
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Cardioverter defibrillator placement in a young woman
with Brugada syndrome: A case report and review
Denisse Y Lazarín Valles1; Lydia Enith Nava Rivera2; Rodrigo Lozoya Martínez2; Nadia D Betancourt Martínez2; Javier Morán Martínez2*
11Departamento de Emergencias, Hospital General de Zona, Instituto Mexciano del Seguro Social Número 16. Boulevard Revolución Colonia, Torreón Jardín, Torreón, Coahuila, México. C.P. 27100.
22Departamento de Biología Celular y Ultraestructura, Centro de Investigación Biomédica. Facultad de Medicina. Universidad Autónoma de Coahuila. Torreón, Coahuila, México. Gregorio A. Garcia No. 198 sur. Toreeón, Coahuila, México. C.P. 27000.
*Corresponding Author : Javier Morán Martínez
Departamento de Biología Celular y Ultraestructura, Centro de Investigación Biomédica. Facultad de Medicina. Universidad Autónoma de Coahuila. Torreón, Coahuila, México. Gregorio A. Garcia No. 198 sur. Toreeón, Coahuila, México. C.P. 27000.
Phone: +(871)7171077;
Email: javiermoranmartinez@uadec.edu.mx
Received : Mar 01, 2023
Accepted : Mar 20, 2023
Published : Mar 27, 2023
Archived : www.jcimcr.org
Copyright : © Martinez JM (2023).
Abstract
Brugada Syndrome (BS) is a hereditary disorder characterized by a primary electrical abnormality, absence of structural heart disease, an elevated risk of sudden death, polymorphous ventricular tachycardia, and ventricular fibrillation, which mainly affects young men. The heterogeneous clinical presentation of this syndrome in contrast to an asymptomatic presence, reinforces the interest in the documentation of management and proper treatment of this syndrome. Patients diagnosed with BS who have overcome sudden cardiac syncope, have a high risk of Ventricular Arrhythmias (VA), there is a general agreement for the Implantation of a Cardioverter Defibrillator (ICD) in those symptomatic patients, however, there is controversy about the feasibility of its placement because of its association with high rates of in appropriate shocks and complications. In the following case, we report the diagnosis of Brugada syndrome of a young woman with a history of secondary hypothyroidism successfully implanted with an automatic defibrillator.
Keywords: Brugada syndrome; Therapeutic; Implantable cardioverter-defibrillator.
Citation: Lazarín Valles DY, Nava Rivera LE, Martínez RL, Betancourt Martínez ND, Martínez JM. Cardioverter defibrillator placement in a young woman with Brugada syndrome: A case report and review. J Clin Images Med Case Rep. 2023; 4(3): 2342.
Introduction
Patients often go to the emergency room with palpitations or syncope, most of them have benign conditions with a favorable prognosis; however, those whose syncope has a cardiac origin, present a mortality rate between 18-33%, in contrast with 0-12% for non-cardiogenic syncope and 6% for unexplained syncope. Syncope of cardiac origin may be classified as structural or arrhythmogenic origin and may be the only warning of a potential sudden cardiac death [1]. Brugada Syndrome (BS) is a genetically determined primary cardiac pathology with a worldwide prevalence estimated in 1 to 5 per 10,000 inhabitants in the West and a higher occurrence in Eastern countries (1/2,500 inhabitants) [2]. This disease is characterized by a distinctive electrocardiographic features and increased risk of sudden cardiac death, secondary to Ventricular Arrhythmias (VA) such as polymorphic ventricular tachycardia or ventricular fibrillation, most of which manly affects individuals in the fourth decade of their life [3]. The clinical presentation is heterogeneous, nontheless many patients are asymptomatic [4]. With regard to the appropriate treatment for this pathology, there are several pharmacological options asisoproterenol [5], quinidine [6] and phosphodiesterase III inhibitors [7]. However more studies are still required to better define the benefits of their employment. In this regard, radiofrequency ablation of ventricular ectopy, has shown to be useful in the prevention of VA in BS patients [8]. Though the only proven effective therapyso faris the use of an implantable Cardioverter-Defibrillator (ICD) that is indicated only in symptomatic patients with a spontaneous ECG pattern, because the rates decrease in patients who were asymptomatic at implantation [9]. Though, there is still controversy about its relationship with a high rate of inappropriate shocks and a prevalence of device-related complications, that increases with the follow-up duration required for patients with this channelopathy [10,11].
