
| Continued tumor growth | 6 | 4.6 | |||
| Alopecia | 2 | 1.5 |
a PSPF: Parasagittal/parafalcine; GKRS: Gamma Knife Radiosurgery; Gy: Gray.
Table 4: Cohort comparisons.
| Patient (n) PSPF group | % | Patient (n)Non-PSPF group | % | P-Value Univariate | P-value Multivariate | Mean (Range) for PSPF | Mean (Range) for non-PSPF | |
|---|---|---|---|---|---|---|---|---|
| Sex | 0.825 | 0.954 | ||||||
| Male | 10 | 27.0 | 23 | 31.5 | ||||
| Female | 27 | 73.0 | 55 | 75.3 | ||||
| Age | 0.036* | 0.059 | 60.7(28-86) | 54.4(18-88) | ||||
| Follow up Months) | 0.324 | 0.135 | 40.4(12-87) | 45.4(12-111) | ||||
| Surgery Prior to GKRS | 11 | 28.9 | 16 | 17.4 | 0.142 | 0.245 | ||
| Tumor Size (CM3) | 0.035* | 0.125 | 3.53 (0.13-12.27) | 2.28 (0.05-22.59) |
a.GKRS: Gamma Knife Radiosurgery; CM: Centimeter; PSPF: Parasagittal/Parafalcine. * Statistically Significant.
Table 5: Tumor size.
| Mean (Range) | P-Value Univariate | P-Value multivariate | |
|---|---|---|---|
| Tumor Size (CM3) in the Total cohort | 2.64 (0.05-22.59) | ||
| For Tumors Required Post-GKRS Surgical Intervention (CM3) | 6.37 (0.14-22.59) | < 0.001 | < 0.001 |
| For tumors Required Non-Surgical Intervention (CM3) | 2.30 (0.05-10.68) |
a.KRS: Gamma Knife Radiosurgery; CM: Centimeter.
Table 6: Surgical Data from Tumors Resected Post GKRS.
| Patient (n) Total Cohort | % | Patient (n) PSPF Group | % | Patient (n) Non-PSPF Group | % | Mean (Range) PSPF Group | Mean (Range)PSPF Group | |
|---|---|---|---|---|---|---|---|---|
| Time from GKRS to Surgery (Months) | 20.3 (6-67) | 23.8 (9-58) | ||||||
| Tumors required surgery < 12 Months post-GKRS(n) | 7 | 63.6 | 5 | 71.4 | 2 | 50.0 | ||
| Reason prompting Surgery | ||||||||
| Neurological Symptoms | 5 | 45.5 | 4 | 57.1 | 2 | 50.0 | ||
| Symptomatic Edema | 4 | 36.4 | 4 | 57.1 | 0 | 0 | ||
| Growth | 4 | 36.4 | 1 | 14.3 | 3 | 75.0 | ||
| Seizure | 2 | 18.2 | 2 | 28.6 | 0 | 0 | ||
| Surgical Complications | ||||||||
| Transient Neurological Deficit | 3 | 27.3 | 3 | 43 | 0 | 0 | ||
| Wound Infection | 1 | 9.1 | 1 | 14 | 0 | 0 | ||
| Extra Axial Hematoma- Non op | 1 | 9.1 | 1 | 14 | 0 | 0 | ||
| Hyponatremia | 1 | 9.1 | 0 | 0 | 1 | 25.0 | ||
| Hydrocephalus Resulting in Shunt (IV tumor) | 1 | 9.1 | 0 | 0 | 1 | 25.0 | ||
| 30-Day Mortality | 0 | 0 | 0 | 0 | 0 | 0 | ||
| Pathology | ||||||||
| WHO Grade | ||||||||
| Grade 1 | 8 | 73 | 5 | 71.4 | 3 | 75.0 | ||
| Grade 2 | 2 | 18 | 2 | 28.6 | 0 | 0 | ||
| Grade 3 | 1 | 9 | 0 | 1 | 25.0 |
a.PSPF: Parasagittal/Parafalcine; GKRS: Gamma Knife Radiosurgery; IV: Intraventricular; WHO: World Health Organization; MIB-1: Proliferative Index.
Tumor size was statistically significant for those tumors requiring surgical intervention after GKRS. The average tumor size for those requiring surgery after GKRS was 6.37 cm3 with a range from 0.14-22.59 cm3, compared to 2.30 cm3 with a range of 0.05-10.68 cm3 for those who did not require surgery after GKRS (P-value=< 0.001 on both univariate and multivariate analysis) (Table 5). Volume was calculated from the MRI at the time of GKRS with the formula [V=4/3πa*b*c], where “a”, “b”, and “c” are the radii in the anterior-posterior, superior-inferior, and medial-lateral tumor dimensions. For tumors >5 cm3 relative risk ratio for needing surgery after GKRS was 6.23, with an odds ratio of 8.32 (95% CI 2.25-30.67, P-value 0.0015, z statistic 3.183). The average tumor size between the PSPF group and non-PSPF group was 3.53 cm3 and 2.28 cm3, respectively; this difference was statistically significant (P-value= 0.035) on univariant analysis, but not multivariate (P-value= 0.125).
