
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
The effect of dyssynchrony on hemodynamics
after pacemaker implantation
Chieko Sakai1; Michiyo Yamano2,3*; Mayumi Takeoka3; Yoshimi Sato1; Tatsuya Kawasaki1
1sDepartment of Cardiology, Matsushita Memorial Hospital, Osaka, Japan.
2Department of Cardiovascular Medicine, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan.
3Central Clinical Laboratory, Matsushita Memorial Hospital, Osaka, Japan.
*Corresponding Author : Michiyo Yamano
Department of Cardiovascular Medicine, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kajii-cho 465, Kawaramachi-Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan.
Tel: +81-75-251-5511; Fax: +81-75-251-5514;
Email: m.yamano823@gmail.com
Received : Mar 02, 2023
Accepted : Mar 17, 2023
Published : Mar 24, 2023
Archived : www.jcimcr.org
Copyright : © Yamano M (2023).
Abstract
We analyzed the correlation between Left Ventricular (LV) contraction and right ventricular pacing position via longitudinal strain on 2-dimensional speckle-tracking echocardiography in a patient underwent permanent pacemaker implantation and developed pacemaker induced cardiomyopathy. Furthermore, the effect of dyssynchrony was quantitatively assessed by LV pressure-strain loop based on systemic blood pressure and LV longitudinal strain.
Keywords: Pacemaker-induced cardiomyopathy; 2-d speckle tracking; Myocardial work.
Abbreviations: LV: Left Ventricular; PICM: Pacemaker-Induced Cardiomyopathy; PMI: Pacemaker Implantation; RV: Right Ventricular.
Citation: Sakai C, Yamano M, Takeoka M, Sato Y, Kawasaki T, et al. The effect of dyssynchrony on hemodynamics after pacemaker implantation. J Clin Images Med Case Rep. 2023; 4(3): 2340.
Clinical image description
Some patients develop impaired Left Ventricular (LV) contraction due to dyssynchrony after Permanent Pacemaker Implantation (PMI), i.e., Pacemaker-Induced Cardiomyopathy (PICM), which may cause symptomatic heart failure. Although proper Right Ventricular (RV) pacing position may prevent PICM, there are no well-established methods for achieving this [1]. It is feasible to analyze the correlation between LV contraction and pacing position via longitudinal strain on 2-dimensional speckle-tracking echocardiography. Negative strain initially appears in the inferolateral area, and contraction spreads toward both the septal and lateral areas in a patient with complete atrioventricular block (Figure 1A). The RV lead was positioned at the septum at time of the first PMI. The next day, the patient developed pulmonary congestion and shock. Echocardiography showed a prominent septal flash and apical shuffle motion. Negative strain appears in the septal area and spreads to the lateral side (Figure 1B). The RV lead was replaced from the septum to the apex because PICM occurred. After the second PMI, the degree of dyssynchrony improved and symptoms disappeared. Negative strain appears in the apical to septal area and spreads toward the inferior and lateral sides (Figure 1C). Furthermore, a noninvasive method of estimating myocardial work based on systemic blood pressure and LV longitudinal strain, i.e., LV pressure-strain loop, has been introduced [2]. The global constructive work decreased and the global wasted work increased after the first PMI located at the RV septum; however, these values improved after the pacing position was changed to RV apex (Figure 1D).
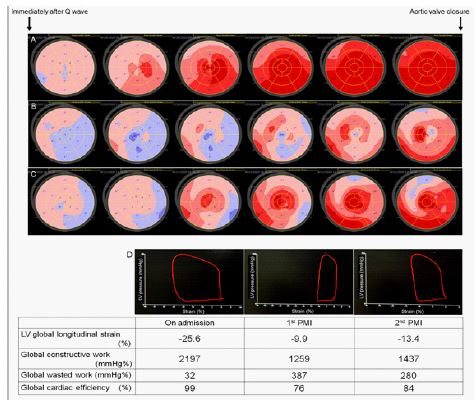
(A) Negative strain initially appears in the inferolateral area, and contraction spreads toward both the septal and lateral areas.
(B) Negative strain appears in the septal area and spreads to the lateral side.
(C) Negative strain appears in the apical to septal area and spreads toward the inferior and lateral sides.
Figure 1D
The LV pressure-strain loops at each clinical time point. The area surrounded by each LV pressure-loop indicates the global myocardial work index from mitral valve closure through mitral valve opening. Constructive Work (CW) indicates work performed during shortening in systole, including negative work during Lengthening In Isovolumetric Relaxation (IVR). Wasted Work (WW) indicates negative work performed during lengthening in systole, including work performed during shortening in IVR. The myocardial work efficiency (%) = CW / (CW + WW).
Declarations
Author contributions: C.S. and M.Y. designed a case study. C.S, M.Y., and M.T. collected the data. M.Y. and M.T. performed the analysis. C.S. and M.Y. wrote the manuscript with support from Y.S. and T.K.
Acknowledgement: The authors declare that they have no conflicts of interest.
References
- Kaye G. The quest for physiological pacing-Does one size fit all? J Cardiovasc Electrophysiol. 2019; 30: 2977-2980.
- Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur Heart J. 2012; 33: 724-733.