
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Rare case of metastatic secretary carcinoma presenting as an abscess
Daniel Holbrook; Brielle Paolini*; Brittany Dobson; Ian Smith; Rebecca J Leddy
Department of Radiology, Medical University of South Carolina, USA.
*Corresponding Author : Brielle M Paolini
Clinical Instructor, Department of Radiology, Medical University of South Carolina, Charleston, S.C, USA.
Email: paolinib@musc.edu
Received : Nov 15, 2022
Accepted : Dec 06, 2022
Published : Dec 13, 2022
Archived : www.jcimcr.org
Copyright : © Paolini BM (2022).
Abstract
Secretory Breast Carcinoma (SBC) is a rare and distinct type of breast cancer which accounts for less than 0.2% of all breast cancers. The modern breast imager should be aware of this rare entity as it can sometimes masquerade as a breast abscess as in the present case. This case underscores the importance of continued imaging follow up, biopsy and/or referral for surgical consultation in cases of chronic axillary masses including suspected abscesses regardless of pertinent history such as Hidra denitis Supprativa predisposing the patient to infection/inflammation. This case also emphasizes that the axillary mass differential in the setting of Hidradenitis Suppurativa importantly includes Squamous Cell Carcinoma or primary/metastatic breast cancer such as Secretory Carcinoma as presented.
Keywords: Breast cancer; Breast imaging; Radiology; Secretory carcinoma; Abscess.
Abbreviations: SBC: Secretory Breast Carcinoma; ETV6-NTRK3: ETV variant 6-neutrophic tyrosine kinase receptor type 3; TRK: Tropomyosin Receptor Kinase; HS: Hidradenitis Suppurativa; PMH: Past Medical History; U/S: Ultrasound; STEMI: ST Segment Elevation Myocardial Infarction; CT: Computed Tomography; CABG: Coronary Artery Bypass Graft; OR: Operating Room; PET/CT: Positron Emission Tomography/Computed Tomography; PAS: Periodic Acid-Schiff; FISH: Fluorescence in-situ hybridization.
Citation: Holbrook D, Paolini B, Dobson B, Smith I, Leddy RJ, et al. Rare case of metastatic secretory carcinoma presenting as an abscess. J Clin Images Med Case Rep. 2022; 3(12): 2196.
Introduction
Secretory Breast Carcinoma (SBC) is a rare and distinct type of breast cancer which accounts for less than 0.2 % of all breast cancers [1,6]. The modern breast imager should be aware of this rare entity as it can sometimes masquerade as a breast abscess as in the present case. This case is an example stressing the importance of imaging follow-up of a suspected abscess. SBC was originally described in children in 1966, but is now known to occur equally as frequently in adult populations [2,3,5]. It rarely metastasizes, but when it does will typically spread to the axillary lymph nodes with distal metastasis exceedingly rare [4,5]. There are fourteen reported cases in the literature of SBCs with distal metastatic lesions [5]. SBC has characteristic histopathologic and molecular features which include a characteristic gene fusion (ETV Variant 6-Neutrophic Tyrosine Kinase Receptor Type 3 (ETV6-NTRK3)) which is secondary to a balanced translocation, t(12;15) [5,6].
SBC is usually immune-profiled as a basal-like molecular subtype of breast cancer which is characterized by triple-negative receptor status (or weak ER expression) [6,7]. Despite basal-like cancers usually being the most aggressive subtype of breast cancer, SBC is slow growing and is associated with good long term survival [6]. There are only a total of eight cases of fatality due to metastatic Secretory Carcinoma [5]. Given the rarity and age range of patients, treatment is generally tailored to the patient’s symptoms and clinical characteristics with surgery the mainstay of treatment [5]. Since there are cases of late local recurrence (usually 10-12 years after diagnosis), many surgeons recommend simple mastectomy at a minimum [5]. Adjuvant radiation or chemotherapy have been considered but have not been overly successful [5]. Tropomyosin Receptor Kinase (TRK) inhibitors such as larotrectinib or entrectinib are a novel treatment strategy with NTRK fusion-positive cancer which have demonstrated excellent clinical response in the metastatic setting [6].
Case presentation
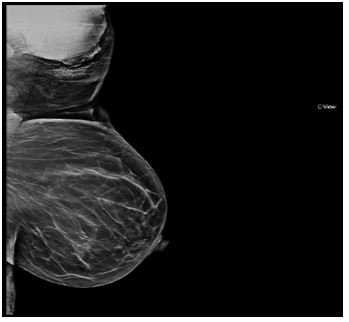
A 63-year-old African-American woman with a past medical history notable for Hidradenitis Suppurativa (HS) presented for a diagnostic mammogram and ultrasound with a 1-year history of a palpable, draining lump in her left axilla. Diagnostic mammogram demonstrated a high-density mass in the left axilla on the MLO view (Figure 1). Targeted ultrasound of the mass demonstrateda 5.4 cm vascular oval mass with circumscribed margins and heterogenous but predominantly hypoechoic echogenicity (Figure 2A and 2B). It was favored to likely represent an abscess in the setting of known HS versus a necrotic mass. The diagnostic mammogram and ultrasound recommended referral to breast surgery, consideration of ultrasound-guided or surgical biopsy, antibiotics, and follow-up ultrasound in 6-8 weeks. Additional note was made that if the biopsy was consistent with an infection then imaging and clinical follow up to resolution was recommended. The patient did seek surgical follow-up and underwent punch biopsy which was consistent with inflammation and abscess. She was placed on antibiotics and elective excision was planned.