Case report
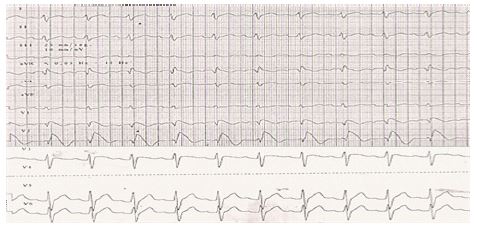
A 28-year-old woman with a history of hypothyroidism secondary to Hashimoto’s Thyroiditis with 11 years since diagnosis, on treatment with levothyroxine 100 mcg/day, dysautonomy with a mixed response of 1 year of evolution on treatment with propranolol 20 mg/12 h and hygienic-dietary recommendations. Multiple hospitalizations in due to hypotension and tachycardias requiring beta-blocker dosage adjustment and use being suspended 1 month prior to hospitalization. Control ECGs were done while receiving propafenone, however, none of its alterations associated to class I antiarrhythmic adverse effects. On March 13th, the patient showed headache, dizziness, vertigo, and bradycardia, symptoms persisted. After withdrawal of beta-bloker and she was evaluated by the otorhinolaryngology department who discarded vestibular vertigo. On March 15th, still admitted, she presented generalized tonic-clonic seizure that cease without medical management. In postictal phase, she presented a new comitial event presented and she was admitted to the shock-trauma unit of Emergency Room (ER), assuming an hemorrhagic cerebrovascular eventorotracheal intubation was performed, sinus bradycardia was documented by monitor, 1 dose of atropine was administered, evolving to pulseless electrical activity, advanced Cardio Pulmonary Resuscitation (CPR) maneuvers were initiated and 1 dose of adrenaline was administered, recovering pulse, hypotensive and (ECG) with sinus rhythm, Heart Rate (HR) 72 bpm, PR 0.28 ms, QRS 0.14 ms, QT 0.40 ms, intermittent Right Bundle Branch Block (RBBB) and aberrant conduction AV Block (AVB) (Figure 1A).

Fifty minutes later ECG was recorded with sinus rhythm, 132 bpm of HR, PR 0.14 ms, QRS 0.10 ms, QT 0.24 ms with Left Bundle Branch Block Image (LBBB) (Figure 1B), so she was transferred to the Intensive Care Unit (ICU) where the central hemorrhagic event is ruled out. In the ICU, a new ECG was recorded with sinus rhythm, HR 110, PR 0.22 ms, QRS 0.10 ms, QT 0.27 ms, with image of RBBB in V1 and V2 compatible with Brugada type 1 pattern and sign of present aVR (Figure 2) proceeding to the placement of a temporary pacemaker; she was transferred to the Coronary Intensive Care Unit (CICU) where she was extubated without complications, maintaining stable tension figures, adequate heart rate, and pacemaker sentinel state.
Electro physiological studies and a pharmacological challenge were performed, which were negative for induction of ventricular tachycardia, sinus node and AV test with in normal parameters too, so she was discharged, continuing with out patient care, with an indication of following hygienic-dietary recommendations. On April 15th, when she was driving, she had a feeling of syncopal dizziness and blurred vision. She is taken to emergency room where she has a syncopal episode and is monitored again finding pulseless electrical activity. Basic and advanced CPR maneuvers are performed for 12 Minutes, documenting asystole, ventricular tachycardia and refractory hypotension to vasoactive amines. The placement of a temporary pacemake was after a monitor documented ECG pattern Brugada type 1 per monitor (Figure 3).
She was moved to CICU and placed a bicameral defibrillator, she was extubated without complications, dischargerd to the internal medicine ward and subsequently discharged to her residence. As a summary of the follow up, there’s been a favorable evolution, with isolated periods of symptoms related to dysautonomia (hypotension and tachycardia) that in 2 years have required treatment with crystalloid solutions on just 1 occasion and which lasted more than 30 minutes til complete resolution. In regard with high energy therapies and pacemaker function of the ICD, 3 downloads were received on the same occasion, which were considered inappropriate because the record that was noted in the ICD that was supraventricular tachycardias, after which the heart rate was adjusted, to which discharge can be performed without presenting more events until now. Initially, the pacemaker function was predominant until strict dietary indications were atended as weight gain, isotonic drink intake and salt intake 7 g/day improved the basal heart rate of the patient, as well as the decrease in the cardiovascular type of exercise to avoid new episodes of bradycardia.
