
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Evaluation of fetal cardiac anomalies and their outcomes in isolated cardiac anomalies and non-isolated groups and based on minor and major abnormalities
Behnaz Moradi1,2; Faramarz Shahriari Fard; Mohammad Hossein Golezar2*; Masoumeh Gity2; Fatemeh Rahimi Sharbaf3; Mohammad Nasir Hematian4; Fatemeh Golshahi4
1Department of Radiology, Yas Hospital Complex, Tehran University of Medical a Sciences, Tehran, Iran.
2Advanced Diagnostic and Interventional Radiology Research Center (ADIR), Medical Imaging Center, Tehran University of Medical Sciences, Tehran, Iran.
3Maternal, Fetal and Neonatal Research Center, Yas Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
4Department of Perinatology and Fetal Cardiology, Yas Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Mohammad Hossein Golezar
Advanced Diagnostic and Interventional Radiology Research Center (ADIR), Medical Imaging Center, Tehran University of Medical Sciences, Tehran, Iran.
Email: drgolezar@yahoo.com
Received : Jan 12, 2023
Accepted : Feb 07, 2023
Published : Feb 14, 2023
Archived : www.jcimcr.org
Copyright : © Golezar MH (2023).
Abstract
Background: This study was aimed to evaluate the characteristics and outcomes of isolated CHD and non-isolated CHD and also compare with major and minor cardiac anomalies.
Methods: This prospective observational study was performed on 135 cases of CHD from September 2018 to December 2021. Patients were prospectively evaluated for abortion, intrauterine death, death during or after delivery, and live birth. Finally, these variables were compared between the two groups of minor and major CHD, and also isolated and non-isolated CHD.
Results: Out of 135 patients, 54 (40.0%) had minor and 81 (60.0%) had major CHD. Also, 78 cases (57.8%) were isolated and 57 cases (42.2%) were non-isolated. The most common minor anomalies are TR (21 cases, 15.6%) and VSD (19 cases, 14.1%), and the most common major anomalies are AVSDs (22 cases, 16.3%). 14 cases (43.8%) of minor CHD and 6 major CHD cases (10.2%), resulted in a live birth (p-Value = 0.002). Also, 18 cases (36.0%) of isolated CHD and only 2 cases (4.9%) of non-isolated CHD resulted in live birth (p-Value = 0.002). The most common extracardiac accompanying anomalies were head, neck, and central nervous system abnormalities, which were seen in 36 cases (26.7%). Moreover, 84.6% of isolated minor CHD cases without hydrops and cystic hygroma survived.
Conclusions: Generally, the major cardiac anomalies and their association with extracardiac abnormalities reduce the likelihood of live birth. Those minor anomalies accompanied by hydrops and cystic hygroma have a poorer prognosis than isolated minor anomalies.
Keywords: Cardiac abnormality; Extracardiac abnormality; Fetal echocardiography; Anomaly scan.
Abbreviations: US: Ultrasound; MRI: Magnetic Resonance Imaging; CHD: Congenital Heart Disease; IUGR: Intra Uterine Growth Retard; TR: Tricuspid Regurgitation; VSD: Ventricular Septal Defects; LVH: Left Ventricular Hypertrophy; PS: Pulmonary Stenosis; AS: Aortic Stenosis; AVSD: Atrioventricular Septal Defect; Coa: Coarctation Of The Aorta; TOF: Tetralogy Of Fallot; TGA: Transposition Of The Great Arteries; HLHS: Hypoplastic Left Heart Syndrome; DORV: Double Outlet Right Ventricle; RV: Right Ventricle; MR: Mitral Regurgitation; PR: Pulmonary Regurgitation.
Citation: Moradi B, Fard FS, Golezar MH, Gity M, Sharbaf FR, et al. Evaluation of fetal cardiac anomalies and their outcomes in isolated cardiac anomalies and non-isolated groups and based on minor and major abnormalities. J Clin Images Med Case Rep. 2023; 4(2): 2284.
Introduction
Congenital Heart Disease (CHD) is the most common anomaly in the fetus, with the prevalence of cardiac abnormalities being 6 times higher than chromosomal abnormalities and 4 times more common than neural tube defects [1,2]. Estimates show that CHD has an incidence of 8 to 10 cases per 1000 births, about one-third of which are severe diseases. CHD is responsible for 20% of neonatal mortality and 40% of perinatal mortality [3].
Routine prenatal screening not only does lead to early detection of congenital heart disease but can also lead to the best postpartum treatment decisions, such as surgery or medical provision, or even a decision to terminate the pregnancy [4].
Most CHD diseases are structural and developmental cardiac problems that occur mainly during the prenatal period and are either inherited or due to environmental factors. The most common types of developmental or structural anomalies are Ventricular Septal Defect (VSD), Atrial Septal Defect (ASD), and Patent Ductus Arteriosus (PDA) [5].
CHD can lead to complications such as cardiac fraternity, preterm delivery, fetal or neonatal death, hemopericardium, or noncomplicated delivery. Any of these complications may be directly related to the type of cardiac anomaly that requires further evaluation [6].
CHD is frequently accompanied by major extra-cardiac malformations, and comprehensive screening for related abnormalities is required when a CHD is detected in pregnancy. Intuitively, the association of a CHD with other abnormalities may impact the parental decision to continue the pregnancy [7,8].
