
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Primary signet ring cell carcinoma of the lung: A case report
Shunchang Liu†; Weina Kong†; Xiang Lv†; Miyessar Anwar; Xiumin Ma; Fan Guo*; Chengming Liu*
1Department of Medical Laboratory Center, Tumor Hospital Affiliated to Xinjiang Medical University, Urumqi, Xinjiang, China.
†Equal Contribution.
*Corresponding Author : Fan Guo & Chengming Liu
Department of Medical Laboratory Center, Tumor Hospital Affiliated to Xinjiang Medical University, No 789 Suzhou Road, Urumqi, Xinjiang 830011, China.
Email: 2813910552@qq.com
Received : Sep 19, 2022
Accepted : Oct 20, 2022
Published : Oct 27, 2022
Archived : www.jcimcr.org
Copyright : © Guo F and Liu C (2022).
Abstract
Signet Ring Cell Carcinoma (SRCC) also known as mucocellular carcinoma, it is a cancer cell with a lot of mucus. Primary lung SRCC is an extremely rare type of lung cancer malignancy. At present, there is no standard treatment scheme for primary pulmonary SRCC at home and abroad. We describe the clinical symptoms of a unique primary lung SRCC and the evaluation of its efficacy after targeted drug therapy. The results suggest that after the immunohistochemical results of ALK are positive, the use of biological targeted therapy may be a better choice.
Citation: Liu S, Kong W, Lv X, Guo F, Liu C, et al. Primary signet ring cell carcinoma of the lung: A case report. J Clin Images Med Case Rep. 2022; 3(10): 2126.
Case description
The patient, a 56-year old male, was hospitalized with “cough, expectoration, hemoptysis with shortness of breath for more than one month”. The patient and his family members complained that the patient developed cough, expectoration with hemoptysis after catching a cold in late December 2021. The blood was dark red, and it started 1-3 times a day in the morning. The amount was not much, accompanied by shortness of breath and discomfort which was obvious after activity. After 5 days of anti-inflammatory treatment in the local clinic, the symptoms were not significantly improved. Later, the above symptoms were not improved significantly, it was recommended to transfer to the superior hospital after the local hospital improved the examination. Thus, the patient visited our hospital today and was admitted to our department with “right lung space occupying” in the outpatient department. Since the onset of the disease, the patient has been in a clear mind, in poor spirit, fair sleep, poor appetite, normal stool once a day, and normal urination. In the past six months, he has lost about 7-8 kg of weight. Specialist examination: Multiple enlarged lymph nodes can be reached in the left clavicle area, with partial fusion, ranging from about 4 cm x 5 cm. The texture is hard, the mobility is poor, there is no tenderness, and the surrounding skin is free of redness, swelling and ulceration. The remaining superficial lymph nodes were not significantly enlarged. The thorax was normal, there was no tenderness in the sternum, and there was no uplift or depression in the chest. The respiratory movement was symmetrical, the costal space was normal, the speech fibrillation was symmetrical on both sides, and there was no pleural friction or subcutaneous twist. Percussion was clear, breathing was regular, biphasic wheezing sound can be reached in both lungs, no expiratory prolongation, voice conduction was symmetrical, and there was no pleural friction sound.
Imaging examination: On January 28, 2022, the CT scan of Changji Baoshihua Hospital showed a space-occupying lesion in the right lung and enlarged lymph nodes in the mediastinum and hilar. On February 7, 2022, the CT (Figure 1) of Tumor Hospital Affiliated to Xinjiang Medical University, showed that there were multiple quasi circular transparent areas in both lungs, with significant changes in the upper lobes of both lungs; Soft tissue mass shadow can be seen in the right hilum and the middle and lower lobe of the right lung. The shape was irregular. The mass surrounds the middle and lower lobe bronchus of the right lung, the distal end of the middle lobe bronchus of the right lung was blocked, and the lower lobe bronchus of the right lung was narrow. The lesion was large, with a cross-sectional size of about 6.2 cm x 4.6 cm. After enhancement, it was obviously uneven; Diffuse patchy shadows with interlobular septal thickening were seen in the right lung; Multiple nodular shadows were seen in the middle and lower lobe of the right lung, lobulated, and burr shadows were seen around. The larger one was located in the middle lobe of the right lung, with a size of about 2.3 cm x 2.4 cm; Nodular shadow can be seen in the anterior basal segment of the lower lobe of the left lung, with a size of about 0.3 cm x 0.2 cm; Multiple nodules and mass shadows can be seen in bilateral lock area, mediastinum and hilar, the larger one was about 6.0 cm x 3.8 cm, located under the tracheal carina, and the mass protrudes to the left main bronchus locally. A small amount of liquid density shadow can be seen in the right thoracic cavity.