The most common reason for GKRS was continued tumor growth in 74 patients (56.8%), followed by new or worsening neurological symptoms in 18 patients (13.8%), recurrence in 15 (11.3%), and residual in 10 (7.7%). The average Gamma Knife dose at the 50% isodose line was 13.6 Gy, with a max dose average of 27.1 Gy. This was not significantly different between the group requiring surgery after GKRS and those who did not (P-value= 0.673 and 0.500, respectively). All but three patients received single fraction treatment. In 103 tumors (79.2%) GKRS was the initial treatment, meaning only 27 tumors (20.8%) had surgery prior to their GKRS. For those undergoing surgical intervention after GKRS, this was a significant factor (P-value= 0.035). Hospital admission for CNS-related reasons within 12 months of GKRS was also a statically significant factor for those requiring surgery after GKRS (P-value= < 0.001), with a relative risk of 10.80 and an odds ratio of 22.56 (95% CI: [5.09-100.02], P value=<0.001, z statistic 4.101). Patients who were admitted within this time frame but did not require surgical intervention were treated with increasing steroids in three incidences, and anti-epileptic adjustment in one case.
Our post-Gamma Knife complication rate was 19.2% with 17 patients (13.1%) experiencing symptomatic peri-tumoral edema, 6 (4.6%) with continued tumor growth, and 2 (1.5%) with mild alopecia. Of those with symptomatic edema, 7 underwent surgery, 1 had repeat GKRS (atypical lesion with recurrence was outside the original field), and 9 were treated successfully with steroids or increasing anti-epileptic medications. The decision for surgery was based on patient response/tolerability of steroids or improvement of seizures with medication.
Eleven patients (11/125, 8.8%) underwent surgical resection of their tumors after GKRS. The mean time from GKRS to surgery was 21.6 months with a range of 6-67 months. Seven of these cases (63.6%) occurred less than 12 months after GKRS. Reasons for prompting surgery included edema with new/worsening neurological symptoms in 7 of the cases, with 4 additionally demonstrating interval tumor growth. Three patients had transient neurological deficits postoperatively, one had a wound infection, and one patient with an intraventricular tumor required ventricular peritoneal shunt placement for hydrocephalus. Eight tumors (72.7%) were WHO grade I, two were grade II (18.2%), and one was a grade III (9.1%) meningioma. The average Mib-1 labeling index, a proliferation biomarker, was 6.37, with a range of 2.1-23.0. There were similar WHO grades between the PSPF and non-PSPF groups, with 71.5% and 75% classified as WHO grade I tumors, respectively (Table 6).
Discussion
Meningiomas are the most common benign primary intracranial brain tumor [1,6]. Meningiomas arise from the arachnoid cap cells and can occur anywhere these cells exist with the five most common locations being PSPF (28.8%), convexity (15.2%), tuberculum sellae (12.8), sphenoid ridge (11.9%), and olfactory groove (9.8%) [38]. Similarly, in our study, PSPF accounts for 29.2% of all meningiomas. Current meningioma grading uses the WHO classification [39], which is based on histological criteria and has an inter observer concordance rate of 87.2% [40].
The natural history of meningiomas has been well described in the literature. The majority of tumors will eventually progress or cause neurological sequelae. Kim et al. followed 201 patients with new asymptomatic meningiomas and showed that 70% eventually had tumor progression, with one-third of those eventually requiring intervention during 5-year follow up [5]. Other studies have shown rates of progression ranging from 31-63% in conservative treatment groups [2-4,6-9], and relative annual progression rates of 0.48-72.8%, with a mean of 14.6% [7].
Several patient and radiographical factors have been attributed to higher rates of progression. Patient factors predictive of progression include younger age, male sex, and presence of neurological symptoms; radiological factors include lack of calcification, T2 hyperintensity, and peritumoral edema [7,8]. Tumor volume has been shown to be predictive of higher annual progression rates in some studies,[8] but not predictive in others [7].