CHD are divided into two categories depending on their association with other congenital abnormalities: isolated and non-isolated CHD. Associated anomalies include genetic defects, non-chromosomal syndromes, and non-specific structural abnormalities. CHD are also divided into two groups based on the type of cardiac anomaly: minor and major. Cases such as isolated VSD, TR, mild to moderate PS, AS, and cardiomegaly are classified as minor anomalies, while AVSD, CoA, TOF and TGA are major anomalies [9].
The present study was aimed to evaluate the characteristics and outcomes of isolated and non-isolated CHD prospectiveliy and also to compare with major and minor cardiac anomalies, and to evaluate the types of extracardiac accompanying abnormalitiesand the final results of CHD pregnancies. We also studied isolated minor cases without hydrops and cystic hygroma to show the impact of these situations on pregnancy outcome.
Methods
Patients and data acquisition
This prospective observational multi-center study was designed based on the Helsinki declaration, and all the necessary information about the study was explained to the patients. This study was performed on 135 cases of CHD from September 2018 to December 2021. Among them, 78 cases were isolated CHD and 57 fetuses were non-isolated.They were also divided into two groups based on the type of cardiac anomaly: Minor [54] and major [81]. Also, fetuses with isolated minor CHD without hydrops and cystic hygroma were compared with another situation.
For inclusion in this study, the main criteria include the presence of a cardiac abnormality in fetuses during all trimesters. Exclusion criteria were patient dissatisfaction with study participation, more than 20% errors in the file information, and a lack of access to required information after birth.
Information required for the study, including maternal age, gestational age, maternal BMI before pregnancy, diabetes, hypertension, preeclampsia, history of CHD, consanguinity marriage, smoking, and alcohol consumption, was extracted from medical records. These parameters and sonographic information were compared in fetuses.
Moreover, the type and prevalence of major and minor CHD, and extra-cardiac associated anomalies were evaluated among fetuses. Also, in limited number of fetuses, chromosomal abnormalities information was available and their association with cardiac and extra-cardiac anomalies was investigated.
Ultrasound protocol
According to the new AIUM 2019 guideline, multiple fetal and maternal risk factors for the occurrence of all types of cardiac anomalies are mentioned as the criterion of this guideline in this study. Ultrasound evaluations were performed using the Philips ultrasound device (Affinity 70, Women imaging configuration, USA), using a 2–6 MHz curve probe with an echo option.
Sonographic information includes hydrops, cystic hygroma, NT > 3.5 mm and IUGR, and types of CHD and Non-CHD. Also, information about arterial-venous anomalies were assessed, including Aberrant Right Subclavian Artery (ARSA), Single Umbilical Artery (SUA), Double SVC, Ductus Venosus Agenesis (DVA), And Portal System Anomalies.
Postnatal assessment
Patients were followed up until the birth of the affected infants to evaluate preterm delivery and their pregnancy outcomes, including abortion, intrauterine death, death during or after delivery, and live birth.
Data analysis
The obtained data were entered into SPSS software version 25. Frequency and frequency percentages were used to describe qualitative data, and mean, and standard deviation was used to describe quantitative data. An independent T-test was used for the analytical analysis of quantitative data, and a Chi-squared test was used for qualitative data analysis. Finally, we used a logistic regression test to investigate the direct effect of each variable on pregnancy outcome. (P-value < 0.05 was considered statistically significant).
Results
The mean age of mothers in this study was 31.63 ± 6.60 years, and the mean gestational age was 18.68 ± 5.60 weeks. Out of 135 patients, 54 (40.0%) had minor CHD, and 81 (60.0%) had major CHD. Also, 78 cases (57.8%) were isolated and 57 cases (42.2%) were non-isolated CHD.
Table 1: Comparison of cases of major with minor cardiac anomalies, isolated with non-isolated CHD, isolated minor cardiac anomalies without hydrops and cystic hygroma with other cardiac anomalies.
