
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Enoxaparin-induced bullous hemorrhagic dermatosis adjacent to and distant from the injection site: A case report
Amir Hossein Hassani1; Zahra Hooshanginezhad2; Mojtaba Rezaei3; Fatemeh Azizi4*
1Medical Student, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
2Clinical Cardiologist, Shiraz University of Medical Sciences, Shiraz, Iran.
3Medical Doctor, Tropical and infectious disease research center, Hormozgan, Iran.
4Clinical Cardiologist, Cardiology Department, Alzahra Hospital, Shiraz University of Medical Sciences. Shiraz, Iran.
*Corresponding Author : Fatemeh Azizi, MD
Department of Cardiology, Alzahra Hospital, Shiraz University of Medical Sciences, Shiraz, Iran.
Tel: +987137355093; Cell: +98–917(392) 5902;
Email: azizi.f69@gmail.com
Received : Oct 17, 2022
Accepted : Nov 02, 2022
Published : Nov 09, 2022
Archived : www.jcimcr.org
Copyright : © Azizi F (2022).
Abstract
Background: Bullous hemorrhagic dermatosis is a rare and benign adverse effect happening on days 5-21 of treatment with heparin and Enoxaparin. It can be localized or generalized and occur in places adjacent to and distant from the subcutaneous injection site. It is mostly happening in the extremities, followed by the trunk and abdomen, and is very rare on the head and neck. Our reported case had lesions on the forehead, neck, trunk, abdomen, and extremities.
Case presentation: Here we present a 84-year-old man with multiple Bullous hemorrhagic dermatosis on the neck, abdomen, and extremities after subcutaneous injection of enoxaparin. It is a rare presentation of a rare adverse effect of low molecular weight heparin.
Conclusions: Bullous hemorrhagic dermatosis is a rare and benign adverse effect of heparin and LMWH that can occur mostly on extremities followed by the abdomen, trunk, and rarely head and neck after 5-12 days of treatment. Doctors should be acquainted with this condition’s dermatologic picture and reassure the patients about it since it mostly follows a benign course.
Keywords: Enoxaparin; Low molecular weight heparin; Bullous hemorrhagic dermatosis.
Abbreviations: LMWH: Low Molecular Weight Heparin.
Citation: Hassani AH, Hooshanginezhad Z, Rezaei M, Azizi F, et al. Enoxaparin-induced bullous hemorrhagic dermatosis adjacent to and distant from the injection site: A case report. J Clin Images Med Case Rep. 2022; 3(11): 2148.
Background
Enoxaparin is Low Molecular Weight Heparin (LMWH), widely used as an anticoagulant factor inhibiting Xa and IIa factors in the hemostasis cascade [1]. Enoxaparin is used to prevent and treat venous thromboembolism and treat ischemic heart disease [2]. Subcutaneous administration of heparin molecules such as Enoxaparin has been associated with multiple dermatologic adverse reactions such as hypersensitivity reactions, skin necrosis, and indurated erythematous lesions with central eschar due to intradermal microvascular thrombosis following heparin-induced thrombocytopenia [3].
Bullous hemorrhagic dermatosis is a rare subcutaneous heparin and LMWH administration sideeffect that mainly develops within 5-21 days of treatment and mostly follows a benign course. This complication was reported as either generalized or localized and usually is seen in sites distant from the injection site. It is mostly happening in the extremities, followed by the trunk and abdomen, and is very rare on the head and neck. Our reported case had lesions on the neck, abdomen, and extremities [4,5].
This condition is believed to be self-limited; however, since it sometimes has a frightening appearance, physicians must be aware of the complication to reassure the patients [6]. So far, most of the case reports have depicted this complication on extremities; however, in our patient, this enoxaparin-induced bullous hemorrhagic dermatosis was found on the forehead, neck, abdomen, and trunk in places adjacent to and distant from the injection site and on abdominal fat.