Microsurgical resection remains a well-established and accepted potential first-line treatment for meningiomas. The extent of resection is quantified using the Simpson Grading Scale, which was first published in 1957 [41]. Several studies evaluating long-term results for grade I meningiomas have been published. Mallio et al. evaluated 149 patients with complete resection and found a 13.4% recurrence rate over 20 years, with the majority of cases recurring within 30 months [42]; similarly, Alkemade et al found 18%, 26%, and 32% recurrence rates at five, ten, and fifteen years, respectively, with higher Simpson grade and lower age being significantly associated with higher recurrence rates [12]. Higher WHO grade tumors have significantly worse overall survival and 5-year PFS after surgery, with grade II PFS being only 50% and grade III being 13% at five years post-surgery [13]. Dobran et al evaluated atypical, grade II, meningiomas over a 10-year period and found that recurrence free survival, but not overall survival, was influenced by the extent of resection. They also found that Mib-1 proliferation index greater than 8 was a negative predictor for recurrence, but a pre-operative Karnoky performance scale (KPS) greater than 80 was a positive predictor value for overall survival [42]. The complication profile for microsurgical intervention varies depending on patient age, tumor location, and extent of resection. Yano et al demonstrated a 4.4% morbidity rate for those under 70 years of age, compared to a 9.4% morbidity rate in those greater than 70 years old [9]. Kuratsu et al also demonstrated the increased morbidity for those older than 70 years was 23.3% [6]. Dobran et al. evaluated patients greater than 80 years old undergoing meningioma resection and found there is a close correlation between operative time over 240 minutes and mortality at 1 month (P=0.0421), as well as lower mortality for ASA (American Society of Anesthesiologists physical status classification) II compared to ASA III patients (P=0.038) [43]. Other large studies show overall morbidity ranging from 8.6-35% [14,44–49].
SRS is also a well-established and accepted first-line treatment for meningiomas, or as adjuvant therapy following incomplete resection. When comparing SRS as an initial treatment versus observation, there is a statistically significant effect on PFS with SRS [4]. Kim et al. showed the 5-year clinical PFS between those receiving SRS as an initial treatment versus observation alone was 98.7% and 64.6%, and the 10-year radiographic PFS was 88.5% and 7.9%, respectively [5]. For grade I tumors, overall tumor control rates generally range from 85-97%, [18,19,24,27-30] with 5-year PFS between 86-98% and 10-year PFS ranging from 70-97% [5,17-19,21-26,30,50]. After SRS, meningiomas have shown regression 14-82% of the time [17-19,21-25,27,30].
Adjuvant SRS has shown benefit in multiple studies and has become a common practice, especially after subtotal resection of high-grade lesions in many institutions. Taylor et al. showed an actuarial local control rate at 10 years of 18% in subtotal resection alone, 77% in total resection alone, and 82% in the combination of subtotal resection and SRS [51]. Other studies have shown the benefit of adjuvant SRS even after complete tumor resection [52]. Additionally, early delivery of SRS after subtotal resection or early recurrence can decrease future progression to higher-grade meningiomas [53]. For higher grade lesions, however, adjuvant radiation may delay but not prevent recurrence [42].
Not all meningiomas respond the same to SRS, and tumor characteristics in such cases are not as well established. Time to progression following SRS is widely variable between cases ranging from 1.2 months to greater than 10 years [16,21-23,25,30,54]. Tumor factors such as location other than skull base, diameter greater than 2.5 cm, higher proliferative index, increasing WHO grade, and those with meningiomatosis are at higher risk for progression after treatment. Additional treatment-related factors predictive of progression include incomplete tumor coverage and history of previous surgery or radiation [30,54].
Treatment-related side effects can occur following SRS for meningioma. The most common side effect following SRS is an increase in peritumoral edema. Its incidence can range from 8-43% [5,20,29,30,32-37]. In our study, we found that the peritumoral edema incidence after SRS is 13.1%. Of interest, about 53% of those patients who developed edema were treated successfully with corticosteroids and anti-epileptic drugs, and about 41% needed surgery; Only 6% required repeated SRS. Several studies have evaluated tumor-related factors predictive of post-SRS edema. Tumor volume has been predictive in some studies [29,30,32,37], but not in others[33,36]. Cai et al. showed for every 1 cm2 increase in brain/tumor contact area, the odds of developing symptomatic edema increased by 17% [32]. Tumor location, specifically parasagittal or midline, has shown a higher likelihood of post-treatment edema [33,35,36] Patil et al. showed that 29% of patients with PSPF tumors developed symptomatic edema compared to 7.5% in other locations (P-value=0.0053, OR 4.1) [35], and Singh et al. had similar results with 22% of the non-skull base tumors (all parasagittal) developing symptomatic edema compared to 6% of the basal tumors [36]. Other potential risk factors for post-SRS-related edema include the extent of pre-treatment edema, previous resection, superior sagittal sinus occlusion, higher tumor grade, higher dose of radiotherapy, and single fraction treatment [29,32,34]. However, a clear consensus of factors causing post-SRS-related edema is lacking [55]. Additional treatment-related side effects following SRS include memory loss (6%), cranial nerve palsies (6.8%), ataxia (2.6%), seizures (1.7%), and numbness (0.9%) [20].
