
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Clinical outcomes of stapled hemorrhoidopexy using a novel three-row stapler for grade III/IV hemorrhoids: A single-center experience with literature review
*Corresponding Author : M Sadiq Kazi
Peshant House Hospital, Ahmedabad, Gujarat, India.
Tel: +91 9825234013;
Email: drsadiqkazi11673@gmail.com
Received : Mar 06, 2023
Accepted : Mar 21, 2023
Published : Mar 28, 2023
Archived : www.jcimcr.org
Copyright : © Kazi MS (2023).
Abstract
Background: Stapled hemorrhoidopexy is recognized as one of the transformative minimally invasive treatments for grade III/IV hemorrhoids, refractory to conservative management. The current evidence on the clinical use of the novel circular hemorrhoidopexy stapler is sparse. Moreover, the efficacy of the stapler in terms of long-term prevention of rectal prolapse, recurrence of hemorrhoids, and risks of anorectal fistula has not been envisaged. Hence, we conducted a retrospective single-center study to evaluate the safety and performance of the novel MIRUS™ circular three-row stapler in patients with grade III/IV hemorrhoids.
Methods: Between July 2016 and July 2018, consecutive patients with grade III/IV internal hemorrhoids underwent stapled hemorrhoidopexy at an urban hospital and completed two years’ follow-up. This study is a retrospective analysis of their data. The primary outcome measure was intraoperative bleeding requiring intervention. The secondary outcome measures were the rates of postoperative bleeding, anal stenosis, urine retention, fecal incontinence, and recurrences/reoperations over the two-year follow-up period.
Results: The cohort mostly comprised men (68%) and predominantly included middle-aged individuals (mean age: 42±15 years). Thirteen (17%) and sixty-four patients (83%) presented with grade III and IV hemorrhoids, respectively, with 13% having prior treatment for hemorrhoids. Intraoperative bleeding at the stapled line requiring intervention occurred in three cases (4%). No cases of postoperative complications (urine retention, anal stenosis, or bleeding) or device-related adverse events were reported at discharge. Throughout the two-year follow-up, no symptoms of recurrence and no cases of reoperation were reported.
Conclusions: Stapled hemorrhoidopexy using the novel three-row stapler was safe and effective in this present cohort. Satisfactory clinical safety and efficacy of the circular three-row MIRUS™ Hemorrhoids Stapler has been demonstrated with a moderate sample size. This device would be a clinically useful alternative for performing stapled hemorrhoidopexy to treat grade III/IV hemorrhoids.
Keywords: Hemorrhoids; Hemorrhoidectomy; Three-row stapler; EEA; Double stapling technique; Stapled hemorrhoidopexy.
Abbreviations: DST: Directional Stapling Technique; EEA: End-To-End Anastomosis; MMH: Milligan-Morgan Hemorrhoidectomy; PPH: Procedure For Prolapse And Hemorrhoids; TST: Tissue-Selecting Therapy Stapler.
Citation: Kazi MS. Clinical outcomes of stapled hemorrhoidopexy using a novel three-row stapler for grade III/IV hemorrhoids: A single center experience with literature review. J Clin Images Med Case Rep. 2023; 4(3): 2343.
Introduction
The increasing prevalence of hemorrhoids due to the widespread adoption of sedentary lifestyle and consumption of processed foods poses a challenge for healthcare systems [1]. Consequently, patients with Grade III/IV hemorrhoids require prompt medicative and/or surgical management. Hemorrhoidectomy was the conventional surgical option, which causes severe postoperative pain, patient discomfort, and delayed recovery. It is less frequently used to treat even grade II or grade III hemorrhoids, despite several modifications of the closed and open hemorrhoidectomy techniques. To reduce the patient discomfort, avoid disruption of pelvic floor muscles, and prevent rectal prolapse, minimally invasive methods are warranted that offer better procedural safety and effectively reduce the hemorrhoidal cushions [1,2]. The procedure for Prolapse And Hemorrhoids (PPH) described by Longo gained enormous clinical attention initially due to its minimal invasiveness and early recovery [3]. The procedure also lowered patient discomfort, reduced pain during defecation, and improved the quality of life that enabled faster return to regular activities [1-3].
