
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A complex case of metastatic pituitary lesions
with unusual presentation
Ahmad Waqar1*; Khan Irfan Iqbal1; Chohan Mohammad Tahir1; Dhakshinamoorthy Barkavi1; Batra Arun2; Scoones David3; Maillo-Nieto Angeles4; Arutchelvam Vijayaraman1
1South Tees Hospitals NHS Foundation Trust, Department of Endocrinology, Marton Road, Middlesbrough, TS4 3BW, United Kingdom.
2South Tees Hospitals NHS Foundation Trust, Department of Radiology, Marton Road, Middlesbrough, TS4 3BW, United Kingdom.
3South Tees Hospitals NHS Foundation Trust, Department of Pathology, Marton Road, Middlesbrough, TS4 3BW, United Kingdom.
4Newcastle Upon Tyne Hospitals NHS Foundation Trust, Department of Endocrinology, Freeman Rd, High Heaton, Newcastle upon Tyne, NE7 7DN, United Kingdom.
*Corresponding Author : Ahmad Waqar
South Tees Hospitals NHS Foundation Trust, Department of Endocrinology, Marton Road, Middlesbrough, TS4 3BW, United Kingdom.
Ph: +44 7305236256;
Email: drwaqarahmad786@yahoo.com
Received : Feb 26, 2023
Accepted : Mar 16, 2023
Published : Mar 23, 2023
Archived : www.jcimcr.org
Copyright : © Waqar A (2023).
Abstract
Metastases to the pituitary gland and hypothalamus commonly occur with breast cancer in women. It is unusual and rare if these metastases are discovered late (10 or more years of primary tumor diagnosis), follow an indolent course and have radiological features suggestive of the inflammatory process. We report a case of a 71 years old female who presented with collapse, which was suspected secondary to adrenal crises, and gradual deterioration of visual acuity on the background of treated breast cancer (10 years ago) with no disease recurrence for five years of surveillance mammography. She was found to have panhypopituitarism. Her pituitary profile was stable on hormone replacement (Hydrocortisone, Levothyroxine and Desmopressin), and pituitary MRI was suggestive of the inflammatory process. She was treated with higher doses of steroids which did not give any clinical or radiological improvement on serial pituitary imaging. Blood tests, including ACE levels, Treponemal antibodies, Quantiferon for TB, autoimmune screen and CSF investigations, including cytology for malignant cells, ACE levels, fungal & mycobacterial cultures and viral PCR, all came back negative, which ruled out any inflammatory pathology. CT thorax abdomen & pelvis and FDG PET CT of the whole body did not show any evidence of occult malignancy. A pituitary biopsy confirmed metastasis from the known breast carcinoma with immunohistochemical evidence of neuroendocrine differentiation in the primary tumor. This case illustrates that pituitary metastasis from breast cancer can present ten years after the initial diagnosis and can follow an indolent course with no metastasis elsewhere. Radiological features can be atypical of metastatic lesions.
Keywords: Pituitary; Metastasis; Breast cancer; Pituitary imaging; Inflammation.
Citation: Waqar A, Iqbal KI, Tahir CM, Barkavi D, Arun B, et al. A complex case of metastatic pituitary lesions with unusual presentation. J Clin Images Med Case Rep. 2023; 4(3): 2338.
Introduction
Pituitary and sellar region tumours account for 15% of all brain tumours. The most common are adenomas, but other tumours like craniopharyngiomas, germ cell tumours, mesenchymal tumours and metastatic deposits are also seen, representing 1% of all surgical cases of pituitary tumours [1,2]. Breast cancer is one of the most common malignancies that metastasise to the brain accounting for 15% of all brain metastasis only preceded by lung cancer (48%) [3]. Pituitary metastasis is commonly secondary to lung and breast carcinomas. Still, late presentation, defined as metastasis after ten or more years of primary diagnosis [3], is rare, yet late metastatic presentation with no metastasis elsewhere is infrequent.
We report a case of hypopituitarism secondary to pituitary metastatic breast cancer in a 71-year-old woman.