Discussion
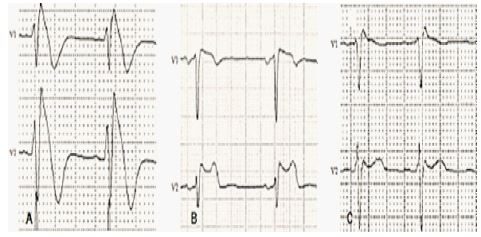
Brugada Syndrome (BS) it’s a channelopathy hereditary, autosomal dominant, with low penetranceor sporadic, which predominantly affects the Right Ventricular Outflow Tract Epicardium (RVOT). Clinically it is manifested by Syncope or Sudden Cardiac Death (SCD) that occurs during rest or night sleep, as a result of episodes of Polymorphic Ventricular Tachycardia (PVT) that may degenerate into Ventricular Fibrillation (VF) in the absence of apparent structural pathology, use of drugs, coronary insufficiency, or electrolytic imbalance [12,13]. In this particular case after presentation episodes of syncope, the bradycardia that evolved to the pulseless electrical activity was always documented. During the resuscitation of the second episode of cardiac arrest, a trace compatible with ventricular tachycardia without pulse was developed in a cardiac monitor however ECG printing was not possible. The BS usually presents in adulthood, although most patients are in the third and fourth decade of life, it has been reported in patients from 2 to 84 years of age. Males are affected more frequently than the females with a ratio of 8-9: 1; the reason for this male preponderance is possibly related to the underlying differences in the hormonal state. It is estimated that BS is responsible for at least 4% of all sudden deaths and at around 20% of all sudden deaths occur in patients without structural heart disease [14]. This disease is genetically heterogeneous; four genes associated with BS have been identified. The first, an A280V mutation in glycerol-3-phosphate dehydrogenase 1-like (GPD1-L) induces an indirect hypofunction of the sodium channel indirectly, making it difficult to transport the sodium through the cell membrane. The novel findings of mutations in the genes CACNA1c and CACNB2b (coding for the calcium channel) and KCNE3 (coding for a beta subunit regulating the transitory potassium currents Ito) have shown that in these cases, although the sodium channel is not affected, the phenotype can be explained because there is an imbalance of ionic currents during phase 1 of the action potential [15]. There is no information about a mutation existing in the treated patient, due to the lack of genetic study, however, there is a familiar background since the patient reports a paternal relative (uncle) who suffered sudden infant death. A potentially fatal cardiac arrhythmia, especially PVT, may occur, if such arrhythmias end spontaneously, patients may present palpitations or syncope [16,17], and if these arrhythmias persist, they may eventually degenerate into VF. The prodromal phase of syncope is characterized by weakness, diaphoresis, bright lights, blurred vision, headache, nausea and sensation of cold extremities. The syncopal phase is brief, during which “seizure-like” movements may occur, recovery is rapid and spontaneous, and headache, weakness, fatigue and pallor may occur at this stage [18,19]. There are still controversies regarding the pathophysiology of BS, and two theories about repolarization and the theory of depolarization have been reported. Regarding the repolarization theory, the authors state that ECG manifestations and the increased risk of ventricular arrhythmias are a consequence of the imbalance found in the ionic currents during the end of phase 1 of the cardiac Action Potential (AP). Decrease of positive in flow currents and/or increase of positive outflow currents result in an accentuation of the notch at the end of stage 1, which causes a ST segment elevation in a “Saddle” or “Bull Terrier” shape as a result of repolarization of the epicardial cells preceding that of the M and endocardial cells, followed by a positive T wave. Eventually the exaggeration of these changes causes loss of AP plateau, especially in the Right Ventricle (RV) epicardium; The ST segment elevation is higher, with a convex morphology, with a negative T wave secondary to the reversal of the sense of repolarization from the endocardium to the epicardium, a consequence of the prolongation of AP in the epicardial cells. The propagation of current from the sites where the AP plateau is maintained to sites of the myocardium where it has disappeared and/or is decreased causes local re-excitation (a phenomenon called “reentry in phase 2”), which determines the appearance of ventricular epicardial extra systoles, Trigger episodes of PVT and/or VF3, [15]. Authors who support the theory of depolarization assert that conduction disorders are the main pathophysiological event, which has been observed in the ECG. These authors also argue that such patients may present minimal structural abnormalities, which would justify the finding of late potentials and conduction disorders. Such conduction disorders are more marked at the RVOT level. When depolarization has started in the RV but not in the RVOT there is current flow towards the latter, which is recorded as elevation of the