Numerous studies have described different modifications of Longo’s technique and compared this minimally invasive procedure to the original invasive treatments [2,4-6], while other studies have compared different stapler devices [1,7]. Giuratrabocchetta et al [7] examined the early safety outcomes of two popular staplers, EEA™ Circular Stapler with DST series™ Technology (Medtronic Inc., Minneapolis, MN, US) and Proximate® PPH01 (Ethicon Endo-surgery Inc., Cincinnati, Ohio, US).
A recent single-center, non-randomized study by Wang et al., compared the EEA™ and Proximate® PPH03 staplers (Ethicon Endo-surgery Inc, US) with an age, gender, and grade-matched analysis. Additionally, a new high volume surgical stapling device, the TST STARR Plus (Touchstone International Medical Science Co. Ltd., China) was reported to facilitate enhanced tissue resection during stapled hemorrhoidopexy due to its larger stapler diameter (36 mm) than the diameters of conventional EEA™ and Proximate® PPH staplers [1]. Over the years, stapled hemorrhoidopexy has been recognized as an acceptable treatment option for patients with higher degree hemorrhoids owing to the consistent positive short-term outcomes [1-7]. A few additional devices have been studied including the Premium CEEA 34 plus (curved end-to-end anastomosis) intraluminal stapler (Tyco Healthcare, US), the Ultimate Hemorrhoidal Circular Stapler (Purple Surgical, UK), and the Kangdi Hemorrhoid Circular Stapler (Medtronic Inc., US). However, these devices have not been examined thoroughly for the indication of hemorrhoid treatment.
Recent studies suggest that three-row staplers may offer improved postoperative outcomes than two-row staplers [8,9]. Further, when using the PPH approaches on patients with grade III/IV hemorrhoids who essentially require surgical treatment, the incidence of recurrence, severe postoperative bleeding, and pain/discomfort is reduced [9]. However, more recent evidence on the usage of three-row staplers and their prognostic outcomes is warranted. In our opinion, such evidence would aid in surgical decision-making and facilitate the advancement of hemorrhoid stapling devices. As a result, this would enhance the management of the rising patient burden of hemorrhoidal disease in both developed and low- and middle-income countries. Therefore, we conducted a single-center study that involved the retrospective analysis of patients who underwent stapled hemorrhoidopexy with a novel three-row stapler device, known as MIRUS™ Hemorrhoids Stapler (Meril Endosurgery Pvt. Ltd., India). The device has an additional third row containing a total of 36 staples with a 34 mm diameter. This specialized feature is useful for performing stapled hemorrhoidopexy with the Directional Stapling Technique (DST) and its additional third row is intended to provide excess hemostasis along the dentate line of the suture. Herein, we present the two-year postoperative outcomes of a retrospective, single-arm cohort of patients with grade III and grade IV hemorrhoids that required surgical management.
Methods
The current report includes two components: The first section discusses the outcomes of the data obtained from single-center study and the second section describes the qualitative literature review. We focused our literature search on the current status of hemorrhoidal disease management practices, the prominent devices used, and analyzed the endpoints of studies performing the PPH technique. The search terms utilized in the search string were “staple”, “hemorrhoid”, “hemorrhoidopexy”, “hemorrhoidectomy”, “haemorrhoid”, “EEA”, “surgical”, “stapler”, “haemorrhoid”, “urinary retention”, “fecal incontinence”, “rectal bleeding”, “EEA”, “anorectal”, and other relevant terminology keywords. Boolean operators (AND, OR) were used as necessary. Studies were extracted from reference/bibliography lists if considered relevant for the literature review. Lastly, to extract the latest reports of stapler devices that have not been thoroughly investigated in the clinical settings, a thorough systematic search using public databases and news articles was performed.
Study population and design
The retrospective case series was performed by analyzing the medical records of consecutive patients who underwent the minimally invasive treatment of stapled hemorrhoidopexy at the Peshant House Hospital, Ahmedabad, India between July 2016 and December 2018. These patients underwent stapled hemorrhoidopexy with the circular three-row MIRUS™ Hemorrhoids Stapler (Meril Endosurgery Pvt, Ltd, India) for the treatment of grade III/IV hemorrhoids and completed the two-year follow-up period. All the patients completed the two-year follow-up period.
Ethics statement
The local ethics committee (Registration number: ECR/147/Inst/GJ/2013/RR-19) approved the study and exempted the requirement for written informed consent without any alteration in the management of patients.