| Variable | Cardiac anomalies | p-Value | Cardiac anomalies | p-Value | Cardiac anomalies | p-Value | Total (sum) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| minor without hydrops and cystic hygroma 25 (18.5%) | Other 110 (81.5%) | Minor 54 (40.0%) | Major 81 (60.0%) | Non isolated 57 (42.2%) | Isolated 78 (57.8%) | ||||||
| Maternal age (M ± SD) | 31.92 ± 5.84 | 31.56 ± 6.78 | 0.809 | 31.31 ± 6.66 | 31.85 ± 6.58 | 0.649 | 32.42 ± 6.75 | 30.55 ± 6.28 | 0.108 | 31.63 ± 6.60 | |
| GA (M ± SD) | 21.06 ± 5.57 | 18.12 ± 5.48 | 0.018 | 19.53 ± 5.97 | 18.09 ± 5.28 | 0.148 | 19.88 ± 5.98 | 17.08 ± 4.63 | 0.003 | 18.68 ± 5.60 | |
| BMIMaternal (M ± SD) | 26.44 ± 3.17 | 26.38 ± 5.29 | 0.956 | 26.33 ± 4.42 | 26.43 ± 5.32 | 0.908 | 26.54 ± 4.68 | 26.19 ± 5.34 | 0.686 | 26.39 ± 4.56 | |
| Pregnancy trimester | First (n, %) | 2 (8.0%) | 31 (28.2%) | 0.103 | 12 (22.2%) | 21 (25.9%) | 0.711 | 15 (19.2%) | 18 (31.6%) | 0.158 | 33 (24.4%) |
| Second (n, %) | 20 (80.0%) | 70 (63.6%) | 36 (66.7%) | 54 (66.7%) | 54 (69.2%) | 36 (63.2%) | 90 (66.7%) | ||||
| Third (n, %) | 3 (12.0%) | 9 (8.2%) | 6 (11.1%) | 6 (7.4%) | 9 (11.5%) | 3 (5.3%) | 12 (8.9%) | ||||
| Fetal sex | Male (n, %) | 15 (75.0%) | 41 (55.4%) | 0.113 | 24 (60.0%) | 32 (59.3%) | 0.942 | 37 (63.8%) | 19 (52.8%) | 0.290 | 38 (40.4%) |
| Female (n, %) | 5 (25.0%) | 33 (44.6%) | 16 (40%) | 22 (40.7%) | 21 (36.2%) | 17 (47.2%) | 56 (59.6%) | ||||
| Smoking | Yes (n, %) | 0 (0.0%) | 1 (0.9%) | 1.000 | 0 (0.0%) | 1 (1.3%) | 1.000 | 1 (1.3%) | 0 (0.0%) | 1.000 | 1 (0.8%) |
| No (n, %) | 24 (100.0%) | 108 (99.1%) | 53 (100.0%) | 79 (98.8%) | 76 (98.7%) | 56 (100.0%) | 132 (99.2%) | ||||
| Alcohol consumption | Yes (n, %) | 0 (0.0%) | 1 (0.9%) | 1.000 | 0 (0.0%) | 1 (1.3%) | 1.000 | 1 (1.3%) | 0 (0.0%) | 1.000 | 1 (0.8%) |
| No (n, %) | 24 (100.0%) | 108 (99.1%) | 53 (100.0%) | 79 (98.8%) | 76 (98.7%) | 56 (100.0%) | 132 (99.2%) | ||||
| Gestational diabetes | Yes (n, %) | 4 (16.0%) | 9 (8.3%) | 0.263 | 8 (14.8%) | 5 (6.3%) | 0.100 | 11 (14.1%) | 2 (3.6%) | 0.042 | 13 (9.7%) |
| No (n, %) | 21 (84.0%) | 100 (91.7%) | 46 (85.2%) | 75 (93.8%) | 67 (85.9%) | 54 (96.4%) | 121 (90.3%) | ||||
| Hypertension | Yes (n, %) | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) |
| No (n, %) | 25 (100.0%) | 109 (100.0%) | 54 (100.0%) | 80 (100.0%) | 78 (100.0%) | 56 (100.0%) | 134 (100.0%) | ||||
| Preeclampsia | Yes (n, %) | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) | 0 (0.0%) | 1.000 | 0 (0.0%) |
| No (n, %) | 21 (100.0%) | 90 (100.0%) | 49 (100.0%) | 62 (100.0%) | 62 (100.0%) | 49 (100.0%) | 111 (100.0%) | ||||
| Consanguineous marriage | Yes (n, %) | 3 (12.0%) | 24 (22.0%) | 0.260 | 12 (22.2%) | 15 (18.8%) | 0.623 | 12 (15.4%) | 15 (26.8%) | 0.105 | 27 (20.1%) |
| No (n, %) | 22 (88.0%) | 85 (78.0%) | 42 (77.8%) | 65 (81.3%) | 66 (84.6%) | 41 (73.2%) | 107 (79.9%) | ||||
| Family history | Yes (n, %) | 4 (17.4%) | 23 (22.1%) | 0.781 | 10 (19.6%) | 17 (22.4%) | 0.709 | 16 (22.2%) | 11 (20.0%) | 0.762 | 27 (21.3%) |
| No (n, %) | 19 (82.6%) | 81 (77.9%) | 41 (80.4%) | 59 (77.6%) | 56 (77.8%) | 44 (80.0%) | 100 (78.7%) | ||||
| NT | >3.5(n, %) | 3 (16.7%) | 28 (33.3%) | 0.163 | 13 (29.5%) | 18 (31.0%) | 0.976 | 17 (27.9%) | 14 (34.1%) | 0.499 | 31 (30.4%) |
| < 3.5(n, %) | 15 (83.3%) | 56 (66.7%) | 30 (69.8%) | 41 (69.5%) | 44 (72.1%) | 27 (65.9%) | 71 (69.6%) | ||||
| history IVF | Yes (n, %) | 4 (16.7%) | 5 (4.8%) | 0.063 | 6 (11.3%) | 3 (4.0%) | 0.161 | 7 (9.6%) | 2 (3.6%) | 0.298 | 9 (7.0%) |
| No (n, %) | 20 (83.3%) | 99 (95.2%) | 47 (88.7%) | 72 (96.0%) | 66 (90.4%) | 53 (96.4%) | 119 (93.0%) | ||||
| Cystic hygroma | Yes (n, %) | - | - | 0 (0.0%) | 5 (12.8%) | 0.073 | 4 (12.9%) | 1 (2.9%) | 0.179 | 5 (7.6%) | |
| No (n, %) | 27 (100.0%) | 34 (87.2%) | 27 (87.1%) | 34 (97.1%) | 61 (92.4%) | ||||||
| Hydrops | Yes (n, %) | - | - | 9 (16.7%) | 20 (24.7%) | 0.266 | 18 (23.1%) | 11 (19.3%) | 0.597 | 29 (21.5%) | |
| No (n, %) | 45 (83.3%) | 61 (75.3%) | 60 (76.9%) | 46 (80.7%) | 106 (78.5%) | ||||||
| IUGR | Yes (n, %) | 1 (4.0%) | 7 (6.4%) | 1.000 | 4 (7.4%) | 4 (4.9%) | 0.713 | 2 (2.6%) | 6 (10.5%) | 0.070 | 8 (5.9%) |
| No (n, %) | 24 (96.0%) | 103 (93.6%) | 50 (92.6%) | 77 (95.1%) | 76 (9.4%) | 51 (89.5%) | 127 (94.1%) | ||||
