
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case report on the abscopal effect of liver-directed GRID radiotherapy
Li Tianpei; Ashley Ong Li Kuan; Ang Khong Wei; Eric Pang Pei Ping; Wang Fuqiang*
Division of Radiation Oncology, National Cancer Centre Singapore 169610, Singapore.
*Corresponding Author : Wang Fuqiang
Division of Radiation Oncology, National Cancer
Centre Singapore, 11 Hospital Cres, Singapore
169610.
Email: wang.fu.qiang@singhealth.com.sg
Received : Sep 19, 2022
Accepted : Nov 16, 2022
Published : Nov 23, 2022
Archived : www.jcimcr.org
Copyright : © F Wang (2022).
Abstract
GRID radiotherapy is a form of spatially fractionated radiotherapy that allows delivery of high radiation doses to bulky tumours. A grid splits the beam into multiple beamlets to give a heterogenous dose to the tumour, while stimulating the immune system to improve tumour response through the abscopal effect. However, this has fallen out of favour in recent times due to the presence of more modern techniques. Here we present a case of a large liver metastasis from a rectal neuroendocrine primary treated with GRID radiotherapy with an abscopal response seen in a portal vein tumour thrombus.
Citation: T Li, ALK Ong, KW Ang, EPP Pang, F Wang. A case report on the abscopal effect of liver-directed GRID radiotherapy. J Clin Images Med Case Rep. 2022; 3(11): 2168.
Introduction
Radiation oncologists have traditionally found it challenging to irradiate large, bulky tumours adequately whilst respecting normal tissue dose constraints. One technique that could circumvent such constraints is Spatially Fractionated Radiation Therapy (SFRT).
SFRT has a history dating back to the early 1900s [1], when it was known as GRID radiotherapy (GRID RT) that delivered highdose orthovoltage radiation [2] through a radio-dense block containing evenly spaced apertures arranged in a “grid” pattern [3]. This achieves spatial fractionation by filtering the beam to form multiple parallel pencil beamlets. The use of GRID RT has been adopted in the modern era with the use of modern machines for treatment of bulky disease, both with palliative [4-6] and with curative intent [4,7,8]. However, the use of GRID RT is limited to few centres worldwide, mainly due to the introduction of megavoltage linear accelerators and its concurrent reduction in skin toxicity, as well as the advent of stereotactic body radiotherapy (SBRT) [9].
Whilst the literature is abound with cases treated with GRID RT, with some showing dramatic responses in tumour size [10,11], there has not been a case of abscopal response seen with GRID RT alone. We hereby present a case report of a patient with metastatic rectal neuroendocrine tumour who received GRID RT to a large liver metastasis and demonstrated response in an unirradiated portal vein tumour thrombus (PVTT).
Case discussion
Patient demographic and medical history
The patient was a 48 year old Chinese gentleman who was diagnosed in September 2017 with rectal well-differentiated neuroendocrine tumour (RNET) with extensive liver metastases. He was treated initially with subcutaneous Octreotide from September 2017 till August 2018 when the metastatic liver disease progressed. He subsequently underwent Yttrium-90 selective internal radiation therapy (Y90 SIRT) to his right liver metastasis for pain in October 2018. There was stable disease post Y90 SIRT. However, there is disease progression with the development of portal vein tumour thrombosis (PVTT) in November 2018. Consequently, he was recommended for Lutetium-177 DOTATATE peptide receptor radionuclide therapy (PRRT) and received 4 sessions between January and December 2019 with overall stable disease. He was treatment free until October 2020 when restaging computed tomography (CT) scans showed disease progression in the PVTT. By then, the PVTT had extended from the right and left portal vein to the superior mesenteric vein. The liver metastases in the liver were stable with a dominant 21.3 cm right liver lobe mass with central necrosis. Clinically, the patient complained of increased right hypochondrium pain despite his radiological stability of liver metastases. His case was discussed at the Neuroendocrine tumour board and though everolimus was possible, the decision was made not to pursue it in view of the poor response rate at 2-20% [12-14]. In consideration that repeat Y90-SIRT would result in excessive radiation dose to normal liver, SBRT was suggested as an alternative and thus he was referred to our Division of Radiation Oncology in December 2020 for consideration of further management.