Ultrasound (Figure 2): the echo of several enlarged lymph nodes was detected on both sides of the neck and on both clavicles (Area IV, area V on the left and area V on the right). The left side was about 3.1 cm x 1.6 cm and the right side was about 3.7 cm x 2.0 cm. The lymph hilus structure was unclear and the blood flow signal was rich. Exploration of sitting position of bilateral pleural cavity: The echo of liquid dark area can be seen in the right pleural cavity, the deepest was about 1.6 cm, the sound can be transmitted internally, the echo of compressed lung tissue can be seen inside, and there was no obvious sign of effusion in the left pleural cavity. Exploration of pericardial cavity: No obvious liquid dark area echo is found. Diagnosis: Space occupying lesion of right lung (puncture biopsy was recommended).
On February 7, 2022, the left supraclavicular lymph node biopsy was performed under the guidance of ultrasound in our hospital.
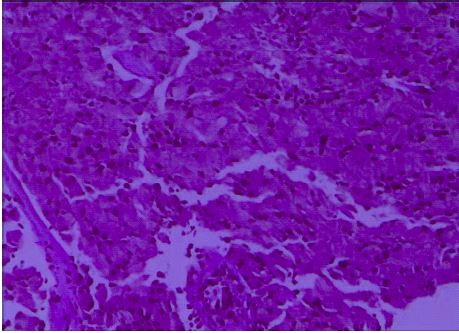
Postoperative pathology (Figure 3): Signet ring cell carcinoma was found in lymphoid tissue and fibrous connective tissue. Immunohistochemical results: CK7 (+), CK20 (-), Cdx-2 (-), satb-2 (-), villin (-), AE1 / AE3 (CK) (+), TTF-1 (+), napsin-a (+), Ki-67 (40% +). Signet ring cell carcinoma can be seen in lymphoid tissue and fibrous connective tissue. Combined with the results of immunohistochemical staining, it was suggested that it originated from the lung. Gene detection: Ros1 (-), ALK (d5f3) (+). The clinical diagnosis was primary signet ring cell carcinoma of the lung. On February 12, 2022, the patient began to take aletinib hydrochloride capsule 600 mg orally twice a day for targeted drug treatment.


One month later, re-examination of chest CT (Figure 4) showed that soft tissue mass shadow can be seen in the right hilum and the middle and lower lobe of the right lung, with irregular shape. The mass surrounded the middle and lower lobe bronchus of the right lung, the distal end of the middle lobe bronchus of the right lung was occluded, the lower lobe bronchus of the right lung was narrow, the lesion was large, the cross-section size was about 4.3 cm x 2.5 cm, and the range was smaller than that before (2022-02-07); Diffuse patchy shadows with interlobular septal thickening were seen in the right lung, and the range was narrower than before; Patchy shadow can be seen in the lower lobe of the right lung; Multiple nodular shadows can be seen in the middle and lower lobe of the right lung, lobulated, and burr shadows can be seen around. The larger one was located in the middle lobe of the right lung, about 2.1 cm x 1.5 cm in size, which was narrower than before; Nodular shadow, about 0.3 cm x 0.2 cm in size, can be seen in the anterior basal segment of the left lower lobe of the lung, which was similar to that in the previous case. Multiple nodules and mass shadows can be seen in bilateral lock area, mediastinum and hilar, the larger one was about 3.7 cm x 2.6 cm, which was located under the tracheal carina and smaller than before. A small amount of liquid density shadow can be seen in the right thoracic cavity, which was more than before. Efficacy evaluation: PR. At present, it is still being treated and followed up with aletinib hydrochloride.