| Arterial-venous anomalies | Yes (n, %) | 1 (4.0%) | 25 (22.7%) | 0.046 | 3 (5.6%) | 23 (28.4%) | 0.001 | 15 (19.2%) | 11 (19.3%) | 0.992 | 26 (19.3%) |
| No (n, %) | 24 (96.0%) | 85 (77.3%) | 51 (94.4%) | 58 (71.6%) | 63 (80.8%) | 46 (80.7%) | 109 (80.7%) | ||||
| Pregnancy outcome | Abortion | 2 (15.4%) | 60 (76.9%) | < 0.001 | 17 (53.1%) | 45 (76.3%) | 0.002 | 26 (52.0%) | 36 (87.8%) | 0.002 | 62 (68.1%) |
| Intra uterine death | 0 (0.0%) | 6 (7.7%) | 1 (3.1%) | 5 (8.5%) | 4 (8.0%) | 2 (4.9%) | 6 (6.6%) | ||||
| Death during or after delivery | 0 (0.0%) | 3 (3.8%) | 0 (0.0%) | 3 (5.1%) | 2 (4.0%) | 1 (2.4%) | 3 (3.3%) | ||||
| Live birth | 11 (84.6%) | 9 (11.5%) | 14 (43.8%) | 6 (10.2%) | 18 (36.0%) | 2 (4.9%) | 20 (22.0%) | ||||
Comparison of major and minor, isolated and non-isolated CHD, and isolated minor CHD without hydrops and cystic hygroma and other cardiac anomalies
As shown in Table 1, patients with minor and major cardiac anomalies do not differ significantly in terms of maternal age, gestational age, and maternal body mass index. However, pregnancy outcomes were significantly different between patients with minor cardiac anomalies and major group. 3 cases (5.6%) of minor cardiac anomalies had an arterial-venous-associated malformation, while 23 patients with major cardiac anomalies (28.4%) had an arterial-venous-associated malformation (p-Value = 0.001). Also, 14 cases (43.8%) of minor cardiac anomalies led to live births, while in the group with major cardiac anomalies, only 6 cases (10.2%) resulted in a live birth (p-Value = 0.002).
Eleven mothers (14.3%) who had fetuses with isolated cardiac abnormalities, and two (3.6%) mothers who had fetuses with non-isolated CHD had diabetes (p-Value = 0.042). Also, 18 cases (36.0%) of isolated CHD eventually resulted in stillbirth, while in cases of non-isolated CHD, only 2 cases (4.9%) resulted in a live birth (p-Value = 0.002).
Fetuses with isolated minor CHD without hydrops and cystic hygroma had no intra-uterine death and death during or after delivery, and also had the lowest abortion and highest live birth compared to other groups, which indicates the importance of these two situations in prognosis.
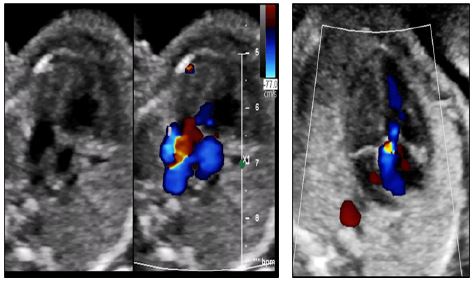
Table 2 shows that the most common minor anomalyis TR (21 cases, 15.6%), and the most common major anomalyis AVSD (22 cases, 16.3%). In Figure 1. A twin fetus with PS, PR, and TR is shown.
Types of extracardiac accompanying anomalies
The most common extracardiac accompanying anomalies were head, neck, and nervous system abnormalities, which were seen in 36 cases (26.7%). Gastrointestinal abnormalities (n: 21, 26.7%), limbs (n: 17, 12.6%), thoracic (n: 11, 8.1%), and genitourinary tract (n: 9, 6.7%) were the most common accompanying abnormalities, respectively, which have been studied in patients (Table 3).
Overall, 24 cases (42.1%) with minor cardiac anomalies and 33 patients (57.9%) with major cardiac anomalies had extracardiacaccompanying abnormalities, which is not statistically significant (p-Value = 0.670) (Table 2).
Pregnancy outcome and evaluation of affecting factors
According to Table 4, 11 cases (84.6%) of isolated minor without hydrops and cystic hygroma, 12 cases (66.7%) of patients with isolated minor cardiac anomalies, 2 cases (14.3%) of patients with non-isolated minor cardiac anomalies, and 6 cases (18.8%) of patients with isolated major cardiac anomalies had live births. In contrast, none of the patients with non-isolated major cardiac anomalies had live births, which was a statistically significant difference (p Value < 0.001).
Table 5, by performing logistic regression, we examined the effect of the studied variables on pregnancy outcome (live birth, abortion, intrauterine death, or during and after birth). As can be seen, the type of cardiac anomaly (minor or major) is independently related to the outcome of the pregnancy; the probability of a case with a minor cardiac anomaly leading to a live birth is 97.39 times higher than that of a major cardiac anomaly (p Value = 0.007).
Cases of chromosomal and genetic disorders
In total, out of 19 patients who underwent genetic and chromosomal testing and were aware of the test results, 13 were normal, and the characteristics of the 6 cases with chromosomal abnormalities are as follows in Table 6.