Case presentation
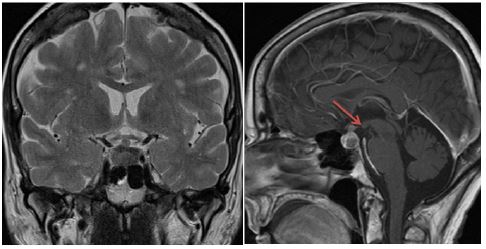
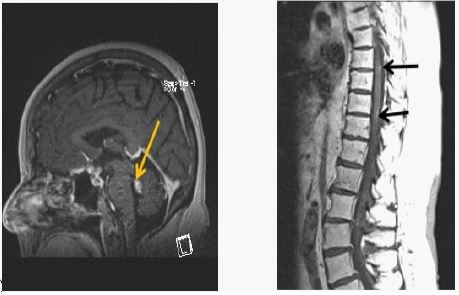
71 year mobile, independent lady was diagnosed with panhypopituitarism with corticotroph, thyrotroph, gonadotroph failure and cranial diabetes insipidus during hospital admission in May 2019. Her pituitary MRI with contrast showed enlarged pituitary with nodular thickening of the stalk and absented posterior bright spot (Figure 1). She was started on hydrocortisone, levothyroxine and desmopressin. Her case was discussed in the pituitary Multidisciplinary Team (MDT) meeting, and the recommendation was made to repeat an MRI pituitary following three months of oral prednisolone 30 mg.
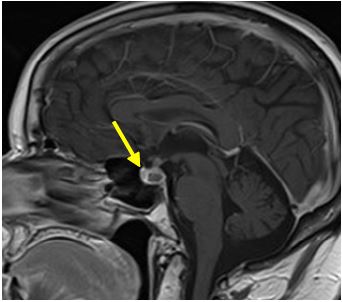
Her repeat pituitary MRI in September 2019 showed a reduction in the thickness of the pituitary stalk with no suprasellar or cavernous extension (Figure 2). Furthermore, her steroid dose was weaned down to the physiological dose of hydrocortisone in February 2020.
She had a history of breast carcinoma treated with a left mastectomy and axillary node clearance in May 2010, followed by adjuvant chemotherapy. In addition, she had hormonal therapy with Letrazole until five years ago. Annual surveillance mammograms from 2011-2015 showed no evidence of disease recurrence.
She had a regular endocrine follow-up. Her pituitary profile, including serum & urine osmolality and urinary sodium, remained stable on hormonal replacement. She was seen by an optometrist in May 2020 for the sudden loss of vision in the left eye without ocular pain and diplopia. She had reduced Visual acuity in the left eye with normal optic disc and macula but the loss of neural tissue on disc scans. On review by the ophthalmologist, the impression of compressive optic neuropathy versus steroid-induced glaucoma was established. Although repeat pituitary MRI at that stage showed no change in the size of the relatively bulky pituitary, imaging features were suggestive of lymphocytic hypophysitis. Furthermore, the response to the short synacthen test was insufficient; she was continued on long-term hydrocortisone. Unfortunately, she had complete vision loss in her left eye by July 2020.
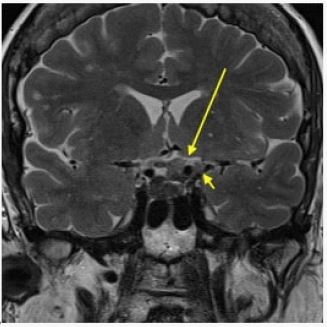
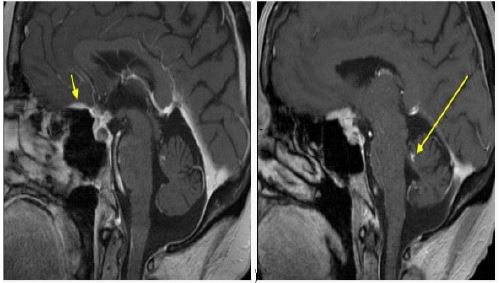
She had another ophthalmologist review in September 2020 due to reduced vision in the right eye. MRI brain showed worsening elevation of the left-sided optic chiasm, which was swollen. Early high T signal change on the left side of optic chiasm in the pre-chiasmatic segment of the left optic nerve was noted (Figure 3). MRI pituitary showed progression of enhancing sellar and hypophyseal lesion with extension into the planum sphenoidale and left clinoid process. Overall, the findings suggested relapse of an inflammatory process (Figure 4). She stayed on hydrocortisone 20 mg daily.
She was admitted in September 2020 with a collapse and was treated for a suspected adrenal crisis. She also developed gradual visual deterioration in her right eye. As per MDT, she was given three doses of 250 mg IV methylprednisolone. MRI pituitary done pre- and post-methylprednisolone showed an unchanged appearance as the post-steroid scan was performed too early to demonstrate the effect of steroid therapy. Unfortunately, visual acuity in the right eye did not improve significantly.
During hospital admission, a neurologist review led to the impression of neurosarcoidosis. Lumbar puncture for microbiology & cytology for malignant cells, serum/CSF ACE levels, autoimmune screen, serum treponemal antibodies and Quantiferon tuberculosis testing were performed, which all came back negative.