Device description
MIRUS™ Hemorrhoids Stapler provides a cutting-edge three-rows approach for performing minimally invasive procedures for prolapsed hemorrhoids. It has a 34 mm three-row circular staggered staple line, circular anal dilator, and a transparent purse-string suture anoscope with the appropriate dentate line markings. Additionally, it has a non-detachable anvil that pro vides support while firing and clamping, which protects from accidental slippage into the anal canal. A larger housing (14 cc) accommodates maximum prolapsed piles mass and delivers optimum resection. The level of compression is controlled using a tissue compression indicator. It provides improved safety, superior hemostasis, and feasibility, resulting in the optimum excision of prolapsed hemorrhoidal tissue. The optimized staple formation technique delivers adjustable height staples, which reduces tissue tension, delivers optimal compression and proper staple line, and ensures an optimal closure height.
Surgical technique
The previously published technique by Longo was adopted [3]. To execute circumferential stapled hemorrhoidopexy, the patient was placed in the lithotomy position under pudendal block anesthesia. Prophylactic doses of intravenous cefoperazone sulbactam (1.5 gm) and metronidazole (500 mg) were administered to each patient at the time of inducing anesthesia. Then, the anal area was dilated and lubricated using a fixator attached with a silk number 1 suture at the 9, 12, 3 and 6 o’clock positions. Later, a circumferential purse-string suture with 2-0 polypropylene (on a 30 mm curved, round-bodied needle given along with stapler pack) was taken starting at 3 o’clock position, at least 1 cm proximal to the largest hemorrhoidal site. It is approximately 3 to 4 cm proximal to dentate line, using the half slit anoscope included with the MIRUS™ stapler pack. A second simple stitch with 2-0 polypropylene was performed at 9 o’clock position at the same level as the purse string to provide counter traction. This ensured that a symmetrical ring of mucosa and submucosa was excised, when the stapler gun was fired. The stapler was opened to its maximum extend and positioned proximal to the purse string, which was then tightened. The stapler was brought closer until the green zone reached and was held for 30 seconds to allow tissue fluid to disperse. Then, the stapler was fired and held in the same position for 60 seconds to ensure hemostasis. Finally, the stapled line was examined for any bleeding. The external hemorrhoidal components were not treated immediately.
Discharge and follow-up
Patients were maintained on postoperative monitoring until they met the criteria for discharge, which included the passage of first bowel motion without any rectal bleeding after surgery. At discharge, oral analgesics, antibiotics, and laxatives were prescribed and patients were recommended to consume a soft diet for two weeks to reduce postoperative rectal discomfort. Patients were followed-up through two years after the surgical procedure. A digital rectal examination and proctoscopy were performed and any incidences of postoperative bleeding per rectum were examined throughout the follow-up period.
Outcome measures
The primary outcome measure was intraoperative staple line bleeding that required immediate surgery. The secondary outcome measures included the rates of postoperative complications (bleeding, anal stenosis, residual skin tags and prolapse, urine retention, and fecal incontinence), incidence of stapler misfire/malfunction, length of hospital stay, operation time, and recurrence of hemorrhoid symptoms/re-operations through two years follow-up. We also recorded the number of adverse or serious adverse events and the clinical course of any cases of adverse or serious adverse events through the two years follow-up.
Statistical analysis
The baseline characteristics were summarized as mean with Standard Deviation (SD). Primary outcome measures were presented as the frequency and percentages. All statistical analysis was performed using SPSS Statistics version 21.0 (IBM Corporation, Armonk, New York, United States).
Results
Baseline characteristics
This single-center cohort included 77 patients (mean age: 42 ± 15 years; 68% men, n=52). Table 1 presents the baseline characteristics of the whole study cohort. The majority of patients presented with grade IV hemorrhoids (n=64; 83%), while 13 (17%) had grade III hemorrhoids, and 10 (13%) had previously undergone treatment for hemorrhoids. Notably, patients had experienced rectal bleeding without stools (69%), pain (64%), burning (30%), and hematochezia during defecation (17%). Some patients also experienced anal protrusion (13%) and severe anal protrusion during defecation (22%); we noted the presence of abnormal nodules in 38% patients, and 13% had a history of Doppler-guided surgery. Figure 1 depicts a representative image of a patient prior to the stapled hemorrhoidopexy procedure. The hemorrhoidal cushions are visible along with protrusion of the anal tissue.
