
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Giant cell tumor of femur transformation after radiation and
denosumab: A rare case of lymph node metastasis
Qinglian Tang; Huaiyuan Xu; Jinchang Lu; Hao Wu; Mi Zhou; Jiayu Gu; Yingchun Zhang*; Jin Wang*
State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou 510060, P. R. China.
*Corresponding Author : Yingchun Zhang & Jin Wang
State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou 510060, P. R. China.
Email: tangql@sysucc.org.cn
Received : Feb 07, 2023
Accepted : Apr 05, 2023
Published : Apr 12, 2023
Archived : www.jcimcr.org
Copyright : © Zhang Y & Wang J (2023).
Abstract
Background: Malignant transformation of Giant Cell Tumor (GCT) is not common. We report a case of GCT transformation after radiation and denosumab with iliac lymph node metastasis.
Case presentation: A 31-year-old man received surgery for his lesion in the left femur in 2010, without histological diagnosis. Eleven years later (2021), his tumor recurred. He received curettage and cement augmentation in another hospital. Unfortunately, he got second recurrence one year later (2021). He received biopsy and found no evidence of malignant transformation. Radiation (60 Gy/20 F) was prescribed for him with denosumab injection per month. However, he had knee pain which was more severe at night. He came to our department (2022) and ordered an MR scan for his left leg. MR imaging revealed soft tissue mass from distal femur. A Multidisciplinary Team (MDT) discussion was launched with the conclusion of suspected malignant transformation. Afterwards, the entire lesion was resected and reconstructed with a hinged prosthesis. The entire bone lesion was sent for histologic examination and malignant transformation was noticed. Two months later, a lump was palpated at his left iliac region and MR reveled multiple lymph nodes in the inguinal region. Ultrasound-guided needle biopsy confirmed lymph node metastasis. Chest and abdomen and pelvis CT did not find another metastasis.
Conclusions: Malignant transformation of recurrent GCT can occasionally occur after administration of radiation and denosumab. Malignant transformation should be suspected if the symptom did not alleviate after treatment. Transformed GCT can sometimes develop lymph node metastasis which is detected by physical examination and appropriate imaging studies.
Keywords: Femur; Giant cell tumor; Radiation; Denosumab; Metastasis; Lymph node.
Citation: Tang Q, Xu H, Lu J, Zhang Y, Wang J, et al. Giant cell tumor of femur transformation after radiation and denosumab: A rare case of lymph node metastasis. J Clin Images Med Case Rep. 2023; 4(4): 2368.
Background
Malignant transformation of Giant Cell Tumor (GCT) of bone is uncommon [1,2]. It’s still unclear the exact rate of malignant transformation after radiation and long-term administration of denosumab. According to the literature, lymph node metastasis of GCT is rare [3,4]. We report a case of recurrent GCT transformation after radiation and denosumab. Also, this patient developed lymph node metastasis, which is rare among literatures.
Case presentation
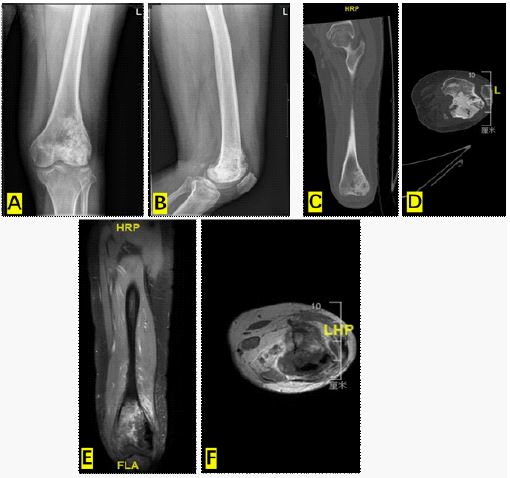
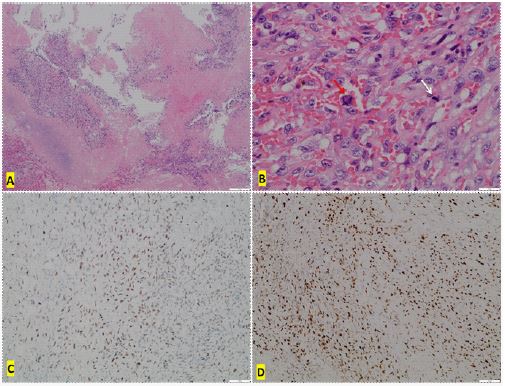
A 31-year-old Chinese man received surgery for his lesion in the left femur in 2010, without histological diagnosis. He had no family history of cancer. Eleven years later (2021), his tumor recurred. He received curettage and Polymethyl Methacrylate (PMMA) augmentation in another hospital. Unfortunately, he got second recurrence one year later (2021). He received biopsy and found no evidence of malignant transformation. Radiation (60 Gy/20 F) was prescribed for him with denosumab injection per month at local hospital. However, he had knee pain which was more severe at night. He was referred to our institution (2022) and ordered Magnetic Resonance (MR) imaging for his left leg. MR imaging revealed soft tissue mass from distal femur (Figure 1). A Multidisciplinary Team (MDT) discussion was launched with the conclusion of suspected malignant transformation. Afterwards, the bone lesion was resected and reconstructed with a hinged prosthesis. The entire bone lesion was sent for histologic examination and malignant transformation was noticed (Figure 2). Microscopic evaluation of the tumor revealed massive necrosis. The existing tumor cells were polygonal, spindle and eosinophilic, with plenty cytoplasm. The nuclei were enlarged and some vacuole nuclei were seen. Obvious nucleolus and mitosis were noticed. Pathological mitoses were also present. The tumor cells were H3.3G34 W (+) by Immunohistochemistry (IHC) staining. Ki-67 Proliferation Index was approximately 70%.