Thirty percent of meningiomas occur in the PSPF location and have been shown to demonstrate post-surgical morbidity [38,56]. In 1984, Giombini et al. demonstrated in a large surgical series of 342 PSPF tumors a 7% risk of peri-operative mortality and a 24% complication rate [46]. This demonstrated that PSPF tumors have a higher rate of recurrence and increased risk of injury to major venous structures compared to other locations [46]. Surgical techniques have advanced over the last 30 years; however, these tumors still pose a surgical challenge. PSPF meningiomas are often in close proximity to the superior sagittal sinus. Invasion of the superior sagittal sinus is seen in 25-45% of cases, making complete resection difficult [48,49,57]. Achieving a Simpson Grade I/II or gross total resection in PSPF meningiomas ranges from 28-85% [45,47,49,56,58,59]. Recurrence rates following surgery are between 11-27% during two-year follow up [45,47,59], with up to 47% recurring after 25-year follow up [56]. Surgical complications range from 8-35% in most studies [43,47-49,59]. Venous infarct or thrombosis are the most common post-surgical complications seen occurring in up to 10% of cases [47,48].
SRS for PSPF meningiomas has shown less favorable outcomes than treatment of meningiomas in non-PSPF locations. Five-year PFS ranges from 70-90% [57,60–62], and one study with long-term follow up found a 10-year PFS of only 55% [61]. Our results are similar to what we found in the literature. We found that the total treatment failure is statistically significant between the PSPF group and the non-PSPF group. These data are less favorable when compared to the previously discussed studies regarding SRS in the treatment of meningiomas at the skull base or if all other locations are included. Kondziolka et al. found on multivariate analysis there was decreased tumor control associated with increasing tumor volume and preexisting neurologic deficit. When they evaluated small, intact PSPF meningiomas with a volume less than 7.5 cc, there were no documented treatment failures [61]. Post-treatment edema was seen in 5.2-43% of cases [57,60,61,63,64], with an elevated edema index starting at 6 months post-treatment and median time to peak onset was 36 months [62]. Hasegawa et al. found a significantly higher post-treatment side effect rate in patients who underwent SRS as initial treatment for PSPF meningiomas [63]. Both Sheehan et al. and Ding et al. had 14% and 13.3% of patients respectively who required surgical intervention after SRS during their follow up period [60,63], similar to the rate shown in our evaluation.
The decision on when and how to treat meningiomas is patient-centered and discussed at a weekly multidisciplinary tumor board meeting at our institution. Neuro-oncology, radiation oncology, pathology, radiology, and neurosurgeons are involved in this process. GKRS was typically considered when the maximum diameter of the tumor was less than 3 cm; only 3 (2.3%) of tumors treated in this cohort had a maximum diameter greater than 3 cm. Other constraints that would preclude gamma knife are location, proximity/involvement of critical structure, and prior radiotherapy. Patient preference in discussing treatment options was one of the main factors in the decision making; 42 (32.3%) patients in this group elected for minimally invasive GKRS as upfront treatment. Other factors deciding treatment included unfavorable tumor location for surgery in 29 (22.3%) patients, tumor size in 19 (14.6%), patient co-morbidities in 15 (11.5%), treatment for recurrence in 14 (10.8%), patient advanced age in 8 (6.2%), and residual tumor in 3 (2.3%). Of the young patients less than 40 years of age (n=14), five had a history of childhood cancer with cranial radiation and multiple lesions throughout the brain making GKRS the preferred first-line modality of treatment.
Overall, our retrospective review demonstrated excellent local control (89.2%) of all meningiomas undergoing GKRS. However, for meningiomas in the PSPF region, there was a higher rate of surgical intervention after GKRS compared to those meningiomas treated in non-PSPF locations. Tumor size, as well as location, is vastly important when deciding on a treatment modality. While the overall rate of surgical intervention following GKRS remains low, these outcomes can help guide patient and physician discussion in regard to treatment recommendations for PSPF meningiomas.
An explanation of the results is the location of the PSPF tumors near eloquent or sensitive cerebral cortex areas. Post-treatment changes may result in tumor swelling and cause significant symptoms in the region of the motor/sensory cortices or associated regions. For instance, a tumor near the apex of the right frontal cortex would tolerate growth or swelling much better than a tumor near eloquent cortex areas.