Table 1: Baseline characteristics of the whole study cohort.
| Variables | Mean ± SD or N (%) |
|---|---|
| Age group (years) | |
| Below 20 | 3 (4) |
| 20–39 | 32 (41) |
| 40–59 | 33 (43) |
| 60 and older | 9 (12) |
| Sex | |
| Male | 52 (68) |
| Female | 25 (32) |
| Grade of hemorrhoids | |
| Grade III | 13 (17) |
| Grade IV | 64 (83) |
| Medical history | |
| Rectal bleeding without stools | 53 (69) |
| Rectal bleeding during defecation | 13 (17) |
| Pain | 49 (64) |
| Presence of nodules | 29 (38) |
| Burning | 23 (30) |
| Protrusion at anus | 10 (13) |
| Protrusion at anus during stools | 17 (22) |
| Doppler-guided surgery | 10 (13) |
SD: Standard deviation
Postoperative outcomes
As regards the evaluation of the primary outcome measure, three (4%) patients with grade IV hemorrhoids experienced an intraoperative bleeding at the stapled line and required immediate suturing using Vicryl 2-0 to achieve hemostasis. The analysis of the secondary outcome measure revealed no instances of postoperative complications (bleeding, anal stenosis, residual skin tags and prolapse, urine retention, and fecal incontinence) throughout the two-year follow-up. In addition, there were no cases of hemorrhoid recurrence over the two-year follow-up period. Table 2 summarizes the intra operative and postoperative clinical outcomes of all patients.
Table 2: Intra operative and postoperative outcomes.
| Variable | Outcome, Mean ± SD or n (%) |
|---|---|
| Intra-operative bleeding event (s) | 3 (4) |
| Mean operation time (min) | 35± 3 |
| Mean hospital stay (days) | 1.06 ± 0.57 |
| Incidence of stapler misfire | 0 (0) |
| Incidence of stapler malfunction | 0 (0) |
| Device success | 100% |
| Post-operative complications | 0 (0) |
| Recurrence rate at two years | 0 (0) |
| Size of stapler used | 34 mm |
SD: Standard deviation
The average operation time was 35 ± 3 minutes, whereas the average hospital stay duration was 1.06 ± 0.57 days. There were no instances of adverse or serious adverse events related to the study device, including stapler misfire or malfunction. Hence, the procedural success was deemed satisfactory. Table 3 presents the intraoperative characteristics of the three patients who required additional medical attention for intraoperative staple line bleeding.
Table 3: Characteristics of patients who required surgical intervention for intra-operative bleeding.
| Variables | N =3, Mean ± SD or N (%) |
|---|---|
| Gender | Male |
| Age, years | 56 ± 27 |
| Grade of haemorrhoid | Grade IV |
| Heart rate, bpm | 80 ± 8 |
| Systolic blood pressure, mm/Hg | 121 ± 2 |
| Diastolic blood pressure, mm/Hg | 74 ± 7 |
| Post-operative complications/recurrence | 0 (0%) |
SD: Standard deviation
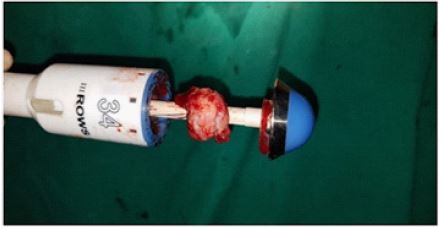
No cases of prolonged hospital stay were reported, which indicates the absence of immediate device-related complications. None of the patients experienced postoperative complications. Figure 2 is an image of excised anorectal mucosa showing an intact mass-like appearance on the three-row stapler.
Notably, throughout the two years follow-up, no instances of postoperative bleeding, anal stenosis, residual skin tags and prolapse, urine retention, and fecal incontinence were reported. Further, throughout the two-year follow-up period no patients showed symptoms of recurrence. In addition, no cases of reoperation or late adverse or serious adverse events were recorded throughout the two-year follow-up period. Figure 3 shows the postoperative image in which the hemorrhoidectomy wound in the anoderm is visible.