Discussion
Signet Ring Cell Carcinoma (SRCC) also known as mucocellular carcinoma, it is a cancer cell with a lot of mucus. Because of its cell are full of mucus, the nucleus is biased to one side, it is shaped like a ring. Primary lung SRCC is an extremely rare type of lung cancer malignancy. At present, it is considered to be a subtype of lung adenocarcinoma. Pathologically, primary lung SRCC can be diagnosed as lung adenocarcinoma with more than 50% signet ring cells [1]. SRCC originates from undifferentiated stem cells in the lamina propria of mucosa. It is a subtype of mucus secreting adenocarcinoma. Often occurs in the gastrointestinal tract, but rarely in the lung. Primary SRCC is one of the subtypes of lung adenocarcinoma, but its prognosis is worse than other types of lung adenocarcinoma. The 5-year survival rate of patients is less than 30% [2]. Its occurrence may be related to ALK gene rearrangement, in which the positive proportion of EML4-ALK fusion gene is significantly higher than that of other types of lung adenocarcinoma [1]. CT findings of this disease showed multiple quasi circular transparent areas in both lungs, with significant changes in the upper lobes of both lungs; Soft tissue mass shadow can be seen in the right hilum and the middle and lower lobe of the right lung, with irregular shape. The mass surrounds the middle and lower lobe bronchus of the right lung, the distal end of the middle lobe bronchus of the right lung is blocked, the lower lobe bronchus of the right lung is narrow, the lesion is large, and it shows obvious uneven enhancement after enhancement; Diffuse patchy shadows with interlobular septal thickening were seen in the right lung; Multiple nodular shadows are seen in the middle and lower lobe of the right lung, lobulated, and burr shadows are seen around. The larger ones are located in the middle lobe of the right lung; Nodular shadows can be seen in the anterior basal segment of the lower lobe of the left lung, multiple nodules and mass shadows can be seen in bilateral lock areas, mediastinum and hilar, which are located under the carina of the trachea, and the mass locally protrudes to the left main bronchus. A small amount of liquid density shadow can be seen in the right thoracic cavity. Zhao Lei et al. [3] found that compared with lung mucinous adenocarcinoma, the density of SRCC lesions on plain CT scan is low, and non-enhanced areas can be seen after enhancement, and most of them are accompanied by intrapulmonary or lymph node metastasis, which is helpful for diagnosis. The tumor is located in the middle lobe of the right lung and grows close to the chest wall. After enhancement, it shows obvious uneven enhancement with multiple metastases in the lung, suggesting a high degree of malignancy. Castro et al [4]. Reported that the positive expression of TTF-1 and CK7 is helpful to the diagnosis of primary SRCC of the lung. Tadashi [5] showed in the latest report that: (CK) AE1 / 3, CK7, CK18, EMA, p53, Ki-67, CEA, CA19-9 and TTF-1 may be highly expressed in primary SRCC, while CK5 / 6, CK8, CK14, CK19, CK2, CD45, CD20, CD3 and Cdx-2 are low. The final diagnosis of pulmonary primary SRCC depends on pathological and immunohistochemical examination. ImImmunohistochemical staining is often positive for TTF-1, CK7 and napsina, and negative for CK20 and Cdx-2. This patient is in line with this requirement.
Conclusion
At present, there is no standard treatment scheme for primary pulmonary SRCC at home and abroad. In addition to surgery, paclitaxel combined with platinum is mostly used in clinical chemotherapy, but the overall curative effect is poor [6]. Yao Yake et al. [1] found that almost all tumors were positive for TTF-1 (18/20) and CK7 (14/14). Eight patients aged ≤ 50 years had ALK gene rearrangement, while only 38.5% of the older patients had ALK gene rearrangement (P = 0.007). With the progress of gene detection technology and the improvement of the speed of new drug research and development, biological targeted therapy has fully covered the first-line treatment of advanced NSCLC. From the data of median PFS, the curative effects of rare targets are more prominent, which have exceeded the curative effects of standard chemotherapy. According to PFS, they are: ALK (aletinib, PFS = 34.8 months), ros1 (seretinib, PFS = 19.3 months), RET (selpercatinib, PFS = 18.4 months), BRAF (darafinib + trimetinib, PFS = 14.6 months) Ntrk (larotinib, PFS ≥ 12 months), met (voritinib, PFS = 9.7 months) [7]. The result of ALK immunohistochemistry showed that the patient was positive, so it was suggested that the patient should take the targeted drug of aletinib orally 1 week later. After taking the drug for 1 month, the patient’s shortness of breath symptoms were significantly improved, and the curative effect evaluated by CT was pr. The results suggest that after the immunohistochemical results of ALK are positive, the use of biological targeted therapy may be a better choice.
Declarations
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- LI Guimei, YANG Zhihui, MEI Jia, CAO Xiaohui. Primary signet-ring cell carcinoma of lung: A clinical pathological analysis of 6 cases [J]. J Clin Exp Pathol. 2014; 30: 163-165+170.
- Tsuta K, Ishii G, Yoh K, Nitadori J, Hasebe T, et al. Primary lung carcinoma with signet-ring cell carcinoma components: Clinicopathological analysis of 39 cases. Am J Surg Pathol. 2004; 28: 868-874.
- Zhao Lei, Du Mingli, Wu Wenjuan, Li Guixiang. Primary signet-ring cell carcinoma of lung: Case report [J]. Chin J Interv Imaging Ther. 2020; 17: 17.
- Castro CY, Moran CA, Flieder DG, Suster S. Primary signet ring cell adenocarcinomas of the lung: A clinicopathological study of 15 cases. Histopathology. 2001; 39: 397-401.
- Tadashi T. Primary signet-ring cell carcinoma of the lung: A case report with an immunohistochemical study[J]. Int J Clin Exp Pathol. 2012; 5: 171-174.
- WANG Yajuan, LIU CHangting, LI Hongxia and PENG Liangz. A clinical study of 12 patients with primary signet ring cell carcinoma of lung and literature review [J]. Med J Chin PAPF. 2010; 21: 324-326, 330.
- JIANG Zhanshenga, ZHANG Yua, REN Xiubao, Pan Zhanyu. Research progression on the first-line biological target therapy of advanced non-small cell lung cancer [J]. Chin J Cancer Biother. 2020; 27: 843-851.