Surgery was deferred due to recurrent episodes of hypertensive urgency and progressive coronary artery disease. She presented 8 months later for a ST Segment Elevation Myocardial Infarction (STEMI) and underwent non-contrasted chest CT for evaluation prior to Coronary Bypass Grafting (CABG). The CT demonstrated an ovoid 6.6 soft tissue mass containing gas in the soft tissues of the left upper chest wall/axilla with associated overlying skin thickening and adjacent axillary lymphadenopathy (Figure 2). These findings were again thought to represent abscess with associated reactive lymphadenopathy.
CT surgery requested infection control prior to cardiothoracic surgery and she was taken to the operating room for excision of the mass lesion and sinus tract. Pathology returned with a diagnosis of Secretory Carcinoma possibly from mammary primary extending from the axillary tail versus cutaneous primary. She was found to be NTRK positive which is characteristic of SBC.
The patient was referred to Oncology. Post-excisional mammogram, ultrasound and MRI showed left axillary lymphadenopathy with a differential of reactive lymph nodes due to Hidradenitis Supprative versus metastatic disease. Left axillary lymph node biopsy was recommended and performed without complication. Left axillary lymph node pathology was positive for metastatic disease.


The patient was deemed not a good surgical candidate due to multiple comorbidities placing her at high risk for surgical mortality and is currently being evaluated for initiation of radiation treatments with consideration of the tyrosine kinase inhibitor, Larotrectinib.
Discussion/conclusion
Secretory breast carcinoma of the breast is a rare and slow growing tumor [5]. Management can uncommonly be complicated by late local recurrence and axillary lymph node metastases [5]. Distant metastases are extremely rare [6]. It usually presents as a slow-growing, painless, well-circumscribed palpable mass [6]. It can occur anywhere within the breast but does demonstrate a predilection for the upper outer quadrant of the breast which can include axillary breast tissue [5]. From a histopathologic standpoint, it has been shown to be associated with a sold, microcystic and tubular structure microscopically with cells demonstrating abundant intracellular and extracellular secretory material which stains positive for Alcian blue or Periodic-Acid-Schiff staining (PAS) [5]. Fluorescence In-Situ Hybridization (FISH) analysis indicates the characteristic fusion translocation of t(12;15) of the ETV6-NTRK3 [5].
We present the case of a 63-year-old woman with past medical history of Hidradenitis Suppurative (HS) who had a chronic left axillary mass which was thought to be secondary to a chronic abscess in the setting of known HS. Surgical resection of this mass for infection control prior to CABG yielded pathology of Secretory Breast Carcinoma. Left axillary lymph nodes were positive for metastatic disease. She was deemed high risk for surgical management due to her comorbidities and is planned to initiate radiation therapy with consideration of Larotrectinib (a TK inhibitor).
This case underscores the importance of continued imaging follow up for breast masses thought to be secondary to chronic abscesses regardless of pertinent history such as Hidradenitis Supprativa predisposing the patient to infection/inflammation. The majority of cases of Secretory Carcinoma present as a breast mass; however, this case underwent delayed diagnosis due to an initially negative punch biopsy in the setting of Hidradenitis Suppurativa as well as lack of clinical follow-up imaging. Hidradenitis Suppurativa has an uncommon but known association with Squamous Cell Carcinoma due to chronic inflammation [8]. This case report highlights the importance of dedicated breast imaging including appropriate follow up, biopsy and/or referral for surgical consultation in cases of chronic axillary masses including suspected abscesses. This case also emphasizes that the axillary mass differential in the setting of Hidradenitis Suppurativaimportantly includes Squamous Cell Carcinoma or primary/metastatic breast cancer such as Secretory Carcinomaas presented.
Acknowledgements: None.
Conflicts of interest: None.
References
- Pohlodek K, Mečiarová I, Grossmann P, Martínek P, Kinkor Z, et al. Secretory carcinoma of the breast: A case report. Int J Surg Case Rep. 2019; 56: 74-77.
- Mc Divitt RW, Stewart FW. Breast Carcinoma in Children. JAMA. 1966; 195: 388–390.
- Horowitz DP, Sharma CS, Connolly E, Gidea-Addeo D and Deutsch I. Secretory carcinoma of the breast: Results from the survival, epidemiology and end results database. Breast. 2012; 21: 350–353.
- H Herz, B Cooke, D Goldstein. Metastatic secretory breast cancer. Non-responsiveness to chemotherapy: Case report and review of the literature. Ann of Onc. 2000; 11: 1343-1348.
- Tang H, Zhong L, Jiang H. Secretory carcinoma of the breast with multiple distant metastases in the brain and unfavorable prognosis: a case report and literature review. Diagn Pathol. 2021; 16: 56.
- Mortensen L, Ordulu Z, Dagogo Jack I, et al. Locally Recurrent Secretory Carcinoma of the Breast with NTRK3 Gene Fusion. Oncologist. 2021; 26: 818-824.
- Laé M, Fréneaux P, Sastre-Garau X. Secretory breast carcinomas with ETV6-NTRK3 fusion gene belong to the basal-like carcinoma spectrum. Mod Pathol. 2009; 22: 291-298.
- Constantinou C, Widom K, Desantis J, Obmann M. Hidradenitis suppurativa complicated by squamous cell carcinoma. Am Surg. 2008; 74: 1177-1181.
- Cocco E, Scaltriti M, Drilon A. NTRK fusion-positive cancers and TRK inhibitor therapy. Nat Rev Clin Oncol. 2018; 15: 731-747.
- Pareja F, Weigelt B, Reis-Filho, JS. Problematic breast tumors reassessed in light of novel molecular data. Mod Pathol. 2021; 34: 38–47.
- Lee SG, Jung SP, Lee HY. Secretory breast carcinoma: A report of three cases and a review of the literature. Oncol Lett. 2014; 8: 683-686.