Results of the qualitative literature review
For the qualitative literature review, 8 papers were analyzed that included systematic reviews, observational studies, randomized clinical trials, and retrospective case series studies [5,6,8,9,10-14]. A network meta-analysis performed by Zhang et al. compared the original PPH technique with Milligan-Morgan Hemorrhoidectomy (MMH) and tissue-selecting Therapy Stapler (TST) technique. The results of this meta-analysis revealed that fewer studies considered urinary retention as the primary endpoint (n=14; 2104 patients) and the PPH group had lower rates of urinary retention and fecal incontinence than the MMH group. Furthermore, the authors explained that preserving the anal cushions and anal canal reduces the postoperative pain score following hemorrhoid treatment [6]. In several trials, the outcomes of stapled hemorrhoidopexy have been compared to those of Ferguson’s closed hemorrhoidectomy technique and MMH procedure. The meta-analysis of several randomized controlled trials concluded that with stapled hemorrhoidopexy, the in-hospital stay duration was indeed shorter (weighted mean difference = -1.02 days (95% confidence interval = -1.47 to -0.57, p=0001). The meta-analysis further reported shorter procedural times including a shorter anesthesia duration and lower postoperative pain scores for the PPH technique in comparison to the conventional MMH procedure [10]. The reduction in postoperative discomfort during defecation was noted for the PPH technique, which was comparatively higher following the MMH technique, which is a significant finding of this meta-analysis. The return to normal activity levels was noted to be significantly higher following the PPH technique than that after the MMH technique. An interesting study by Iida Y and colleagues compared 2 hemorrhoidopexy staplers (PPH-LA01, PPH-LA03), with two other prominent techniques, MMH and sclerotherapy, showed higher recurrence rates of hemorrhoids with prolapse following stapled hemorrhoidopexy using PPH-LA01 and PPH-LA03 staplers (Ethicon Endo-surgery Pvt. Ltd, Cincinnati, Ohio, US) [9]. Such relapse cases required further treatment with rubber band ligation or MMH. This study concluded that creating a rectal an astomosis at a lower site than that advised in the original Longo technique was possible with the PPH-LA03 stapler. This technique further reduced the incidence of recurrence, major postoperative bleeding, and postoperative pain in comparison to MMH and PPH technique with the PPH01 stapler. Iida et al. further stated that the postoperative recurrence rate after stapled hemorrhoidopexy with the Ethicon PPH-LA03 stapler is as low as that with MMH until up to 16 years [9].
The long-term outcomes of stapled hemorrhoidopexy versus open hemorrhoidectomy were compared between 1998–2008 and 2009–2019 in the systematic review conducted by Ruanet al. [11]. It was concluded that stapled hemorrhoidopexy had considerable long-term safety for up to two years but is less cost-effective, and provides fewer years of quality-adjusted lifespan than open or closed hemorrhoidectomy [11]. Therefore, it is less frequently advised as a treatment option for the surgical management of grade III/IV hemorrhoids. Over time, the outcomes of stapled hemorrhoidopexy has not improved as anticipated. Moreover, a thorough analysis of various randomized clinical trials comparing stapled hemorrhoidopexy with the traditional surgeries revealed that the improvement in the procedural outcomes has reached a plateau. In addition, we identified other minimally invasive procedures that have been used such as transanal haemorrhoidal dearterialization, with and without Doppler guidance, the hemorrhoid laser procedure, and a tissue selection therapy stapler technique [5,10,12-14].
Discussion
Symptomatic hemorrhoidal illness affects the quality of life to the extent that patients develop the requirement of assisted mobility. This anorectal disease, particularly of grade IV is common among women with high-risk pregnancies, terminally ill patients such as those with cancer, paralysis, or patients having significant physical debilitation.
The treatment of hemorrhoids has benefitted immensely from the development of transformative devices, such as hemorr hoidopexy staplers, which were introduced into routine practice in the last decade. Hemorrhoidopexy staplers have enabled the minimally invasive treatment of the hemorrhoidal cushions without worsening of postoperative discomfort and with spinal anaesthesia alone. The recent reports of stapled hemorrhoidopexy have reported its clinical benefits including shorter hospital stays, lower volumes of intraoperative and postoperative bleeding, and reduced postoperative pain and discomfort [1,2,5,7,14]. Because of the encouraging data available for the PPH staplers, stapled hemorrhoidopexy has become a preferred treatment for grade III/IV hemorrhoids.
In our first-hand experience, grade IV haemorrhoids were more incident than grade III hemorrhoids, and the mid-term postoperative outcomes with a three-row stapler were acceptable. The short-term outcomes of this device had been investigated in a previous high-volume single-center study by Gupta et al [8]. Moreover, given that prolonged hospitalization could be a consequence of severe postoperative pain or adverse events, the incidence of urine retention and the length of stay were independently assessed as secondary endpoints. Our data further demonstrated the safety and performance of a new three-row stapler in the treatment of prolapsed hemorrhoids. By offering secure staple formation and improved hemostasis, the results of the present study indicated the clinical feasibility of study device for stapled hemorrhoidectomy.