An alternative explanation could lie in the individual tumor genetic profile. Over the last several years, the genetic landscape of meningiomas has been investigated but has had little effect on clinical decision making at this time. Several genetic mutations have been associated with meningiomas including NF2, TRAF7, AKT1, KLF4, PIK3CA, SMO, POLR2A, and SMARCB1 [65-75]. Yuzawa et al reviewed a large series of meningiomas and found that 80% of cases harbored at least one of these mutations [75], with NF2 being the most commonly mutated gene found in 50-82% of sporadic meningiomas [66,70,71]. Several studies have shown the mutational profile can predict its anatomical location [65,68-70,72-75]. For example, tumors harboring NF2 mutations are more commonly located in the convexity or along the falx [69,70,75], whereas those with TRAF7, AKT1, or SMO are located in the anterior skull base or medial middle fossa [68,69,73,75]. In addition to location, histological subtype, grade, and even prognosis have been associated with the mutational profile of meningiomas [66,68-70,74,75]. Sahm et al found six clinically relevant DNA methylation classes of meningiomas [72]. It was shown that these classes were a better predictor of patient outcome than WHO classification by identifying high-risk grade I tumors and low-risk grade II tumors, improving the clinical basis for or against additional therapy after surgery [5,9]. Similarly, Patel et al used RNA and whole exome sequencing to find three distinct types of meningiomas that correlate with clinical outcomes better than WHO classifications, as well as anatomical location [76].
Understanding the genetic landscape of meningiomas and how it will change clinical decisions is in its infancy. It has been shown that location and prognosis are variables affected by the tumor’s mutational profile. Many questions, however, still need answering, such as do specific mutation types respond differently to radiation and are there medications available that can target these mutations? With this study, we showed that parasagittal and parafalcine meningiomas have a higher incidence of surgery after GKRS than tumors in other locations, and we are hypothesizing that one of the reasons may lie within genetics. Further studies are needed as the knowledge and understanding of meningioma genetics continues to grow.
Limitations
Limitations of this study include its retrospective nature, which allows for selection bias. The overall cohort and tumors treated were of decent size; however, the primary endpoint- surgery after GKRS was a small sample. A larger, multicenter study with higher power would give additional strength to the results seen here. Also, the length of follow up is frequently a concern when studying meningiomas as they are slow growing and ideally would have follow up of several years.
Conclusion
Our retrospective review has demonstrated excellent local control (89.2%) of all meningiomas undergoing GKRS. For meningiomas in the PSPF region, there was a higher rate of surgical intervention after GKRS compared to those meningiomas treated in non-PSPF locations. While the overall rate of surgical intervention following GKRS remains low, our institutional outcomes are hypothesis generating for consideration of further clinical trials in meningioma management; including the tumors’ genetic makeup, radiation sensitivity for specific histological variants, and genetic mutations, as well as precision medicine based on these results. These outcomes can help guide patient and physician discussion regarding treatment recommendations for PSPF meningiomas.
Declarations
Conflict of interest: The authors declare no competing interests.
Funding: Not applicable.
Ethics approval and informed consent: This study was approved by our Institutional Review Board. Patient consent was not sought due to the retrospective nature of this study.
Previous publications: Portions of this work were presented at the North American Skull Base Society (NASBS) meeting, February 8th, 2020 as an oral presentation.
Acknowledgments: The Biostatistics Department at the Medical College of Wisconsin reviewed the statistics in the manuscript.
References
- Wiemels J, Wrensch M, Claus EB. Epidemiology and etiology of meningioma. J Neurooncol. 2010; 99: 307–314.
- Hashiba T, Hashimoto N, Izumoto S, et al. Serial volumetric assessment of the natural history and growth pattern of incidentally discovered meningiomas: Clinical article. JNS. 2009; 110: 675–684.
- Jadid KD, Feychting M, Höijer J, Hylin S, Kihlström L, Mathiesen T, et al. Long-term follow-up of incidentally discovered meningiomas. Acta Neurochir. 2015; 157: 225–230.
- Jo K-W, Kim C-H, Kong D-S, et al.: Treatment modalities and outcomes for asymptomatic meningiomas. Acta Neurochir. 2011; 153: 62–67.
- Kim KH, Kang SJ, Choi JW, Kong DS, Seol HJ, et al. Clinical and radiological outcomes of proactive Gamma Knife surgery for asymptomatic meningiomas compared with the natural course without intervention. Journal of Neurosurgery. 2019; 130: 1740–1749.
- Kuratsu J, Kochi M, Ushio Y. Incidence and clinical features of asymptomatic meningiomas. Journal of Neurosurgery. 2000; 92: 766–770.
- Nakamura M, Roser F, Michel J, Jacobs C, Samii M, et al. The natural history of incidental meningiomas. Neurosurgery. 2003; 53: 62–70.
- Oya S, Kim SH, Sade B, Lee JH. The natural history of intracranial meningiomas. Clinical article. JNS. 2011; 114: 1250–1256.
- Yano S, Kuratsu J, et al. Indications for surgery in patients with asymptomatic meningiomas based on an extensive experience. JNS. 2006; 105: 538–543.
- Sughrue ME, Rutkowski MJ, Aranda D, Barani IJ, McDermott MW, et al. Treatment decision making based on the published natural history and growth rate of small meningiomas: A review and meta-analysis. JNS. 2010; 113: 1036–1042.