When reviewed at our clinic, besides the abdominal pain, the patient was also bothered by early satiety. SBRT was not feasible as the liver metastasis was too large. The lack of radiological response to prior internal radiation therapy (1 session of Y-90 SIRT and 4 sessions of PRRT) suggested the disease is likely radioresistant and may not respond to conventionally fractionated external beam radiotherapy. Furthermore, there was a possible risk of radiation-induced liver disease (RILD) given prior normal liver irradiation from previous internal radiation therapy. This was discussed with the patient. However, given the lack of effective therapeutic options, we offered the patient a short course of external beam radiotherapy (EBRT). The patient was keen to proceed with treatment.
Due to the multiple complexities surrounding the patient’s care, his case was discussed at our institution’s palliative radiation oncology audit meeting. At that juncture, our institution had just commissioned applicator-based GRID RT. The 25 cm by 25 cm GRID applicator, manufactured by .decima LLC (Sanford, FL, USA), is essentially made out of brass [2] with evenly spaced apertures arranged in a hexagonal array manner. Each aperture transmits a beam of diameter 1.4 cm, with a centre to centre distance of 2 cm, when measured at a source-skin distance (SSD) of 100 cm. As part of the implementation protocol, suitable patients can be treated with GRID RT if they fulfil the following clinical criteria: tumours >10 cm, previously irradiated, estimated prognosis more than 6 months, lack of effective alternative treatment options and with symptoms that is unmanageable by usual palliative measures. Our patient was deemed suitable for GRID RT and was thus offered this treatment in addition to EBRT.
Pre-treatment preparation
In terms of treatment planning, the patient was simulated as per our departmental protocol with a four-dimensional computed tomography (4D-CT) to take into account patient’s respiratory motion. The treatment plan was generated with reference to the work by Neuner et al [11], where the internal target volume (ITV) of the right liver lobe metastasis was identified as the target volume for GRID RT with no volumetric expansion added to it. Given the size and location of the tumour, it naturally displaced the adjacent small bowels. A beam angle of 350 degrees was selected as this optimised a direct beam path from the skin to the tumour whilst minimising normal liver irradiation. Using the beam’s eye view, multi-leaf collimators (MLC) were manually adjusted to close off beamlets to minimise exit doses to adjacent bowels. This meant the MLC shielded part of the GTV but was deemed necessary from the dosimetric safety point of view. Despite this, the eventual field size was still large at 14.2 cm by 14.3 cm, with a total of 43 beamlets delivering radiation. A nominal dose of 15 Gy was prescribed for GRID RT.
Doses to OAR were minimal: mean normal liver dose (i.e. the total liver volume minus ITV) was 1.3 Gy and the planning volumes of OAR (mainly bowels) received maximum doses ranging from 0.3-1.5 Gy. As a result, we could plan for a higher dose allowance to the OARs in the subsequent EBRT where we planned to deliver 30 Gy in 10 daily fractions. All treatment planning and calculations were done on the Eclipse Treatment Planning System Version 13.6, using AAA dose calculation algorithm (Varian Medical System, Palo Alto, USA).
Treatment delivery and outcomes
On the day of the GRID RT on 11 January 2021, the patient was set up as simulated and onboard cone-beam computed tomography (CBCT) images were acquired to verify position. After which, the GRID applicator was mounted on the gantry and the treatment delivered as planned. Besides the usual departmental radiotherapy delivery protocol, we also verified the SSD of 100 cm and verified the number and pattern of open holes through which GRID RT was eventually delivered uneventfully.
Unfortunately, 1 week after GRID RT, on 18 January 2021, the patient presented to the clinic with worsening right hypochondrium pain. To rule out tumour rupture, an urgent CT scan of his abdomen was done the following day. This showed stability in the right liver lobe mass with no rupture but the PVTT was extending further into the superior mesenteric vein. We managed to control his pain conservatively but the patient declined to continue with the planned EBRT.
