
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Infant with large arachnoid cyst presented with repetitive vomiting after minor fall
Umma Kulthum Umar; Sarah Bin Hariz*; Ayesha Al Memari
Sheikh Shakhbout Medical City, Department of Emergency, Abu Dhabi, United Arab Emirates.
*Corresponding Author : Sarah Bin Hariz, MBBS
Emergency Medicine Specialist, Shaikh Shakhbout Medical City, Abu Dhabi, UAE.
Phone: 971557107656;
Email: binharizsarah@gmail.com;
smhariz@ssmc.ae;
ORCID ID: 0000-0001-8095-5496.
Received : Dec 14, 2022
Accepted : Jan 06, 2023
Published : Jan 13, 2023
Archived : www.jcimcr.org
Copyright : © Hariz SB (2023).
Citation: Umar UK, Hariz SB, Memari AA. Infant with large Arachnoid Cyst presented with repetitive vomiting after minor fall. J Clin Images Med Case Rep. 2023; 4(1): 2242.
Description
A 12-month-old boy, previously healthy, presented to our Emergency Department (ED) with 7 episodes non-bilious vomiting, parents gave history of mild head injury the night before. Clinical examination was unremarkable. According to pediatric Computerized Tomography (CT) head rule (PECARN) in less than 2 years old he would be low risk for intracranial pathology and would not require CT of the brain. However, CT scan was done based on clinical gestalt given history of repetitive vomiting since the fall.
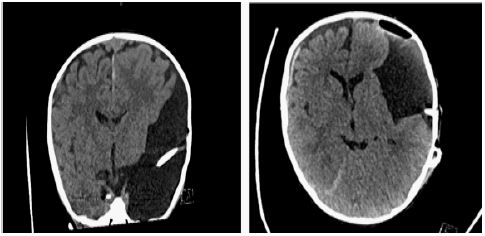
The CT scan showed a large left temporal Arachnoid Cyst (AC) with mass effect and shift of midline structures, which is an incidental finding, we wonder if the minor head injury had caused cyst rupture or intra-cyst bleed (Figure 1).
AC are clear benign cysts that arise from the arachnoid membrane within the brain and spinal cord. They contribute to about 1% of intracranial masses, with half of them forming within the middle cranial fossa. These cysts tend to occur in children and are more common in males [1]. Majority arise due to developmental anomalies [1,2]. The clinical presentation of these cysts depends on their size and location [1]. They are usually asymptomatic and often found incidentally [1-3]. When symptomatic, they can present with a wide range of symptoms like nausea, vomiting, headaches, ataxia, paraparesis and seizures [1-3]. AC are rarely associated with chronic subdural hemorrhage following head injury and it is very rare to develop intra-cystic bleeding spontaneously [1,3]. A CT scan is diagnostic; however, Magnetic Resonance Image (MRI) is helpful for evaluation of anatomic location, size and extent of adjacent structures involved. MRI can also differentiate between AC and epidermoid cysts, which is an important differential diagnosis [1-3]. Symptomatic cysts are treated surgically with craniotomy fenestration, endoscopic cyst fenestration or shunt placement. Small, non-symptomatic cysts are managed conservatively [1-3].

Declarations
Competing interests: None declared.
Consent: The authors have obtained patient consent.
References
- Hong JC, Kim MS, Chang CH, Kim SH. Arachnoid Cyst with Spontaneous Intracystic Hemorrhage and Chronic Subdural Hematoma. J Korean Neurosurg Soc. 2008; 43: 54–56.
- Arachnoid Cysts [Internet]. NORD (National Organization for Rare Disorders). [cited 2021 Nov 4]. Available from: https://rarediseases.org/rare-diseases/arachnoid-cysts/
- Petridis AK, Doukas A, Barth H, Mehdorn HM. Spinal cord compression caused by idiopathic intradural arachnoid cysts of the spine: review of the literature and illustrated case. Eur Spine J. 2010; 19: 124–129.