Discussion
The present study was designed and performed to compare isolated with non-isolated cardiac abnormalities and major with minor CHD prospectively and to evaluate the types of extracardiac-associated abnormalities, and outcomes of CHD pregnancies diagnosed on prenatal examination. Diagnosis and management of fetal cardiac anomalies before birth is critical because the leading cause of infant death is congenital anomalies, and CHD is the leading cause of neonatal death due to congenital anomalies [10]. In the United States, CHD is diagnosed in almost 1% of births and is the cause of 4% of neonatal mortality and 30% to 50% of congenital malformations [11,12].
In general, the proportion of live births in cases with minor cardiac abnormalities was higher compared to major cardiac abnormalities, and also, isolated cardiac abnormalities were higher than non-isolated cardiac abnormalities.
In the present study, we also divided patients into two groups with major and minor cardiac anomalies, most of which (60%) had major cardiac anomalies. Previous studies have reported a higher number of cases of complex and major cardiac anomalies than minor cases, which is in line with the results of our study [1,13,14]. However, in some studies that have also examined postpartum, the prevalence of minor anomalies has been reported to be higher [15].
Studies show that the best time to screen for fetal cardiac structural abnormalities is 18 to 22 weeks. As in previous studies, most cases of cardiac anomalies are diagnosed in the second trimester [15,16].
Various risk factors for fetal CHD have been identified [17]. For example, having a parent or sibling with CHD can increase the risk of a fetus developing the disease 3 to 4 times in the general population [18,19]. The present study examined the cases of CHD and the possible risk factors between the two groups with minor and major cardiac anomalies and between the groups with isolated and non-isolated cardiac anomalies.
Table 2: Types of cardiac abnormalities their association with extracardiac accompanying anomalies.
| Major/Minor | Type of cardiac anomaly | n (%) | Total | Accompanying anomaly | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Minor | TR | 21 (15.6%) | 54 (40%) | 6 (10.5%) | 15 (19.2%) |
| VSD | 19 (14.1%) | 12 (21.1%) | 7 (9.0%) | ||
| Cardiomegaly* | 4 (3.0%) | 0 (0.0%) | 4 (5.1%) | ||
| LVH | 2 (1.5%) | 0 (0.0%) | 2 (2.6%) | ||
| PS* | 2 (1.5%) | 2 (3.5%) | 0 (0.0%) | ||
| AS* | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| VSD+TR | 3 (2.2%) | 2 (3.5%) | 1 (1.3%) | ||
| TR+ Cardiomegaly | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) | ||
| VSD+PS | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) | ||
| Major | AVSD | 22 (16.3%) | 81 (60.0%) | 13 (22.8%) | 9 (11.5%) |
| CoA | 10 (7.4%) | 6 (10.5%) | 4 (5.1%) | ||
| TOF | 6 (4.4%) | 4 (7.0%) | 2 (2.6%) | ||
| TGA | 4 (3.0%) | 2 (3.5%) | 2 (2.6%) | ||
| Ebstein’s abnormality | 4 (3.0%) | 0 (0.0%) | 4 (5.1%) | ||
| HLHS | 2 (1.5%) | 0 (0.0%) | 2 (2.6%) | ||
| Ectopia cordis | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) | ||
| Common truncus | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| AVSD+CoA | 3 (2.2%) | 1 (1.8%) | 2 (2.6%) | ||
| DORV+AVSD | 3 (2.2%) | 1 (1.8%) | 2 (2.6%) | ||
| AVSD+TOF | 2 (1.5%) | 1 (1.8%) | 1 (1.3%) | ||
| VSD+CoA | 2 (1.5%) | 1 (1.8%) | 2 (2.6%) | ||
| DORV TGA type | 2 (1.5%) | 0 (0.0%) | 2 (2.6%) | ||
| pentalogy of cantrell+common truncus+ VSD | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| ASD+TGA+HLHS | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| VSD+commontruncus+Ectopia cordis | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| TR+dextroversion | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| DORV+TOF | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| TR+TS+PS | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| DORV+TR | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) | ||
| Hypoplastic RV+PS | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| TR+MR+PS+ Cardiomegaly | 1 (.7%) | 0 (0.0%) | 1 (1.3%) | ||
| HLHS+PR | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| TGA+VSD | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| DORV+PS | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) | ||
| VSD+TR+PR | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) | ||
| Other | 6 (4.2%) | 2 (2.6%) | 4 (5.2%) | ||
*Mild to Moderate
TR: Tricuspid regurgitation, VSD: Ventricular septal defects, LVH: Left ventricular hypertrophy, PS: Pulmonary stenosis, AS: Aortic stenosis, AVSD: Atrioventricular septal defect, CoA: Coarctation of the aorta, TOF: Tetralogy of Fallot, TGA: Transposition of the Great Arteries, HLHS: Hypoplastic left heart syndrome, DORV: Double outlet right ventricle, RV: Right ventricle, MR: Mitral regurgitation, PR: Pulmonary regurgitation
Table 3: Types of extracardiac accompanying anomalies in studied patients.
| Total | n (%) | Extracardiac accompanying anomaly | |
|---|---|---|---|
| 78 (57.8%) | 78 (57.8%) | No | |
| 57 (42.2%) | 36 (26.7%) | CNS and head and neck | Yes |
| 21 (15.6%) | Gastrointestinal system | ||
| 9 (6.7%) | Genitourinary system | ||
| 11 (8.1%) | Thoracic | ||
| 17 (12.6%) | Limbs | ||
Table 4: Pregnancy outcome by major and minor cardiac anomalies and extracardiac-associated anomalies..