The incidence of bleeding during stapled hemorrhoidectomy has been a significant cause of patient morbidity and delayed recovery. When performing the Longo approach, the stapler is inserted in an intact bowel lumen and it cuts across a well-vascularized tissue including the sub mucosal blood vessels under relatively high pressure [3]. Intraoperative staple line bleeding has been linked to a higher risk of major intraoperative bleeding that requires immediate medical intervention. In our study sample, the number of patients who required additional surgical intervention was lower (n=3) than that reported earlier [15-17]. There were no cases of postoperative bleeding; taken together an acceptable safety profile was demonstrated. This investigation highlights the clinical utility of this procedure for standard office-based treatment. An earlier study that compared the use of a two-row device (Proximate® PPH) with the three-row (MIRUS™) hemorrhoids stapler found that the PPH group had a higher rate of hemostatic suturing (n=39 of 108 patients, 36.11%) than MIRUS™ group (n=27 of 116 patients, 23.3%) [8].
Nevertheless, there is substantial clinical evidence to support that triple-line stapling with three-row staplers performed better than double-line stapling with two-row staplers for the treatment of prolapsing hemorrhoids, especially to prevent recurrences for at least 5 years [9]. In a recent randomized clinical trial, the short-term outcomes of a modified hemorr hoidal transanal arterial ligation technique and stapled hemorrhoidopexy method were compared at Putuo Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai [18]. The study found similar trends in the reduction of postoperative pain and prevention of symptom recurrence using a disposable PAH 32 stapler (Brightness Medical Device Co., China) for the stapled surgery (hematochezia, prolapse, and rectal pain).
Limitations
Although the clinical performance of study device has been evaluated, there is currently inadequate evidence to ascertain its long-term safety and performance. Larger and long-term trials with prospectively enrolled cohorts and a randomized controlled study design would be necessary to reaffirm the device efficacy. The assessments may include digital rectal examinations, thorough clinical evaluation, and the presence of anal pain, soiling, perianal itching, and other recurring symptoms at regular intervals.
Conclusions
The current study reports acceptable clinical outcomes of stapled hemorrhoidopexy with the three-row stapler device in a single-arm cohort with no recurrences observed after two years postoperatively. Our data and analysis advocate the use of a stapled hemorrhoidopexy technique with three-row stapling for the management of grade III and IV hemorrhoids. The selection of the surgical procedure should be determined by the patient’s ability to undergo an office-based procedure with local anesthetic or a procedure that necessitates complete sedation and if the patient has bleeding of hemorrhoids. Currently, it is recommended that the potential prognostic characteristics seen after various surgical treatments for hemorrhoids should be thoroughly explained to the patients in advance. Appropriate medical management and dietary modifications should be implemented to enable higher patient satisfaction following stapled hemorrhoidopexy. A three-row stapler is relatively beneficial in alleviating patient discomfort and enabling faster return to regular activities.
Declarations
Conflict of interest: The author declares no conflict of interest.
Competing interests: The authors declare there are no financial conflicts of interest to disclose.
Ethical consent: Waiver for the written informed consent has been received from the ethics committee.
Informed consent: Informed consent was obtained from all individual participants included in the study.
Consent for publication: I hereby give our consent for publication.
Author contributions: Dr. M. Sadiq Kazi was responsible for the conception and design, analysis and interpretation of the data, the drafting of the paper or revising it critically for intellectual content. The author has approved the final version of the manuscript to be published.
Data availability statement: The data that support the findings of this study are available on request from the corresponding author, Dr M. Sadiq Kazi, upon reasonable request.
References
- Wang TH, Kiu KT, Yen MH, Chang TC. Comparison of the short-term outcomes of using DST and PPH staplers in the treatment of grade III and IV hemorrhoids. Sci Rep. 2020; 10: 5189.
- Watson AJ, Cook J, Hudson J, Kilonzo M, Wood J, Bruhn H, et al. A pragmatic multicentre randomised controlled trial comparing stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease: the eTHoS study. Health Technol Assess. 2017; 21: 1-224.