J point and the ST segment in the right precordial leads. At the beginning of the depolarization in RVOT the AP of the RV is in phase 3, so the potential gradients are reversed, and the current circulation occurs from RVOT to RV, away from the right precordial leads, and recorded as negative T waves [3,15]. It is important to remember that the data found on the BS ECG can be unmasked or intensified by vagal stimulation. Neuro Cardiogenic Syncope (NCS) has been described in patients with BS and there is increasing evidence that autonomic dysfunction contributes significantly to arrhythmogenesis of the disease [20,21]; coupled with this, the existence of a total loss of the ordinary balance between the sympathetic and the parasympathetic cardiac function in the syndrome [4], this balance being the predisposition to the arrhythmias to cause a reduction in the sympathetic activity and the consequent predominance of the parasympathetic tone; partially explaining the higher incidence of ventricular arrhythmias and sudden death in rest and during sleep [1,4,17,21,22]. In contrast, it is posed that the episodes of symptomatic hypotension described in this case were due to a lack of dietetic indications, according to the recommendations of the treating cardiologist. In the case of long-lasting hypoperfusion, seizures similar to the movements observed in an epileptic seizure may be observed [8], leading to incorrect studies and diagnoses. Diagnosis of Brugada syndrome is established when a characteristic repolarization pattern called Type 1 of BS or “coved” in at least 2 right precordial leads (V1 to V3) is observed, and less frequently in the inferior leads (DII, DIII and aVF), characterized by a prominent ST-segment elevation of convex morphology with J-point amplitude or ST segment elevation ≥2 mm, followed by a negative T-wave, associated with a complete or incomplete right bundle branch block (Figure 3A) [3,17,21]. Two other repolarization patterns, respectively called Type 2 BS or saddleback (elevation of point J ≥ 2 mm, ST segment elevation ≥1 mm concave morphology, followed by positive or biphasic T wave) and BS Type 3 (Concave or convex morphology, with ST segment elevation < 1 mm) are considered to be suggestive (Figures 3B and 3C) [3,14,21]. Occasionally electrocardiographic alterations become evident when the position of the V1 and V2 electrodes is raised one or two intercostal spaces with or without the use of sodium channel blockers [12]. The ECG of the BSis dynamic: The same patient may present the 3 electrocardiographic patterns associated with the syndrome at different times, and normal ECG at baseline, with the appearance of the Type 1 pattern of BS in the presence of stimuli such as fever, hypokalemia, hypercalcemia, Vagotonic agents, class I antiarrhythmic drugs, and alcohol and cocaine consumption [2,12]. Given the dynamic character of the ECG in BS and the ability of class I antiarrhythmic drugs to reproduce the diagnostic pattern, the administration of these drugs is used to unmask the pathology in those suspected but with an ECG Normal or suggestive but not diagnostic baseline. The drugs most commonly used for this purpose are Ajmaline, Flecainide and Procainamide [3,12,15]. The development of a Type 1 ECG of BS during the test is a criterion for stopping it, as well as the appearance of a type 2 BS pattern with an ST segment elevation ≥5 mm, aQRS widening ≥130% of its initial value or the development of any arrhythmia. The pharmacological test is only considered positive when there is a conversion to the ECG pattern type 1 in at least 2 right precordial leads [3,21]. First-degree AVB is observed in about 50% of cases of SCR, especially when the SCN5A gene mutation is identified. The “aVR sign” is defined as the presence of a R wave ≥3 mm or a R / q ratio ≥0.75 in the aVR lead and has been associated with an increased risk of ventricular arrhythmias [15], as in the case of our Patient where the sign is appreciated (Figure 2). Hypothetically, the increase in the voltage of the R wave in aVR indicates a greater delay of the ventricular conduction in the RVVD and consequently greater electrical heterogenicity. The BS is definitively diagnosed in patients who documented a Type 1 ECG pattern, either spontaneously or unmasked by class I antiarrhythmics, along with at least one of the following clinical diagnostic criteria: A) Family history data: Sudden Cardiac Detah (SCD) in a family member younger than 45 years; ECG type 1 in relatives. B) Symptoms related to ventricular arrhythmias: syncope, seizures or agonal nocturnal breathing. C) Documented ventricular arrhythmias: PVT or VF [3,12,14]. Patients with BS can also have a higher incidence of supraventricular tachycardias, especially atrial fibrillation (up to 30% of cases) [3]. It is essential to perform a differential diagnosis with certain pathologies or situations that produce alterations with ECG patterns very similar to BS, such as: atypical right bundle branch block, acute myocardial infarction particularly of the RV, pericarditis/acute myopericarditis, pericardial effusion, cocaine intoxication, Pulmonary thromboembolism, aortic dissecting aneurysm, Duchenne muscular dystrophy, Friedreich’s ataxia, left ventricular hypertrophy, RV arrhythmogenic dysplasia, mechanical compression of RVOT, mediastinal tumor, pectus excavatum, post-electrical cardioversion changes, early repolarization (athletes) and Hypothermia [2,3]. All series agree that patients with symptomatic BS have a high arrhythmic risk. Sudden Cardiac Arrest survivors are at high risk for recurrent episodes, fatal or near fatal ventricular arrhythmias (17-62%), and therefore have a class I indication for ICD as secondary prevention. Cardiac syncope is also a marker of high arrhythmic risk (recurrence between 6-9%), also with a class I indication of ICD implantation. The implantation of ICD is considered reasonable in patients affected by BS and who have documented VT, even if it has not resulted in SCA or symptoms (indication class IIa) [3]. The spontaneous type 1 ECG pattern has been identified as an independent predictor of ventricular arrhythmias and clinical ECG monitoring is recommended in order to detect a spontaneous type 1 ECG pattern in patients with BS whose diagnosis has been made by pharmacological test with or without previous symptoms (class IIa indication). Current guidelines consider that the EPS in risk stratification in patients with asymptomatic BS with spontaneous Type 1 ECG is an indication class IIb [3]. The only therapeutic tool that has been proven effective for the prevention and recovery of SCA in patients with BS is the implantation of an ICD. It is also recommended to emphasize the absolute contraindication of the practice of competitive sports, especially sports such as withdrawal, swimming or weight lifting, favoring the use of single-chamber devices (fewer complications), and treating supraventricular arrhythmias [3]. Isoproterenol has proven to be useful for the treatment of electric storms in the context of BS (Class IIa Indication). Quinidine, (Ito and IKr current blocker) prevents VF inducibility during FES and suppresses spontaneous ventricular arrhythmias and is used in patients with ICD with multiple appropriate discharges; or in cases where the ICD implant is contraindicated or as an alternative to it (class IIb indication) [3]. In terms of dysautonomia or its final sign; neurocardiogenic syncope, the association of this with the BS is very possible and frequent in young people, a false impression of the etiology of syncope can lead to it being misdiagnosed therefore underestimating the risk of SCA and not give the right treatment. It is important to consider that the use of a 12-lead ECG is a fundamental diagnostic information source for patients with BS; given that it is a simple, affordable, and mandatory tool in the emergency department. Regardless of the patients’ gender, if they mention a history or presence of vertigo, syncope and/or palpitations and questioning in a directed way a family history of unexplained sudden deaths, an ECG should be obtained. In addition, the ST segment in the BS is highly dynamic, showing a variation of its amplitude and beat-to-beat morphology, and it is mandatory to know the different electrocardiographic data of the BS in order to carry out the algorithm correctly to give an accurate diagnosis and timely treatment, thus avoiding the recurrence of ventricular arrhythmias. The relevance of the case rests on the electrocardiographic changes that occur dynamically during its evolution, on the final appearance of the Type 1 characteristic pattern and its subsequent normalization in the basal state; despite having a low risk EEF for a new ventricular arrhythmia, the patient presented a second event of recovered SCA, which is the determining factor for the implantation of an ICD as the only therapeutic option with a class I indication.
Conclusion
This case illustrates the complexity of the therapeutic decisions in patients who refer symptoms considered as not relevant, so it is urged to be more exhaustive in the interrogation and especially to continuous cardiac monitoring to reduce the rate of sudden death determined as unexplained.
Declarations
Conflict of interests: The authors declare no conflict of interest.
Compliance with ethics requirements: The authors declare no conflict of interest regarding this article. The authors declare that all the procedures and treatments of this study respect the ethical standards in the Helsinki Declaration of 1975, as revised in 2008(5), as well as the national law. Informed consent was obtained from the patient included in the study.
Acknowledgements: The authors thank the Emergency Department of the Hospital General Universitario Joaquín del Valle Sánchez in Torreón, Coahuila, Mexico, for their willingness and collaboration in the development of this study.