- Sughrue ME, Kane AJ, Shangari G, Rutkowski MJ, McDermott MW, et al. The relevance of Simpson Grade I and II resection in modern neurosurgical treatment of World Health Organization Grade I meningiomas: Clinical article. JNS. 2010; 113: 1029–1035.
- van Alkemade H, de Leau M, Dieleman EMT, et al. Impaired survival and long-term neurological problems in benign meningioma. Neuro-Oncology. 2012; 14: 658–666.
- Adeberg S, Hartmann C, Welzel T, et al. Long-Term Outcome After Radiotherapy in Patients With Atypical and Malignant Meningiomas Clinical Results in 85 Patients Treated in a Single Institution Leading to Optimized Guidelines for Early Radiation Therapy. International Journal of Radiation Oncology*Biology*Physics. 2012; 83: 859–864.
- Zeng L, Wang L, Ye F, Chen J, Lei T, Chen J, et al. Clinical characteristics of patients with asymptomatic intracranial meningiomas and results of their surgical management. Neurosurg Rev. 2015; 38: 481–488.
- Adegbite AB, Khan MI, Paine KWE, Tan LK, et al. The recurrence of intracranial meningiomas after surgical treatment. Journal of Neurosurgery. 1983; 58: 51–56.
- Couldwell WT, Cole CD, Al-Mefty O, et al. Patterns of skull base meningioma progression after failed radiosurgery. JNS. 2007; 106: 30–35.
- Davidson L, Fishback D, Russin JJ, et al. Postoperative Gamma Knife surgery for benign meningiomas of the cranial base. FOC. 2007; 23: E6.
- DiBiase SJ, Kwok Y, Yovino S, et al. Factors predicting local tumor control after gamma knife stereotactic radiosurgery for benign intracranial meningiomas. International Journal of Radiation Oncology*Biology*Physics. 2004; 60: 1515–1519.
- Feigl GC, Bundschuh O, Gharabaghi A, Samii M, Horstmann GA, et al. Volume reduction in meningiomas after gamma knife surgery. Journal of Neurosurgery. 2005; 102: 189–194.
- Gupta A, Xu Z, Cohen-Inbar O, et al. Treatment of Asymptomatic Meningioma With Gamma Knife Radiosurgery: Long-Term Follow-up With Volumetric Assessment and Clinical Outcome. Neurosurg. 2019; 85: E889–E899.
- Han JH, Kim DG, Chung HT, Park CK, Paek SH, Kim CY, et al. Gamma Knife Radiosurgery for Skull Base Meningiomas: Long-Term Radiologic and Clinical Outcome. International Journal of Radiation Oncology*Biology*Physics. 2008; 72: 1324–1332.
- Iwai Y, Yamanaka K, Ikeda H, et al. Gamma Knife radiosurgery for skull base meningioma: long-term results of low-dose treatment: Clinical article. JNS. 2008; 109: 804–810.
- Kollová A, Liščák R, Novotný J, Vladyka V, Šimonová G, et al. Gamma Knife surgery for benign meningioma. JNS. 2007; 107: 325–336.
- Kondziolka D, Mathieu D, Lunsford LD, Martin JJ, Madhok R, et al. RADIOSURGERY AS DEFINITIVE MANAGEMENT OF INTRACRANIAL MENINGIOMAS. Neurosurgery. 2008; 62: 53–60.
- Kreil W. Long term experience of gamma knife radiosurgery for benign skull base meningiomas. Journal of Neurology, Neurosurgery & Psychiatry. 2005; 76: 1425–1430.
- Malik I, Rowe J, Walton L, Radatz M, Kemeny A, et al. The use of stereotactic radiosurgery in the management of meningiomas. British Journal of Neurosurgery. 2005; 19: 13–20.
- Pollock BE. Stereotactic radiosurgery for intracranial meningiomas: Indications and results. FOC. 2003; 14: 1–7.
- Sheehan JP, Williams BJ, Yen CP. Stereotactic radiosurgery for WHO grade I meningiomas. J Neurooncol. 2010; 99: 407–416.
- Unger KR, Lominska CE, Chanyasulkit J, et al. Risk Factors for Posttreatment Edema in Patients Treated With Stereotactic Radiosurgery for Meningiomas. Neurosurgery. 2012; 70: 639–645.
- Zada G, Pagnini PG, Yu C, Erickson KT, Hirschbein J, et al. Long-term Outcomes and Patterns of Tumor Progression After Gamma Knife Radiosurgery for Benign Meningiomas. Neurosurgery. 2010; 67: 322–339.
- Ding D, Starke RM, Hantzmon J, Yen CP, Williams BJ, et al. The role of radiosurgery in the management of WHO Grade II and III intracranial meningiomas. FOC. 2013; 35: E16.