She was discharged home with Prednisolone 60 mg daily, aiming to repeat an MRI pituitary with contrast in a few weeks to assess steroid response. MRI pituitary (October 2020) showed a slight reduction in the Dural/cavernous sinus and suprasellar enhancing nodular tissue.
Meanwhile, she stayed under regular endocrine, neurology, ophthalmology and neurosurgery follow-up and was discussed repeatedly in pituitary MDT. As a result, steroids were slowly weaned to physiological doses without any clinical change.
CT thorax, abdomen and pelvis in December 2020 showed no evidence of occult malignancy or breast cancer recurrence. Whole-body Fludeoxyglucose (FDG) Positron emission tomography CT showed equivocal FDG uptake within the pituitary gland, and no FDG avid primary or secondary malignancy was demonstrated elsewhere. There was no convincing evidence of extracranial lymphoma or sarcoidosis on FDG PET CT. Hence, she remained in a diagnostic dilemma.
She had a repeat diagnostic lumbar puncture in January 2021 to look for biochemical evidence of neurosarcoidosis or lymphoma, which returned normal. MRI brain & whole spine in Feb2021 showed deposits in the cerebellum at the level of the 4th ventricle along with intra-spinal deposits (Figure 5)
MRI pituitary & whole spine in May 2021 showed progressive disease, particularly in the anterior cranial fossa and cauda equine. After discussion in Pituitary MDT, it was unanimously decided to proceed with pituitary biopsy, given diagnostic uncertainty.
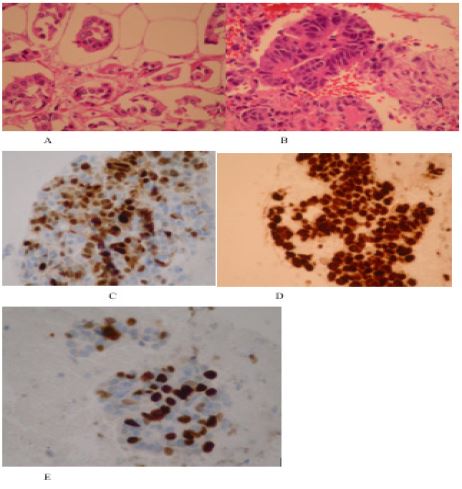
She underwent an endoscopic transsphenoidal biopsy in May 2020. Histopathology from pituitary samples showed fibrosis with hemosiderin deposition and infiltration by cytologically atypical epithelial cells showing glandular differentiation. Immunohistochemical staining was focally positive for CK7 and negative for CK20. It was positive for GATA3, oestrogen and progesterone receptors and very focally for gross cystic disease fluid protein. It was negative for PAX8. Ki-67 immunostaining showed a high proliferation rate. There was some immunohistochemical evidence of neuroendocrine differentiation with positive immunostaining for chromogranin and synaptophysin (Figure 6). Given this, immunostaining for these markers was retrospectively performed on the breast carcinoma. Although the primary breast carcinoma did not show morphological features suggestive of neuroendocrine differentiation, it was also positive for these markers. The morphological and immunohistochemical findings were in keeping with metastasis from the previous primary breast carcinoma.
She was referred to an oncologist to assess whether she was appropriate for chemo and radiotherapy. Still, unfortunately, she passed away due to cardiac arrest before any treatment was planned.
Discussion
Pituitary metastasis is primarily asymptomatic, but common presentations include headache, visual symptoms, visual field defects, diabetes insipidus and pituitary hormone deficiencies [4].
Metastasis commonly occurs in the posterior pituitary and is usually due to the homogeneous spread of malignant cells, which disseminate to the posteriorpituitary easier, supplied by the hypophyseal-portal-system [5]. While the posterior lobe of the pituitary is the most common site for metastasis, it can also involve the anterior pituitary and the stalk. Diabetes insipidus develops with posterior pituitary or stalk involvement, manifested in less than 1 % of adenomas. In a series of 52 patients with pituitary metastasis, Heshmati et al. found that visual impairment (visual field defect or extraocular palsy) was the presenting complaint in 56% of subjects. Diabetes insipidussignalled pituitary involvement in 40% of patients in their series [6]. However, in our patient, the symptoms of visual impairment and diabetes insipidus were present. Still, the bulky stalk initially pointed towards inflammatory processes (lymphocytic hypophysitis, neurosarcoidosis) rather than adenoma or metastasis. In addition, the breast cancer was well treated and followed up, and the lady didn’t have any evidence of metastasis elsewhere, making pituitary metastasis less likely; hence, she was investigated for inflammatory processes.