At 2 months following GRID RT, the patient reported improvements in pain such that he stopped taking regular analgesia. He also reported improved appetite and oral intake. On examining his abdomen, there was a faint erythematous grid pattern observed on the skin where the beamlets entered, whilst a significantly more hyperpigmented grid pattern was observed posteriorly which corresponded to the exiting beamlets. We discussed about pursuing further treatment with the patient, but he declined as he was already satisfied with the symptomatic relief so far.
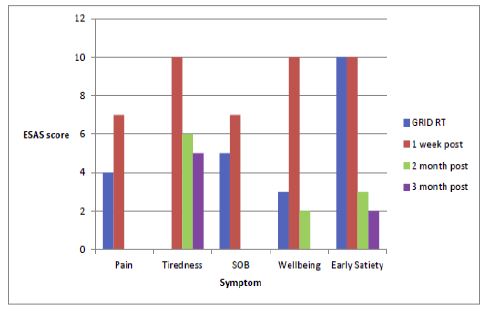
Repeat CT scan at 3 months post GRID RT showed stability of the liver metastases. However, unexpectedly, there was partial response in the PVTT. At the last re-staging scan at 6 months post GRID RT, there was further reduction seen in the PVTT despite no further treatment (radiotherapy, systemic therapy or anti-coagulation). Figure 1 illustrates the trend of symptoms on the day of GRID RT and at 1-month, 3-months and 6-months post GRID RT.
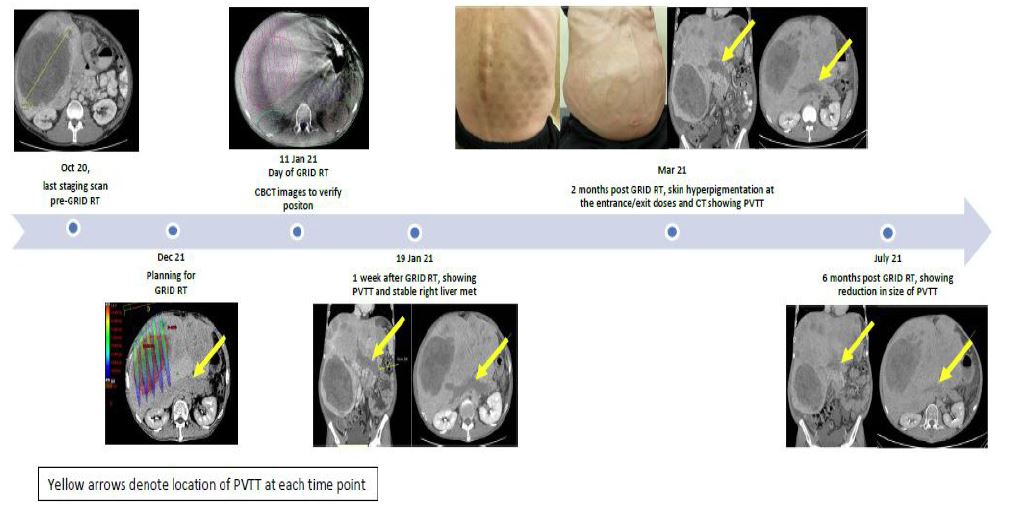
About 8 months on from GRID RT, the patient’s liver function subsequently deteriorated with the development of recurrent ascites requiring drainage. The cause of the ascites was attributed to liver failure from the liver metastases themselves rather than GRID RT, as the mean normal liver dose was only 1.3 Gy in 1 fraction. Further re-staging scans were not performed as the patient declined further treatment and opted for supportive care. His performance status worsened over time and was hospitalized repeatedly for complications of liver failure (recurrent ascites, scrotal swelling and pedal oedema from the loss of synthetic function of the liver). He passed away in December 2021, approximately 1 year post GRID RT. Timeline showing images and treatment related events are illustrated in Figure 2.
Discussion
Given the rarity of neuroendocrine tumours, especially one with massive liver metastases, our patient likely represented the first use of GRID RT in this scenario. In the literature, GRID RT has been applied across a variety of cancer types in the palliative setting [15] with a response rate of 76-100% [15] and with an acceptable toxicity profile. Sarcoma and head and neck carcinoma remain two of the more commonly treated cancer subtypes [3,6,8]. Regarding application of GRID RT to the liver, Mohiuddin et al [16] reported treating 3 patients with hepatocellular carcinoma out of a group of 22 patients. These patients had diverse pathology and had exhausted conventional chemotherapy and radiotherapy options. Similarly, Neuner et al reported treating 6 patients (out of 79 patients) with primary liver cancer with GRID RT. These studies had established the basis of the feasibility and safety profile of liver directed GRID RT and our patient was offered GRID RT on a compassionate basis.