Case presentation
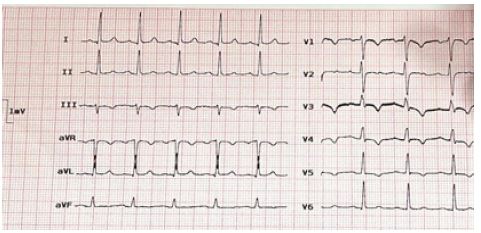
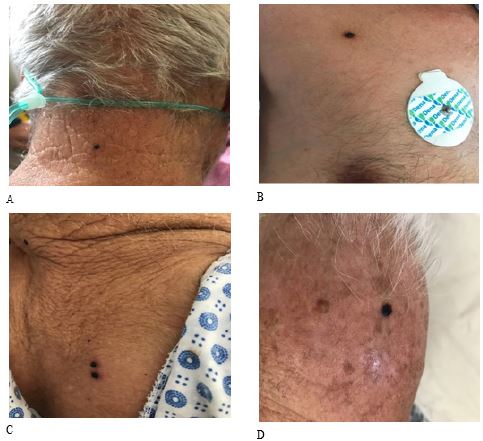
The patient was an 84-years old gentleman with a history of systemic hypertension who came to our emergency department with a chief complaint of typical chest pain. He had been receiving losartan 25 mg twice a day. The patient was admitted with a Non-ST segment elevation myocardial infarction diagnosis due to his positive Troponin and ST-coving and T-wave inversion in his electrocardiogram (Figure 1). During his course of hospitalization, he was started on ASA, Clopidogrel, and therapeutic enoxaparin (60 mg twice daily, in the periumbilical region) for five days. On the fifth day of admission, he developed multiple asymptomatic lesions on the forehead, neck, chest wall, and abdomen (Figure 2) and a single tense hemorrhagic bullous on the periumbilical area near the injection site (Figure 3).
Laboratory tests, including complete blood cell count and biochemical and coagulation panel (activated partial thromboplastin time, prothrombin time, international normalized ratio) and liver function test and serum electrolytes have been checked and were within normal range. Biopsy wasn’t performed due to the typical clinical appearance of lesions, and the patient was diagnosed with bullous hemorrhagic dermatosis induced by enoxaparin.
No abnormal bleeding was seen in the patient, and the physical examination of his mucous membranes was normal.
Enoxaparin was discontinued for the patient, lesions continued to resolve, and after three weeks, no sign of enoxaparin-induced bullous hemorrhagic dermatosis was found on the patient’s body. This was a relatively rare case in which enoxaparin-induced bullous hemorrhagic dermatosis is seen on the trunk of a patient both adjacent to and distant from the injection site of Enoxaparin.
Discussion
In this article, we reported a case of enoxaparin-induced bullous hemorrhagic dermatosis in places adjacent to and distant from the injection site. Bullous hemorrhagic dermatosis is a rare complication of various heparin molecules first described by Perrinaud et al [7]. They reported this condition in three patients, two of whom received low molecular weight heparin (Dalteparin and Tinzaparin), while the other received heparin calcium. All of the dermatological lesions appeared distant from the injection site. The treatment was continued in the patient receiving heparin calcium, and the lesions were resolved spontaneously. The treatment was discontinued in the patient receiving Tinzaparin, and the lesion disappeared within ten days. The other patient expired due to cerebral hemorrhage, possibly consequent of Vitamin K antagonist overdose.
Less than thirty enoxaparin-induced bullous hemorrhagic dermatosis cases have been previously reported [8,9]. The patients ranged from 38 to 90 years old. In the cases who stayed alive after treatment of their underlying disease, the bullous hemorrhagic dermatosis resolved regardless of the continuation or discontinuation of enoxaparin. Pathologic investigation can confirm the diagnosis by ruling out other entities. Although skin biopsy was not performed in our study, previous literature has shown that the bulla is intraepidermal and subcorneal [5]. No significant change was detected in complete blood counts, coagulation panels, liver function tests, or serum electrolytes in the reported cases. In our case, no significant difference was seen in the laboratory results either.
The underlying pathogenesis of heparin-induced bullous hemorrhagic dermatosis is yet to be found. Multiple hypotheses are postulated in this regard. Gonzalez et al. and Thuillier et al. found eosinophilic infiltration in the dermis underneath the bulla and proposed hypersensitivity reactions as a possible mechanism for bullous hemorrhagic dermatosis formation [10,11]. Anticoagulant overdose and idiosyncratic reactions are the other possible etiologies [12,13]. In the previous literature, no vasculitis feature was seen in pathology specimens.