- Cai R, Barnett GH, Novak E, Chao ST, Suh JH, et al. Principal Risk of Peritumoral Edema After Stereotactic Radiosurgery for Intracranial Meningioma Is Tumor-Brain Contact Interface Area. Neurosurgery. 2010; 66: 513–522.
- Chang JH, Chang JW, Choi JY, Park YG, Chung SS, et al. Complications after gamma knife radiosurgery for benign meningiomas. Journal of Neurology, Neurosurgery & Psychiatry. 2003; 74: 226–230.
- Kan P, Liu JK, Wendland MM, Shrieve D, Jensen RL, et al. Peritumoral edema after stereotactic radiosurgery for intracranial meningiomas and molecular factors that predict its development. J Neurooncol. 2007; 83: 33–38.
- Patil CG, Hoang S, Borchers DJ, et al. Predictors of peritumoral edema after stereotactic radiosurgery of supratentorial meningiomas. Neurosurgery. 2008; 63: 435–442.
- Singh VP, Kansal S, Vaishya S, Julka PK, Mehta VS, et al. Early complications following gamma knife radiosurgery for intracranial meningiomas. Journal of Neurosurgery. 2000; 93: 57–61.
- Kim DG, Kim CH, Chung HT, Paek SH, Jeong SS, Han DH, et al. Gamma knife surgery of superficially located meningioma. Journal of Neurosurgery. 2005; 102: 255–258.
- Yamashita J, Handa H, Iwaki K, Abe M. Recurrence of intracranial meningiomas, with special reference to radiotherapy. Surg Neurol. 1980; 14: 33–40.
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016; 131: 803–820.
- Rogers CL, Perry A, Pugh S, et al. Pathology concordance levels for meningioma classification and grading in NRG Oncology RTOG Trial 0539. Neuro Oncol. 2016; 18: 565–574.
- Simpson D. The recurrence of intracranial meningiomas after surgical treatment. Journal of Neurology, Neurosurgery & Psychiatry. 1957, 20: 22–39.
- Dobran M, Marini A, Splavski B, Rotim K, Liverotti V, et al. Surgical Treatment and Predictive Factors for A typical Meningiomas: A Multicentric Experience. World Neurosurgery. 2020; 144: e1–e8.
- Dobran M, Marini A, Nasi D, Liverotti V, Benigni R, et al. Surgical treatment and outcome in patients over 80 years old with intracranial meningioma. Clinical Neurology and Neurosurgery. 2018; 167: 173–176.
- Maillo A, Orfao A, Espinosa AB, et al. Early recurrences in histologically benign/grade I meningiomas are associated with large tumors and coexistence of monosomy 14 and del (1p36) in the ancestral tumor cell clone. Neuro-Oncology. 2007; 9: 438–446.
- Eichberg DG, Casabella AM, Menaker SA, Shah AH, Komotar RJ, et al. Parasagittal and parafalcine meningiomas: Integral strategy for optimizing safety and retrospective review of a single surgeon series. British Journal of Neurosurgery. 2020; 34: 559–564.
- Giombini S, Solero CL, Lasio G, Morello G. Immediate and late outcome of operations for parasagittal and falx meningiomas. Report of 342 cases. Surgical Neurology. 1984; 21: 427–435.
- Raza SM, Gallia GL, Brem H, Weingart JD, Long DM, et al. Perioperative and Long-term Outcomes From the Management of Parasagittal Meningiomas Invading the Superior Sagittal Sinus. Neurosurgery. 2010; 67: 885–893.
- Skudas G, Tamasauskas A. [Prognosis of the surgical treatment of parasagittal meningioma]. Medicina (Kaunas). 2002; 38: 1089–1096.
- Sughrue ME, Rutkowski MJ, Shangari G, Parsa AT, Berger MS, et al. Results with judicious modern neurosurgical management of parasagittal and falcine meningiomas: Clinical article. JNS. 2011; 114: 731–737.
- Starke RM, Williams BJ, Hiles C, Nguyen JH, Elsharkawy MY, et al. Gamma Knife surgery for skull base meningiomas: Clinical article. JNS. 2012; 116: 588–597.
- Taylor BW, Marcus RB, Million RR. The meningioma controversy: Postoperative radiation therapy. International Journal of Radiation Oncology*Biology*Physics. 1987; 13: 106.
- Komotar RJ, Iorgulescu JB, Raper DMS, et al. The role of radiotherapy following gross-total resection of atypical meningiomas: Clinical article. JNS. 2012; 117: 679–686.
- Harris AE, Lee JYK, Omalu B, Flickinger JC, Kondziolka D, et al. The effect of radiosurgeryduring management of aggressive meningiomas. Surgical Neurology. 2003; 60: 298–305.
- Przybylowski CJ, Raper DMS, Starke RM, Xu Z, Liu KC, et al. Stereotactic radiosurgery of meningiomas following resection: Predictors of progression. Journal of Clinical Neuroscience. 2015; 22: 161–165.
