
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Surgical treatment of solitary axillary schwannoma
Alessandro Paganini1; Vito D’andrea2; Eleonora Rapanotti1; Paolo Missori3*
1Department of General Surgery and Surgical Specialties “Paride Stefanini”, Policlinico Umberto I, Sapienza University of Rome, Italy.
2Department of Surgical Sciences, Policlinico Umberto I, Sapienza University of Rome, Italy.
3Department of Human Neurosciences, Neurosurgery, Policlinico Umberto I, Sapienza University of Rome, Italy.
*Corresponding Author : Paolo Missori, MD
Neurochirurgia, Viale del Policlinico, 155, 00161 Roma, Italy.
Tel: 0039- 0649979136, Fax: 0039- 0649979136;
Email: missorp@yahoo.com
ORCID: 0000-0003-2056-0104
Received : Mar 08, 2023
Accepted : Mar 23, 2023
Published : Mar 30, 2023
Archived : www.jcimcr.org
Copyright : © Missori P (2023).
Abstract
Solitary axillary schwannomas are very rare lesions, with just over 20 cases previously reported in the literature. Here we describe a patient with a symptomatic solitary axillary schwannoma. Total removal was successful, without complication. In patients with increasingly symptomatic axillary schwannoma, early surgical removal is recommended to avoid further neurological deficit, and to achieve the best results.
Keywords: Axillary; Breast; Misdiagnosis; Schwannoma; Surgery.
Citation: Paganini A, Andrearea VD, Rapanotti E, Missori P, et al. Surgical treatment of solitary axillary schwannoma. J Clin Images Med Case Rep. 2023; 4(3): 2348.
Introduction
Solitary axillary schwannomas are very rare lesions. Just over 20 cases have been reported in the literature, and many of these patients are adult females with a previous history of breast cancer and radiological misdiagnosis of a secondary lesion. Surgical treatment is feasible but difficult due to frequent adhesions of the tumor to vascular structures and the brachial plexus’ nerve fibers. Here we report the case of a young female with an increasingly symptomatic solitary axillary schwannoma.
Case presentation
A 55-year-old female with negative pathological history was admitted to the hospital with a three-month history of right axillary pain, sometimes located on the right arm and hand, particularly on the ulnar side. For over one year, she had noticed a progressive small swelling in the middle of the right axillary region, and tingling on the medial side of the right hand.
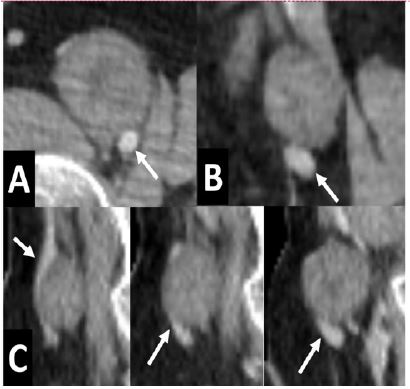
Examination revealed a firm and slightly tender lump, firmly attached to the deep structures. Neurological assessment revealed slightly decreased grip strength, with a positive ulnar nerve test and reduced tactile sensitivity in the C7 territory. Full-body CT scan with contrast dye showed a single roundish lesion of 37 × 27 mm, immediately adjacent to the right axillary artery, with no other lesions elsewhere (Figure 1). Electromyography confirmed slight C7 nerve dysfunction. Needle biopsy proved a schwannoma.
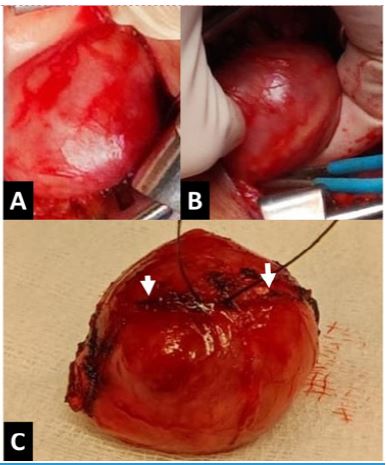
Through a transverse skin incision, an encapsulated lesion was exposed, with a nerve sticking out from the medial and lateral ends. Some adherent flat nerve fibers were visible on the superior surface of the lesion. The axillary artery was detached, and marginal resection with a bipolar coagulation forceps was performed to avoid neural damage (Figure 2). Ultimately, the lesion was completely removed, leaving the spinal nerve thinned out but intact.