| Pregnancy outcome | Fetal anomaly | p-Value | ||||
|---|---|---|---|---|---|---|
| Isolated minor without hydrops and cystic hygroma | Isolated minor | Non-isolated minor | Isolated major | Non-isolated major | ||
| Abortion | 2 (15.4%) | 6 (33.3%) | 11 (78.6%) | 20 (62.5%) | 25 (92.6%) | < 0.001 |
| Intra uterine death | 0 (0.0%) | 0 (0.0%) | 1 (7.1%) | 4 (12.5%) | 1 (3.7%) | |
| Death during or after delivery | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (6.3%) | 1 (3.7%) | |
| Live birth | 11 (84.6%) | 12 (66.7%) | 2 (14.3%) | 6 (18.8%) | 0 (0.0%) | |
Table 5: The effect of the evaluated variables on the outcome of pregnancy.
| Variable | p-Value | Exp(B) | 95% C.I.for EXP(B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Maternal age | 0.652 | 1.045 | 0.864 | 1.263 |
| Maternal BMI | 0.293 | 0.898 | 0.735 | 1.097 |
| Gestational diabetes | 0.333 | 0.142 | 0.003 | 7.435 |
| Consanguineous marriage | 0.633 | 2.057 | 0.107 | 39.638 |
| NT>3.5 mm | 0.900 | 1.215 | 0.059 | 25.073 |
| Family history of CHD | 0.528 | 2.624 | 0.131 | 52.488 |
| Hydrops | 0.055 | 74.199 | 0.905 | 6083.493 |
| IUGR | 0.289 | 5.877 | 0.222 | 155.407 |
| Accompanying anomaly | 0.054 | 18.688 | 0.952 | 367.031 |
| Cardiac anomaly (major/minor) | 0.007 | 97.391 | 3.523 | 2692.076 |
The only significant difference was the mothers’ having diabetes, which was higher in cases of isolated cardiac abnormalities than in cases with extracardiac accompanying abnormalities, for which there is no specific justification due to the lack of similar studies. Although accurate judgment in this regard requires further studies, the results of our study show that the risk factors that increase the risk of CHD are not significantly related to minor or major cardiac anomalies and extra cardiac accompanying anomalies.
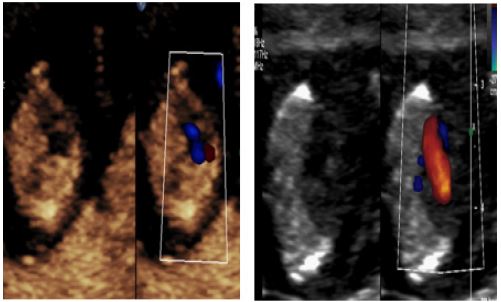
In this study, AVSD, TR, and VSD were the most common cardiac abnormalities, respectively. In Figure 3 and 4, two cases of VSD and AVSD are shown. In many previous studies, VSD and AVSD have also been reported as the most common cardiac anomalies [9,15].
Diagnosis of cardiac abnormalities in the fetus should be followed by extracardiac abnormalities in these cases as well as it has been found that at least 20% to 40% of cardiac abnormalities are accompanied by other abnormalities [20-22]. In addition, in some cases, cardiac abnormalities are part of a syndromic problem [23,24]. In the present study, most cases (57.8%) had isolated cardiac anomalies, and 42.2% had concomitant anomalies. The results of previous studies in this field are very different, and the prevalence of concomitant anomalies has been reported from 5% to 73% [25,26]. The most common extracardiac accompanying abnormalities in our study are head, neck, and central nervous system abnormalities, followed by gastrointestinal, organ, thoracic, and genitourinary abnormalities, respectively. In this regard, the results of previous studies are different. According to a study by C. Stoll et al., which examined comorbid anomalies in 25 articles published in this field, the most common concomitant anomalies were musculoskeletal and gastrointestinal, urinary, and face and mouth were reported [9].
Regarding the association of cardiac abnormalities with chromosomal and genetic abnormalities, the results vary according to the study’s time and the examination type [27]. As in the studies of three decades ago, the rate of this association was reported to be 3% [28]. but in more recent studies, which have studied this issue more closely, the association of cardiac abnormalities with chromosomal abnormalities has been reported at up to 33% [26]. In general, the most common chromosomal abnormalities that have been reported with previous anomalies were Down syndrome and trisomy 18, respectively [29].
Due to the limited number of cases in which chromosomal and genetic studies were performed, we were not able to statistically accurately assess and correlate them with other variables, but out of 6 cases with chromosomal abnormalities, four were Down syndrome, and two were trisomy 18, which is consistent with previous studies. Another noteworthy point in this regard is the high association of AVSD with chromosomal disorders based on previous studies [30], which our study also reported four cases of AVSD out of six cases with chromosomal disorders (Figure 1). Even though there is not a recognizable relationship between TGA and numerical chromosomal abnormalities like Trisomy 18 and 21, we have presented a case of Down syndrome with TGA [24,31] (Table 6).