In terms of treatment toxicity, our patient sustained mild skin reactions despite the high nominal dose prescribed. Mohiuddin et al [42] had described in their report of a patient with massive hepatomegaly treated with 2 opposing GRID fields of 30 cm x 15 cm, who developed skin erythema within 15 minutes of treatment which self-subsided in 4 hours. Our patient had a single GRID RT field of 14 cm by 14 cm and with more noticeable skin changes at the exit site at 1-month post GRID RT that subsequently subsided at 2 months. Whilst there was initial worsening of his abdominal symptoms, these resolved satisfactorily with time.
Though the mechanism underlying the efficacy of GRID RT is better expounded on in other reviews [1], it may be attributed to three possible effects: direct, bystander and abscopal.
The direct effect of GRID RT is likely the result of high dose radiation causing vascular damage and resultant tumour cell death from starvation. The bystander effect refers to the radiobiological effects on tumour cells in the low-dose region next to the high-dose ones [1], whereby the degree of cell kill in the low dose regions are higher than expected as compared to cells given low-dose radiation alone [1]. However, admittedly, in our patient, there was no radiological response in the treated liver metastasis to suggest the direct and bystander effects. This could be due to two possible reasons. Firstly, the tumour movement during treatment likely led to the “smearing” of doses delivered by the beamlets, which negates the high dose-low dose differentiation required for the bystander effect. Motion management methods were not employed for this patient as the movement on 4D-CT was less than 1 cm, and the patient was unable to tolerate breath-holding. Secondly, EBRT following GRID RT was not delivered. Previous studies have shown [7,17] enhanced tumour response when GRID RT is followed by fractionated EBRT.
Interestingly, the abscopal effect was observed in the PVTT post GRID RT in our patient. The abscopal effect describes tumour response outside of the intended radiation field [18]; in essence, a systemic effect of radiation [19]. This is largely attributed to immune system activation induced by radiotherapy [18]. On retrospective review of our treatment plan, we verified that the PVTT was not exposed to radiation from the GRID RT. Furthermore, he did not receive any systemic therapy or anticoagulation. The earliest scan at 1-week following GRID RT did not show any change in PVTT, but the subsequent scans at 3 and 6 months post GRID RT demonstrated gradual reduction in the PVTT. In his study, Grimaldi et al [20] reported the time to abscopal effect to range from 1 to 4 months. Thus, it is quite possible that we are observing the abscopal effect in the PVTT.
PVTT associated with neuroendocrine tumours have been reported mostly in pancreatic neuroendocrine tumours (PNET) [21,22]. In the context of HCC, PVTT may be seen in 35-50% of patients [23] and is associated with a short median survival of 2.7-4.0 months [24] if left untreated. Besides its status as a poor prognostic indicator, PVTT also adversely affects the hepatic vasculature, leading to portal hypertension [25] and associated downstream effects such as splenomegaly and variceal formation [23]. As our patient decided not to pursue further treatment, there was no repeat serial imaging beyond 6 months post GRID RT. The durability of response in the PVTT is hence unknown, though our patient did manage to survive almost 1-year post GRID RT. Thus, we postulate that as a result of this unexpected abscopal response in the PVTT, GRID RT has contributed meaningfully to our patient’s prolonged survival.
A potential criticism of this case could be our centre’s adoption of applicator-based GRID RT for the treatment of patients in a similar situation as the patient described in this report. Indeed, technological advances in the delivery of radiotherapy have allowed the development of other techniques of SFRT, including VMAT (Volumetric Arc Therapy)-GRID, lattice radiotherapy and proton GRID [1]. They all employ the same principle of delivering a heterogeneous high dose to a bulky tumour whilst respecting OAR dose constraints. There is also the exciting potential of combination therapy with immunotherapy [26]. However, at our centre, we believe that applicator-based GRID RT has its place as it requires minimal planning and is easy to deliver whilst being relatively economical. As a static irradiation, it is also less susceptible than other techniques to uncertainties such as tumour and MLC (and/or other mechanical) motion interplay. Furthermore, as exemplified in this case, there is a potential for clinical benefit despite the relative simplicity of treatment.