- Longo A. Treatment of Hemorrhoids Disease by Reduction of Mucosa and Hemorrhoidal Prolapse with a Circular Suturing Device: A New Procedure. In: Proceedings of the 6th World Congress of Endoscopic Surgery, Rome (Monduzzi Publishing Co.) 1998; 777-784.
- Lin HC, He QL, Shao WJ, Chen XL, Peng H, et al. Partial Stapled Hemorrhoidopexy Versus Circumferential Stapled Hemorrhoidopexy for Grade III to IV Prolapsing Hemorrhoids: A Randomized, Noninferiority Trial. Dis Colon Rectum. 2019; 62: 223-233.
- Ho KS, Ho YH. Prospective randomized trial comparing stapled hemorrhoidopexy versus closed Ferguson hemorrhoidectomy. Tech Coloproctol. 2006; 10: 193-197.
- Zhang G, Liang R, Wang J, Ke M, Chen Z, et al. Network meta-analysis of randomized controlled trials comparing the procedure for prolapse and hemorrhoids, Milligan-Morgan hemorrhoidectomy and tissue-selecting therapy stapler in the treatment of grade III and IV internal haemorrhoids (Meta-analysis). Int J Surg. 2020; 74: 53-60.
- Giuratrabocchetta S, Pecorella G, Stazi A, Tegon G, De Fazio M, Altomare DF, et al. Safety and short-term effectiveness of EEA stapler vs PPH stapler in the treatment of degree III haemorrhoids: Prospective randomized controlled trial. Colorectal Dis. 2013; 15: 354-358.
- Gupta P, Kundra DN, Khanna A, Aggarwal A, Kapoor K, et al. Our initial experience of three versus two rows circular stapler devices for stapled hemorrhoidopexy: A single institution review of 224 cases. Int Surg J. 2020; 7: 685–688.
- Iida Y, Saito H, Takashima Y, Saitou K, Munemoto Y, et al. Procedure for Prolapse And Hemorrhoids (PPH) with low rectal an astomosis using a PPH 03 stapler: Low rate of recurrence and postoperative complications. Int J Colorectal Dis. 2017; 32: 1687-1692.
- Nisar PJ, Acheson AG, Neal KR, Scholefield JH, et al. Stapled hemorrhoidopexy compared with conventional hemorrhoidectomy: Systematic review of randomized, controlled trials. Dis Colon Rectum. 2004; 47: 1837-1845.
- Ruan QZ, English W, Hotouras A, Bryant C, Taylor F, et al. A systematic review of the literature assessing the outcomes of stapled haemorrhoidopexy versus open haemorrhoidectomy. Tech Coloproctol. 2021; 25: 19-33.
- Ratto C, Donisi L, Parello A, Litta F, Doglietto GB, et al. Evaluation of transanal hemorrhoidal dearterialization as a minimally invasive therapeutic approach to hemorrhoids. Dis Colon Rectum. 2010; 53: 803-811.
- Longchamp G, Liot E, Meyer J, Toso C, Buchs NC, et al. Non-excisional laser therapies for hemorrhoidal disease: A systematic review of the literature. Lasers Med Sci. 2021; 36: 485-496.
- Festen S, van Hoogstraten MJ, van Geloven AA, Gerhards MF, et al. Treatment of grade III and IV haemorrhoidal disease with PPH or THD. A randomized trial on postoperative complications and short-term results. Int J Colorectal Dis. 2009; 24: 1401-1405.
- Moore JS, Seah AS, Hyman N. Management of hemorrhoids in unusual circumstances. Semin Colon Rectal Surg. 2013; 24: 108-111.
- Ceci F, Picchio M, Palimento D, Calì B, Corelli S, et al. Long-term outcome of stapled hemorrhoidopexy for Grade III and Grade IV hemorrhoids. Dis Colon Rectum. 2008; 51: 1107-1112.
- Lee KC, Chen HH, Chung KC, Hu WH, Chang CL, et al. Meta-analysis of randomized controlled trials comparing outcomes for stapled hemorrhoidopexy versus Liga Sure hemorrhoidectomy for symptomatic hemorrhoids in adults. Int Surg J. 2013; 11: 914-918.
- Yang H, Shi Z, Chen W, Chen T, Ding P, et al. Modified ligation procedure for prolapsed haemorrhoids versus stapled haemorrhoidectomy for the management of symptomatic haemorrhoids (MoLish): randomized clinical trial. BJS Open. 2022; 6: zrac064.