The most common site for pituitary metastasis is from the breast in females and the lungs in males [7]. Metastasis is also reported from kidneys, prostate and pancreas, but breast and lung entail two-thirds of pituitary metastasis [8]. The first manifestations are metastasis elsewhere, such as lymph nodes, lungs or bone. Metastasis to the pituitary gland occurs later, mostly detected incidentally and usually occurs in the end stages of cancer [6,9]. Contrary to this, our patient presented with pituitary metastasis without evidence of extra CNS metastasis supported by intensive investigations in the form of CT thorax, abdomen and pelvis and FDG PET, which led to a delay in the diagnosis as the pituitary MRI was also favouring the inflammatory process rather than metastasis and the possibility of pituitary metastasis without metastasis elsewhere is very small.
It is challenging to diagnose pituitary metastasis; symptoms are non-specific, with few differences between metastatic lesions, inflammatory process and adenomas on neuroimaging, which can be misleading, as in our patient. Still, at the same time, it is vital to find whether a pituitary tumour is primary or secondary to guide the treatment. Hence tissue sampling is required in most cases. Once the lesion is confirmed to be metastatic, the therapy entails pituitary hormone replacement and symptomatic relief with local tumour control in the form of surgery followed by chemo-radiotherapy. However, the prognosis depends on the source and extent of the primary lesion [10]. Reported life expectancy ranges from 6 to 22 months but declines to 2-4 months in case of stalk invasion [4,9]. The surgical intervention can improve visual symptoms.
In our case, the diagnosis was challenging till the biopsy; breast cancer remained in remission for more than ten years, followed an indolent course and presented with metastasis to the pituitary gland before metastasising anywhere else.
The case reflects that the metastatic lesions of the pituitary gland can mimic signs and symptoms of pituitary adenoma or inflammatory process, leading to a delay in diagnosis of several months. The absence of specific radiological signs make it difficult to distinguish these metastatic lesions from other more common benign pituitary lesions [11,12]. Usually, in clinical practice, breast cancer patients are followed up for 5-8 years after cancer treatment. Like this, few cases in the literature have been published stating it can present late, even after ten years of completed cancer treatment, emphasising the importance of extended follow-up post-cancer treatment [13].
Conclusion
To conclude, pituitary metastasis can present even ten years after the initial diagnosis of breast cancer. It can follow an indolent course with no evidence of metastasis elsewhere. Radiological features of pituitary metastasis may resemble inflammatory pituitary processes.
Consent: Written informed consents were obtained.
Conflict of interest: No potential conflict of interest.
References
- Lin B, Huang D, Yang X, et al. Distribution of brain metastases: low risk metastasis areas may be avoided when treating with whole‐brain radiotherapy. Cancer Imaging. 2020; 20:29.
- Komninos J, Vlassopoulou V, Protopapa D, et al. Tumors metastatic to the pituitary gland: case report and literature review. J Clin Endocrinol Metab. 2004; 89: 574-580.
- Gabrovski N, Poptodorov G, Velinov N, Gabrovski S. [Late metastases from breast cancer--report of two cases]. Khirurgiia (Sofiia). Bulgarian. 2010; 1: 62-66.
- Fassett DR, Couldwell WT. Metastases to the pituitary gland. Neurosurg Focus. 2004; 16: E8.
- Sturm I, Kirschke S, Krahl D, Dörken B. Panhypopituitarism in a patient with breast cancer. Onkologie. 2004; 27: 480-482.
- Heshmati HM, Scheithauer BW, Young WF. Metastases to the pituitary gland. Endocrinologist. 2002; 12: 45-49.
- Weil RJ. Pituitary metastasis. Arch Neurol. 2002; 59: 1962-1963.
- Teears RJ, Silverman EM. Clinicopathologic review of 88 cases of carcinoma metastatic to the pituitary gland. Cancer. 1975; 36: 216-220.
- Kurkjian C, Armor JF, Kamble R, Ozer H, Kharfan-Dabaja MA. Symptomatic metastases to the pituitary infundibulum resulting from primary breast cancer. Int J Clin Oncol. 2005; 10: 191-194.
- Morita A, Meyer FB, Laws ER Jr. Symptomatic pituitary metastases. J Neurosurg. 1998; 89: 69-73.
- Suganuma H, Yoshimi T, Kita T, Okano H, Suzuki Y, Oki Y, et al. Rare case with metastatic involvement of hypothalamo-pituitary and pineal body presenting as hypopituitarism and diabetes insipidus. Intern Med. 1994; 33: 795-798.
- Branch CL, Laws ER. Metastatic tumors of the sella turcica masquerading as primary pituitary tumors. J Clin Endocrinol Metab. 1987; 65: 469-474.
- Spinelli GP, Lo Russo G, Miele E, Prinzi N, Tomao F, et al. Breast cancer metastatic to the pituitary gland: A case report. World Journal of Surgical Oncology. 2012; 10: 1-4.