Conclusion
There remains to be a dearth of experience with GRID RT. This case helps to add to the literature regarding this radiotherapy technique and highlights the possible responses that could be elicited beyond conventional fractionated treatment.
References
- W. Yan, M. K. Khan, X. Wu, C. B. Simone, 2nd, J. Fan, E. Gressen, et al., “Spatially fractionated radiation therapy: History, present and the future,” Clinical and translational radiation oncology, vol. 20, pp. 30-38, 2019.
- C. Buckey, S. Stathakis, K. Cashon, A. Gutierrez, C. Esquivel, C. Shi, et al., “Evaluation of a commercially-available block for spatially fractionated radiation therapy,” J Appl Clin Med Phys, vol. 11, p. 3163, Apr 26 2010.
- J. L. Huhn, W. F. Regine, J. P. Valentino, A. S. Meigooni, M. Kudrimoti, and M. Mohiuddin, “Spatially Fractionated GRID Radiation Treatment of Advanced Neck Disease Associated with Head and Neck Cancer,” Technology in Cancer Research & Treatment, vol. 5, pp. 607-612, 2006/12/01 2006.
- M. Mohiuddin, M. Fujita, W. F. Regine, A. S. Megooni, G. S. Ibbott, and M. M. Ahmed, “High-dose spatially-fractionated radiation (GRID): a new paradigm in the management of advanced cancers,” Int J Radiat Oncol Biol Phys, vol. 45, pp. 721-7, Oct 1 1999.
- M. Mohiuddin, J. H. Stevens, J. E. Reiff, M. S. Huq, and N. Suntharalingam, “Spatially fractionated (GRID) radiation for palliative treatment of advanced cancer,” Radiation Oncology Investigations, vol. 4, pp. 41-47, 1996.
- M. Mohiuddin, T. Miller, P. Ronjon, and U. Malik, “Spatially Fractionated Grid Radiation (SFGRT): A Novel Approach in the Management of Recurrent and Unresectable Soft Tissue Sarcoma,” International Journal of Radiation Oncology, Biology, Physics, vol. 75, p. S526, 2009.
- J. A. Peñagarícano, E. G. Moros, V. Ratanatharathorn, Y. Yan, and P. Corry, “Evaluation of spatially fractionated radiotherapy (GRID) and definitive chemoradiotherapy with curative intent for locally advanced squamous cell carcinoma of the head and neck: initial response rates and toxicity,” Int J Radiat Oncol Biol Phys, vol. 76, pp. 1369-75, Apr 2010.
- J. M. Edwards, P. H. Shah, J. L. Huhn, W. St. Clair, W. F. Regine, M. Mohiuddin, et al., “Definitive GRID and Fractionated Radiation in Bulky Head and Neck Cancer Associated With Low Rates of Distant Metastasis,” International Journal of Radiation Oncology, Biology, Physics, vol. 93, p. E334, 2015.
- S. S. Poh, M. L. K. Chua, and J. T. S. Wee, “Why we should give spatially fractionated radiation therapy (GRID) a second look—especially in nasopharyngeal carcinoma,” Annals of Nasopharynx Cancer; Vol 2, No 4 (April 2018): Annals of Nasopharynx Cancer, 2018.
- A. Kaiser, M. M. Mohiuddin, and G. L. Jackson, “Dramatic response from neoadjuvant, spatially fractionated GRID radiotherapy (SFGRT) for large, high-grade extremity sarcoma,” Journal of Radiation Oncology, vol. 2, pp. 103-106, 2013/03/01 2013.
- G. Neuner, M. M. Mohiuddin, N. Vander Walde, O. Goloubeva, J. Ha, C. X. Yu, et al., “High-dose spatially fractionated GRID radiation therapy (SFGRT): a comparison of treatment outcomes with Cerrobend vs. MLC SFGRT,” Int J Radiat Oncol Biol Phys, vol. 82, pp. 1642-9, Apr 1 2012.