- Milano MT, Sharma M, Soltys SG, et al. Radiation-Induced Edema After Single-Fraction or Multifraction Stereotactic Radiosurgery for Meningioma: A Critical Review. International Journal of Radiation Oncology*Biology*Physics. 2018; 101: 344–357.
- Pettersson-Segerlind J, Orrego A, Lönn S, Mathiesen T, et al. Long-Term 25-Year Follow-up of Surgically Treated Parasagittal Meningiomas. World Neurosurgery. 2011; 76: 564–571.
- Sheehan JP, Cohen-Inbar O, Ruangkanchanasetr R, et al. Post-radiosurgical edema associated with parasagittal and parafalcine meningiomas: a multicenter study. J Neurooncol. 2015; 125: 317–324.
- Colli BO, Carlotti CG, Assirati JA, dos Santos MBM, Neder L, et al. Parasagittal meningiomas: Follow-up review. Surgical Neurology. 2006; 66: S20–S27.
- Nowak A, Marchel A. Surgical treatment of parasagittal and falx meningiomas. Neurol Neurochir Pol. 2007; 41: 306–314.
- Ding D, Xu Z, McNeill IT, Yen CP, Sheehan JP, et al. Radiosurgery for parasagittal and parafalcine meningiomas: Clinical article. JNS. 2013; 119: 871–877.
- Kondziolka D, Flickinger JC, Perez B. Judicious Resection and/or Radiosurgery for Parasagittal Meningiomas: Outcomes from a Multicenter Review: Neurosurgery. 1998; 43: 405–413.
- Sheehan JP, Lee CC, Xu Z, Przybylowski CJ, Melmer PD, et al. Edema following Gamma Knife radiosurgery for parasagittal and parafalcine meningiomas. JNS. 2015; 123: 1287–1293.
- Hasegawa T, Kida Y, Yoshimoto M, Iizuka H, Ishii D, et al. Gamma Knife surgery for convexity, parasagittal, and falcine meningiomas: Clinical article. JNS. 2011; 114: 1392–1398.
- Girvigian MR, Chen JCT, Rahimian J, Miller MJ, Tome M, et al. Comparison of early complications for patients with convexity and parasagittal meningiomas treated with either stereotactic radiosurgery or fractionated stereotactic radiotherapy. Neurosurgery. 2008; 62: A19–A28.
- Abedalthagafi M, Bi WL, Aizer AA, et al. Oncogenic PI3K mutations are as common as AKT1 and SMO mutations in meningioma. Neuro Oncol. 2016; 18: 649–655.
- AlSahlawi A, Aljelaify R, Magrashi A, et al. New insights into the genomic landscape of meningiomas identified FGFR3 in a subset of patients with favorable prognoses. Oncotarget. 2019; 10: 5549–5559.
- Bi WL, Greenwald NF, Abedalthagafi M, et al. Genomic landscape of high-grade meningiomas. npj Genomic Med. 2017; 2: 15.
- Boetto J, Bielle F, Sanson M, Peyre M, Kalamarides M, et al. SMO mutation status defines a distinct and frequent molecular subgroup in olfactory groove meningiomas. NEUONC. 2017; now276.
- Clark VE, Erson-Omay EZ, Serin A, et al. Genomic analysis of non-NF2 meningiomas reveals mutations in TRAF7, KLF4, AKT1, and SMO. Science. 2013; 339: 1077–1080.
- Kros J, de Greve K, van Tilborg A, et al. NF2 status of meningiomas is associated with tumour localization and histology. J Pathol. 2001; 194: 367–372.
- Riemenschneider MJ, Perry A, Reifenberger G. Histological classification and molecular genetics of meningiomas. The Lancet Neurology. 2006; 5: 1045–1054.
- Sahm F, Schrimpf D, Stichel D, et al. DNA methylation-based classification and grading system for meningioma: A multicentre, retrospective analysis. The Lancet Oncology. 2017; 18: 682–694.
- Strickland MR, Gill CM, Nayyar N, et al. Targeted sequencing of SMO and AKT1 in anterior skull base meningiomas. Journal of Neurosurgery. 2017; 127: 438–444.
- Youngblood MW, Duran D, Montejo JD, et al. Correlations between genomic subgroup and clinical features in a cohort of more than 3000 meningiomas. Journal of Neurosurgery. 2020; 133: 1345–1354.
- Yuzawa S, Nishihara H, Tanaka S. Genetic landscape of meningioma. Brain Tumor Pathol. 2016; 33: 237–247.
- Patel AJ, Wan YW, Al-Ouran R, et al. Molecular profiling predicts meningioma recurrence and reveals loss of DREAM complex repression in aggressive tumors. Cancer Biology. 2019.