References
- Watrich D, Woods R, Steiner I. Brugada syndrome in a young patient with palpitacions. Can J of Emerg Med. 2005; 7: 347-350.
- Berne P, Aguinaga LE, Brugada J. Síndrome de Brugada. Rev Fed Arg Cardiol. 2012; 41: 225-234.
- Meregalli P, Wilde A. Tan H. “Pathophysiological mechanisms of Brugada syndrome: Depolarization disorder, repolarization disorder, or more?.”Cardiovascular Research 2005; 67: 367-378.
- Hermosillo A, Cárdenas M, Márquez M, Vallejo M. El síndrome de Brugada y su relación con el sistema nervioso autónomo y el síncope vasovagal”. Arch Cardiol Méx 2008; 78: 7-10.
- Watanabe A, Fukushima K, Morita H, Miura D, Sumida W, Hiramatsu S, et al. Low-dose isoproterenol for repetitive ventricular arrhythmia in patients with Brugada syndrome. Eur Heart J. 2006; 27: 1579–1583.
- Belhassen B, Glick A, Viskin S. Efficacy of quinidine in high-risk patients with Brugada syndrome. Circulation. 2004; 110: 1731–1737.
- Abud A, Bagattin D, Goyeneche R, Becker C. Failure of cilostazol in the prevention of ventricular fibrillation in a patient with Brugada syndrome, J Cardiovasc Electrophysiol. 2006; 17: 210–212.
- Murakoshi N, Aonuma K. Catheter ablation for ventricular tachyarrhythmia in patients with channelopathies. J Arrhythmia. 2016; 32: 404–410.
- Conte G, Sieira J, Ciconte G, de Asmundis C, Chierchia BB, Baltogiannis G, et al. Implantable cardioverter-defibrillator therapy in Brugada syndrome: A 20-year single-center experience. J Am Coll Cardiol 2015; 65: 879–888.
- Bonny A, Talle MA, Vaugrenard T, Taieb J, Ngantcha M, et al. Inappropriate implantable cardioverter-defibrillator shocks in Brugada syndrome: Pattern in primary and secondary prevention. Indian Pacing Electrophysiol J. 2017; 17: 10–15.
- Sacher F, Probst V, Maury P, Babuty D, Mansourati J, Komatsu Y, et al. Outcome after implantation of a cardioverter-defibrillator in patients with Brugada syndrome: A multicenter study-part 2. Circulation. 2013; 128: 1739–1747.
- Aydin A, Salukhe T, Wilke I, Willems S. Anagement and therapy of vasovagal syncope: A review. World J Cardiol. 2010; 2: 308-315.
- Kossaify A, Kallab K. Neurocardiogenic syncope and associated conditions: Insight into autonomic nervous system dysfunction. Turk Soc Cardiol. 2013; 41: 75-83.
- Picón R, Síndrome de Brugada: Puesta al día. Cardiocore. 2013; 48: 69-74.
- Jaramillo H, Acosta M, Aguilera R, Acosta H, et al. Paciente con síndrome de Brugada con alteración en el gen SCN5A. Comunicación de un caso y revisión de la bibliografía. Med Int Mex. 2008; 24: 243-246.
- Carrillo R, Méndez N, Carillo J, Carrillo L. Sincope neuro cardiogénico una entidad poco frecuente y poco reconocida. Rev Invest Med Sur Mex. 2008; 15: 191-195.
- Khan A, Mittal S, Sherrid M. Current review of Brugada syndrome: From epidemiology to treatment. Anadolu Kardiyol Derg. 2009; 9: 12-16.
- Bravo J, Dificultades en el Diagnóstico y Tratamiento de la Disautonomía. Rev Chil Reumatol. 2012; 28: 152-158.
- Benito B, Brugada J, Brugada R, Brugada P, et al. Síndrome de Brugada. Rev Esp Cardiol. 2009; 62: 1297-1315.
- Babaee M, Aslani A, Aslani A. Significance of cardiac autonomic neuropathy in risk stratification of Brugadasíndrome. Europace. 2008; 10: 821-824.
- Miranda D, Medina F, Salinas J. Sindrome de Brugada: Reporte de un caso y revisión de la literatura. Rev Med Hered. 2009; 20: 225-229.
- Pérez-Riera A, Femenía F, Baranchuk A. Valor del electrocardiograma en el diagnóstico y pronóstico del síndrome de Brugada. Rev Urg Cardiol. 2011; 26: 122-140.