- J. C. Yao, M. H. Shah, T. Ito, C. L. Bohas, E. M. Wolin, E. Van Cutsem, et al., “Everolimus for Advanced Pancreatic Neuroendocrine Tumors,” New England Journal of Medicine, vol. 364, pp. 514-523, 2011.
- J. C. Yao, N. Fazio, S. Singh, R. Buzzoni, C. Carnaghi, E. Wolin, et al., “Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study,” The Lancet, vol. 387, pp. 968-977, 2016.
- M. H. Kulke, P. Ruszniewski, E. Van Cutsem, C. Lombard-Bohas, J. W. Valle, W. W. De Herder, et al., “A randomized, open-label, phase 2 study of everolimus in combination with pasireotide LAR or everolimus alone in advanced, well-differentiated, progressive pancreatic neuroendocrine tumors: COOPERATE-2 trial,” Ann Oncol, vol. 28, pp. 1309-1315, Jun 1 2017.
- C. Billena and A. J. Khan, “A Current Review of Spatial Fractionation: Back to the Future?,” International journal of radiation oncology, biology, physics, vol. 104, pp. 177-187, 2019.
- M. Mohiuddin, D. L. Curtis, W. T. Grizos, and L. Komarnicky, “Palliative treatment of advanced cancer using multiple nonconfluent pencil beam radiation. A pilot study,” Cancer, vol. 66, pp. 114-8, Jul 1 1990.
- A. Prasanna, M. M. Ahmed, M. Mohiuddin, and C. N. Coleman, “Exploiting sensitization windows of opportunity in hyper and hypo-fractionated radiation therapy,” Journal of thoracic disease, vol. 6, pp. 287-302, 2014.
- M. A. D’Andrea and G. K. Reddy, “Systemic Antitumor Effects and Abscopal Responses in Melanoma Patients Receiving Radiation Therapy,” Oncology, vol. 98, pp. 202-215, 2020.
- D. J. Craig, N. S. Nanavaty, M. Devanaboyina, L. Stanbery, D. Hamouda, G. Edelman, et al., “The abscopal effect of radiation therapy,” Future Oncology, vol. 17, pp. 1683-1694, 2021/05/01 2021.
- A. M. Grimaldi, E. Simeone, D. Giannarelli, P. Muto, S. Falivene, V. Borzillo, et al., “Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy,” Oncoimmunology, vol. 3, pp. e28780-e28780, 2014.
- A. Balachandran, E. P. Tamm, P. R. Bhosale, M. H. Katz, J. B. Fleming, J. C. Yao, et al., “Venous Tumor Thrombus in Nonfunctional Pancreatic Neuroendocrine Tumors,” American Journal of Roentgenology, vol. 199, pp. 602-608, 2012/09/01 2012.
- P. Addeo, A. d’Alessandro, G. Averous, A. Imperiale, F. Faitot, B. Goichot, et al., “Macrovascular venous invasion of pancreatic neuroendocrine tumours: impact on surgical outcomes and survival,” HPB, vol. 21, pp. 653-661, 2019/06/01/ 2019.
- L. Cerrito, B. E. Annicchiarico, R. Iezzi, A. Gasbarrini, M. Pompili, and F. R. Ponziani, “Treatment of hepatocellular carcinoma in patients with portal vein tumor thrombosis: Beyond the known frontiers,” World J Gastroenterol, vol. 25, pp. 4360-4382, Aug 21 2019.
- M. Minagawa and M. Makuuchi, “Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus,” World J Gastroenterol, vol. 12, pp. 7561-7, Dec 21 2006.
- M. Wu, M. Schuster, and M. Tadros, “Update on Management of Portal Vein Thrombosis and the Role of Novel Anticoagulants,” J Clin Transl Hepatol, vol. 7, pp. 154-164, Jun 28 2019.
- L. Jiang, X. Li, J. Zhang, W. Li, F. Dong, C. Chen, et al., “Combined High-Dose LATTICE Radiation Therapy and Immune Checkpoint Blockade for Advanced Bulky Tumors: The Concept and a Case Report,” Frontiers in Oncology, vol. 10, 2021-February-12 2021.