Table 6: Cases of chromosomal and genetic disorders.
| Case | Chromosomal disorder | Fetal sex | Type of cardiac anomaly | Extracardiac accompanying anomaly | Pregnancy problems |
|---|---|---|---|---|---|
| Case 1 | Down syndrome | Female | AVSD | Gastrointestinal system | Hydrops |
| Case 2 | Down syndrome | Male | AVSD | Head, neck, and nervous system + Limbs | IUGR |
| Case 3 | Trisomy 18 | Female | VSD+TR | Head, neck, and nervous system + Limbs + Gastrointestinal system | IUGR |
| Case 4 | Down syndrome | Female | AVSD | Non | Non |
| Case 5 | Trisomy 18 | Male | AVSD | Gastrointestinal system | Non |
| Case 6 | Down syndrome | Female | TGA | Head, neck, and nervous system | Non |
Bensemlali et al. discovered that when extracardiac abnormalities accompanied CHD, the mortality rate in children born alive was higher. They also demonstrated that these associations were unrelated to the severity of the CHD [32]. Zyblewski et al. showed that an associated chromosomal abnormality rather than the CHD’s severity could contribute to pregnancy termination [33].
Meberg et al. showed that CHDs with associated anomalies compared to isolated CHDs are associated with a significantly higher mortality rate, indicating the lethality of these conditions or the severity of CHDs in these cases [34]. Russo et al. reported an overall mortality rate of 25%, increasing to 54% in cases of CHD detected before 24 weeks of gestation. It was impacted significantly by chromosomal abnormalities, extracardiac abnormalities, or both, and the degree of the abnormality [35].
Sananes et al. indicate that the risk of severe CHD appears to be greater in cystic hygroma Colli and hydrops cases than in patients with elevated nuchal translucency [36].
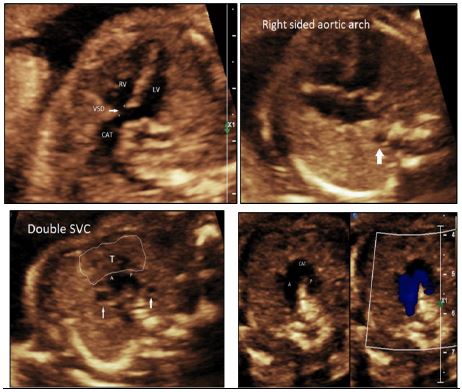
According to a survey conducted by Chen et al., cystic hygroma has a poor outcome because it is usually associated with hydrops fetalis and chromosomal abnormalities, especially in fetuses with other major malformations [37]. Here a rare case of a fetus with cystic hygroma accompanied with multiple anomalies is shown (Figure 4).
The main limitation of our study is the low number of patients. Moreover, the chromosomal Assessment has not been performed for all cases. Furthermore, some potentially influential factors, such as birth term and birth weight, were not available for this study. Generally, our study’s rate of live births is lower than in other studies. Given that our study was conducted in a referral center and many cases were referred from forensic medicine for abortion licenses, the relatively high rate of abortions in this study seems to be justified.
Conclusion
Generally, the major cardiac anomalies and their association with extracardiac abnormalities reduce the likelihood of live birth. Moreover, those minor anomalies accompanied by hydrops and cystic hygroma have a poorer prognosis than other isolated minor anomalies. Overall, the existence of major cardiac anomalies rather than hydrops and cystic hygroma is a more significant factor influencing the outcome of pregnancy.
Declarations
Ethics approval and consent to participate: This study was approved by the ethics committee of Tehran University of Medical Sciences with approval number: IR.TUMSMEDICINE.REC.1400.151.l patients included in this research gave written informed consent to publish the data contained within this study.
Funding: He authors did not receive any funding in the study
Acknowledgments : Not applicable.
References
- Rocha LA, Araujo Júnior E, Rolo LC, et al. Prenatal detection of congenital heart diseases: one-year survey performing a screening protocol in a single reference center in Brazil. Cardiol Res Pract. 2014; 2014: 175635.
- Clur S, Van Brussel P, Mathijssen I, Pajkrt E, Ottenkamp J, et al. Audit of 10 years of referrals for fetal echocardiography. Prenat diagn. 2011; 31: 1134-1140.
- Galindo A, Herraiz I, Escribano D, Lora D, Melchor JC, et al. Prenatal detection of congenital heart defects: A survey on clinical practice in Spain. Fetal Diagn Ther. 2011; 29: 287-295.
- Cai M, Huang H, Su L, et al. Fetal congenital heart disease: Associated anomalies, identification of genetic anomalies by single-nucleotide polymorphism array analysis, and postnatal outcome. Medicine (Baltimore). 2018; 97.
- Levi S, Zhang WH, Alexander S, Viart P, Grandjean H, et al. Short‐ term outcome of isolated and associated congenital heart defects in relation to antenatal ultrasound screening. Ultrasound Obstet Gynecol. 2003; 21: 532-538.
- Araujo Júnior E, Tonni G, Chung M, Ruano R, Martins WP. Perinatal outcomes and intrauterine complications following fetal intervention for congenital heart disease: systematic review and meta‐analysis of observational studies. Ultrasound Obstet Gynecol. 2016; 48: 426-433.
- Mellander M. Perinatal management, counselling and outcome of fetuses with congenital heart disease. Semin Fetal Neonatal Med. 2005; 10: 586-593.
- Allan LD, Huggon IC. Counselling following a diagnosis of congenital heart disease. Prenat Diagn. 2004; 24: 1136-1142.
- Stoll C, Dott B, Alembik Y, Roth M-P. Associated noncardiac congenital anomalies among cases with congenital heart defects.Eur J Med Genet. 2015; 58: 75-85.
- Moradi B, Tahmasebpour A-R, Kazemi MA, Sharifian H, Rokni-Yazdi H. Prenatal diagnosis of concurrent facial and cerebral vascular malformation which caused congestive heart failure.Middle East Fertil Soc J.2017; 22: 343-346.
- Heron MP. Deaths: leading causes for 2015. Natl Vital Stat Rep. 2017; 66: 1-76.