Histological evaluation confirmed a schwannoma. The postoperative course was uneventful. The patient complained of a tactile sensitivity deficit in the last two fingers. After six months, the pain has been eliminated, but the neurological hand strength and sensitivity have not yet improved. It is recommended that the patient continue to undergo clinical and radiological breast examinations.
Discussion
The literature reports that most lesions of the axillary nerve are caused by traumatic injury [1]. Sporadic peripheral nerve sheath tumors in the axilla are much less common, with peripheral nerve schwannomas showing a prevalence of only 4% among adults [2]. To date, just over 20 cases of axillary nerve schwannomas have been reported in the literature, and more than one-third of the affected patients are adult females with a history of synchronous or metachronous breast cancer [3-10]. With no family history of von Recklinghausen’s disease the schwannoma mimics an axillary metastasis and misdiagnosis can occur [3-10]. Our presently reported patient does not have a history of breast cancer, but we advise a careful clinical follow-up, since we cannot exclude the possibility that a new tumor may arise in another organ.
If a patient experiences early symptoms from a brachial plexus nerve schwannoma, early surgical removal should be promptly considered before damage of the nerve bundles becomes irreversible. Careful radiological evaluation of the vascular and nervous relationships enables assessment of surgical risks, and planning of the best surgical strategy. In our patient, the identification of a thinned nerve on the tumor surface allowed us to perform marginal resection with bipolar coagulation forceps, leaving the axillary nerve intact as much as possible. After surgical treatment, the patient complained of persistent tactile sensitivity and motor deficits, which have not yet improved at short-term follow-up. In conclusion, early surgical removal of an axillary schwannoma is recommended, to avoid further neurological deficit and achieve the best possible clinical results.
Declarations
Data availability: Raw data were generated at the Policlinico Umberto I, “Sapienza” University of Rome Hospital. Further inquiries can be directed to the corresponding author.
Conflicts of interest: The authors declare that they have no competing interest.
Data availability statement: Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Funding statement: None.
Conflict of interest disclosure: None.
Ethics approval statement: This case report does not need ethical approval.
Patient consent statement: A written consent form has been signed by the patient for the publication and we retain the original written consent form and provide it to the Publisher if requested.
References
- M Artico, M Salvati, V D’Andrea, EO Ramundo, F Nucci, et al. Isolated lesion of the axillary nerve: Surgical treatment and outcome in 12 cases. Neurosurgery. 1991; 29: 697-700.
- J Zipfel, M Al-Hariri, I Gugel, A Grimm V Steger, et al. Surgical Management of Sporadic Peripheral Nerve Schwannomas in Adults: Indications and Outcome in a Single Center Cohort. Cancers (Basel). 2021; 13: 1017.
- H Kumagai, K Takehana, Y Shioi, C Tono. Axillary schwannoma mimicking lymph node metastasis-associated breast cancer: A case report. Surg Case Rep. 2022; 8: 135.
- M Duehrkoop, B Frericks, C Ankel, C Boettcher, W Hartmann, et al. Two case reports: Breast schwannoma and a rare case of an axillary schwannoma imitating an axillary lymph node metastasis. Radiol Case Rep. 2021; 16: 2154-2157.
- H Ramdani, S El Haddad, L Chat, A Souadka, N Allali. Axillary schwannoma mimicking a breast cancer lymph node metastasis. Breast J. 2021;27: 387-388.
- RA da Costa Vieira, LC Navarro de Oliveira, RM Martins, PC Falcão-Junior. Schwannoma associated with breast cancer mimicking axillary metastasis. Breast J. 2021; 26: 2412-2413.
- A Lynch, G Peters. Brachial plexus tumor simulating an axillary metastasis from breast carcinoma. Radiol Case Rep. 2015; 7: 712.
- GR Boto, A Moreno-Gutiérrez, R Gutiérrez-González, AVillar-Martín, LA Arraez-Aybar, J Serrano Hernando, et al. Neurinoma del plexobraquialsimulando metastasis de adenocarcinoma de mama [Schwannoma of the brachial plexus resembling a breast adenocarcinoma metastasis]. Medicina (B Aires). 2011; 71: 459-461.
- N Fujiuchi, T Saeki, H Takeuchi, H Sano, T Takahashi, et al. A false positive for metastatic lymph nodes in the axillary region of a breast cancer patient following mastectomy. Breast Cancer. 2011: 18:141-144.
- M Nakamura, S Akao. Neurilemmoma arising in the brachial plexus in association with breast cancer: Report of case. Surg Today. 2000; 30: 1012-1015.