Regarding managing heparin-induced bullous hemorrhagic dermatosis, the lesions can resolve despite the continuation or discontinuation of heparin therapy; however, the evidence on this matter is not enough to draw a wholesome conclusion. Consequently, the decision to continue or discontinue heparin or LMWH should be individualized.
Conclusion
Bullous hemorrhagic dermatosis is a rare and benign adverse effect of heparin and LMWH that can occur mostly on extremities followed by the abdomen, trunk, and rarely head and neck after 5-12 days of treatment. Doctors should be acquainted with this condition’s dermatologic picture and reassure the patients about it since it mostly follows a benign course. Management of this adverse effect should be an individualized decision since further research is needed to have a generalizable conclusion regarding the treatment of this condition.
Declarations
Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shiraz University of Medical Sciences, Iran. Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.
Consent to publication: Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.
Availability of data and material: The data presented in this study are available on request from the corresponding author.
Competing interest: The authors declare no conflict of interest.
Funding: This research received no external funding.
Author contributions:
1. Amir Hossein Hassani: investigation, resources, writing case report, review, editing
2. Zahra Hooshanginezhad: validation, investigation, review, and editing.
3. Mojtaba Rezaei: Collecting data, investigation, review.
4. Fatemeh Azizi: Collecting data, investigation, resources, writing case report, review, editing, supervision.
All authors have read and agreed to the published version of the manuscript
Acknowledgments: We sincerely appreciate the participation of the patient in the current research.
References
- SW, et al. Pharmacodynamic and pharmacokinetic properties of enoxaparin: Implications for clinical practice. Clin Pharmacokinet. 2003; 42: 1043-1057.
- Hofmann T. Clinical application of enoxaparin. Expert Rev Cardiovasc Ther. 2004; 2: 321-337.
- Schindewolf M, Lindhoff Last E, Ludwig RJ, Boehncke WH. Heparin-induced skin lesions. Lancet. 2012; 380: 1867-1879.
- Al-Mashdali AF, Yassin MA. Enoxaparin-induced bullous hemorrhagic dermatosis at a distant location from the injection site. Clin Case Rep. 2021; 9: e05014.
- Frizzell MR, Nguyen NM, Goldberg LH, Parikh SA, Sinai MJ, et al. Heparin-induced bullous hemorrhagic dermatosis: A report of 3 cases. JAAD Case Rep. 2020; 6: 1065-1068.
- Villanueva CA, Nájera L, Espinosa P, Borbujo J. Bullous hemorrhagic dermatosis at distant sites: a report of 2 new cases due to enoxaparin injection and a review of the literature. Actas Dermosifiliogr. 2012; 103: 816-819.
- Perrinaud A, Jacobi D, Machet MC, Grodet C, Gruel Y, Machet L, et al. Bullous hemorrhagic dermatosis occurring at sites distant from subcutaneous injections of heparin: three cases. J Am Acad Dermatol. 2006; 54: S5-S7.
- Gouveia AI, Lopes L, Soares-Almeida L, Filipe P. Bullous hemorrhagic dermatosis induced by enoxaparin. Cutan Ocul Toxicol. 2016; 35: 160-162.
- Russo A, Curtis S, Balbuena-Merle R, Wadia R, Wong E, Chao HH, et al. Bullous hemorrhagic dermatosis is an under-recognized side effect of full dose low-molecular weight heparin: A case report and review of the literature. Exp Hematol Oncol. 2018; 7: 15.
- Gonzales UP, Scott GA, Briones AJ, Pentland AP, et al. Remote hemorrhagic bullae occurring in a patient treated with subcutaneous heparin. Arch Dermatol. 2009; 145: 604-605.
- Thuillier D, Chaby G, Dadban A, Dascotte E, Miquel-Christophe O, Andrejak M, et al. [Low-molecular-weight heparin-induced bullous haemorrhagic dermatosis associated with cell-mediated hypersensitivity]. Ann Dermatol Venereol. 2009; 136: 705-708.
- Snow SC, Pearson DR, Fathi R, Alkousakis T, Winslow CY, Golitz L, et al. Heparin-induced haemorrhagic bullous dermatosis. Clin Exp Dermatol. 2018; 43: 393-398.
- Gargallo V, Romero FT, Rodríguez-Peralto JL, Zarco C, et al. Heparin induced bullous hemorrhagic dermatosis at a site distant from the injection. A report of five cases. An Bras Dermatol. 2016; 91: 857-859.