- Control CfD, Prevention. Data and statistics on congenital heart defects.June 6, 2019. Available at: http://www.https://www.cdc.gov/ncbddd/heartdefects/data.html. Accessed may 26, 2011.
- Özbarlas N, Erdem S, Küçükosmanoğlu O, et al. Prevalence and distribution of structural heart diseases in high and low risk pregnancies. Anatol J Cardiol. 2011; 11.
- Emam SM. High prevalence of complex congenital cardiac anomalies detected by fetal echocardiography in a cohort of Saudi women referred for prenatal assessment. J Egypt Soc Parasitol. 2012; 240: 1-10.
- Tegnander E, Williams W, Johansen O, Blaas HG, Eik‐Nes S. Prenatal detection of heart defects in a non‐selected population of 30 149 fetuses—detection rates and outcome. Ultrasound Obstet Gynecol. 2006; 27: 252-265.
- Donofrio MT, Moon-Grady AJ, Hornberger LK, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation. 2014; 129: 2183-2242.
- Moradi B, Kazem MA, Shirazi M. Impact of Fetal Weight in Assessment of Fetal Cardiac Output in Three Cases of High Output Cardiac Failure. JOGCR. 2018; 3: 83-86.
- Yokouchi-Konishi T, Yoshimatsu J, Sawada M, et al. Recurrent congenital heart diseases among neonates born to mothers with congenital heart diseases. Pediatr Cardiol. 2019; 40: 865-870.
- Brodwall K, Greve G, Leirgul E, Tell GS, et al.Recurrence of congenital heart defects among siblings—a nationwide study. Am J Med Genet Part A. 2017; 173: 1575-1585.
- Greenwood RD, Rosenthal A, Parisi L, Fyler DC, Nadas AS. Extracardiac abnormalities in infants with congenital heart disease. Pediatrics. 1975; 55: 485-492.
- Wallgren E, Landtman B, Rapola J. Extracardiac malformations associated with congenital heart disease. Eur J Cardiol. 1978; 7: 15-24.
- Song M, Hu A, Dyhamenahali U, et al. Extracardiac lesions and chromosomal abnormalities associated with major fetal heart defects: Comparison of intrauterine, postnatal and postmortem diagnoses. Ultrasound Obstet Gynecol.2009; 33: 552-559.
- Copel JA, Pilu G, Kleinman CS. Congenital heart disease and extracardiac anomalies: Associations and indications for fetal echocardiography. Am J Obstet Gynecol. 1986; 154: 1121-1132.
- Pajkrt E, Weisz B, Firth HV, Chitty LS. Fetal cardiac anomalies and genetic syndromes. Prenat Diagn. 2004; 24: 1104-1115.
- Wojtalik M, Mrówczyński W, Henschke J, et al. Congenital heart defect with associated malformations in children. J Pediatr Surg. 2005; 40: 1675-1680.
- Jorgensen M, McPherson E, Zaleski C, Shivaram P, Cold C. Stillbirth: The heart of the matter. Am J Med Genet Part A. 2014; 164: 691-699.
- Moradi B, Moosavi NS, Kazemi MA, Tahmasebpour AR, Fattahi Masrour F, et al. A case of prenatally detected left isomerism and hemiazygos continuation of inferior vena cava. J Clin Ultrasound. 2017; 45: 430-33.
- Hanna EJ, Nevin NC, Nelson J. Genetic study of congenital heart defects in Northern Ireland (1974-1978). J Med Genet. 1994; 31: 858-863.
- Lowry RB, Bedard T, Sibbald B, et al. Congenital heart defects and major structural noncardiac anomalies in Alberta, Canada, 1995–2002. Birth Defects Res A Clin Mol Teratol. 2013; 97: 79-86.
- Rankin J, Tennant PW, Bythell M, Pearce MS. Predictors of survival in children born with Down syndrome: A registry-based study. Pediatrics. 2012; 129: e1373-e1381.
- Petracchi F, Sisterna S, Igarzabal L, Wilkins‐Haug L. Fetal cardiac abnormalities: Genetic etiologies to be considered. Prenat Diagn. 2019; 39: 758-780.
- Bensemlali M, Bajolle F, Ladouceur M, et al. Associated genetic syndromes and extracardiac malformations strongly influence outcomes of fetuses with congenital heart diseases. Arch Cardiovasc Dis. 2016; 109: 330-336.
- Zyblewski SC, Hill EG, Shirali G, et al. Chromosomal anomalies influence parental treatment decisions in relation to prenatally diagnosed congenital heart disease. Pediatr cardiol. 2009; 30: 1105-1111.
- Meberg A, Hals J, Thaulow E. Congenital heart defects—chromosomal anomalies, syndromes and extracardiac malformations. Acta Paediatr. 2007; 96: 1142-1145.
- Russo MG, Paladini D, Pacileo G, et al. Changing spectrum and outcome of 705 fetal congenital heart disease cases: 12 years, experience in a third-level center. J Cardiovasc Med. 2008; 9: 910-915.
- Sananes N, Guigue V, Kohler M, et al. Nuchal translucency and cystic hygroma colli in screening for fetal major congenital heart defects in a series of 12,910 euploid pregnancies. Ultrasound Obstet Gynecol. 2010; 35: 273-279.
- Chen Y-N, Chen C-P, Lin C-J, Chen S-W. Prenatal ultrasound evaluation and outcome of pregnancy with fetal cystic hygromas and lymphangiomas. J Med Ultrasound. 2017; 25: 12-15.