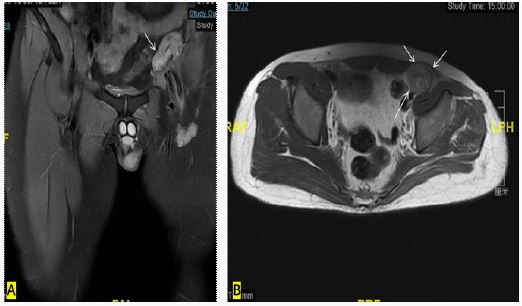
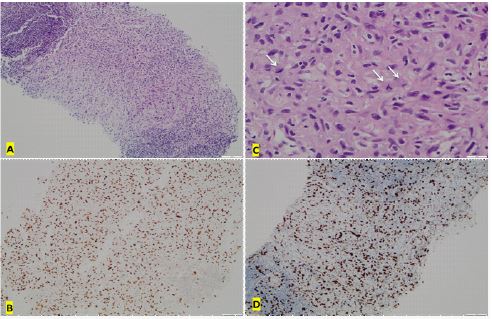
Two months later, a lump was palpated at his left iliac region and MR revealed multiple lymph nodes in the inguinal region (Figure 3). Ultrasound-guided needle biopsy confirmed lymph node metastasis (Figure 4). Chest and abdomen and pelvis CT did not find another metastasis.
Discussion
Giant Cell Tumor of Bone (GCTB) is a benign neoplasm with locally aggressive behavior. Surgery is the main treatment of choice for appendicular GCT. Local recurrence rate in the extremityis 15%-22% after curettage surgery with PMMA [5]. This case has second recurrences and biopsy is performed to evaluated the possibility of malignant transformation. No transformed cells were detected from the biopsy tissue.
Spontaneous malignant transformation of GCTB has been reported [1,6]. However, the exact incident of spontaneous malignant transformation is unknown. Radiation therapy is a potential risk factor for malignant transformation. Radiation Therapy (RT) is less effective for locally recurrent disease than the primary one [7,8]. In most circumstance, RT is considered only after failure of other treatment options.
Denosumab is approved for treatment of patients whose GCTB is unresectable or when surgery is likely to result in unacceptable morbidity. In a study [9], malignant transformation of benign GCTB was noticed in four patients (1%).
To date, it is not clear whether the rate of transformation is increased when RT is combined with denosumab. We presented here the case in which transformation arise post RT and denosumab. Patients must be aware that there is still the potential for RT and denosumab to induce malignant transformation, even with the advent of new RT technology. In clinical setting, if the patient experiences an unrelieved pain after RT or denosumab, malignant transformation should be suspected and further investigations are warranted. As presented in this case, the patient had intractable knee pain after RT and denosumab. When a transformed GCT is suspected, MDT discussion is recommended. Our MDT discussion pointed out a high possibility of malignant transformation. We performed surgical resection of the tumor and malignant transformation was finally confirmed. H3F3A mutations can help diagnose GCTB, but cannot entirely exclude transformed GTCB [10-12]. This case showed G34W mutation even after malignant transformation.
Lymph nodal involvement is very rare in GCT and is usually associated with pulmonary metastasis. The GCT of this patient here metastasized to external iliac lymph nodes without lung metastasis. We resected the external iliac lymph nodes and the final histopathology showed lymph nodal involvement. The prognosis of GCT with sole lymph node metastasis is unknown due to the very limited clinical cases.
Conclusion
In the present case, transformation of recurrent femur GCT developed after radiation and denosumab. Also, the disease spread to lymph node without lung involvement, which is very rare among literatures. Awareness of GCT transformation and lymph node metastasis is essential, and careful long-term follow-up is needed for a transformed GCT.
References
- Grote HJ, et al. Spontaneous malignant transformation of conventional giant cell tumor. Skeletal Radiol. 2004; 33: 169-175.
- Anract P, et al, Malignant giant-cell tumours of bone. Clinico-pathological types and prognosis: A review of 29 cases. Int Orthop. 1998; 22: 19-26.
- Aftab K, B Umar. Giant cell tumor of bone with lymph node metastases: A rare presentation. Indian J Pathol Microbiol. 2011; 54: 396-397.
- Viswanathan S NA. Jambhekar, Metastatic giant cell tumor of bone: Are there associated factors and best treatment modalities? Clin Orthop Relat Res. 2010; 468: 827-833.
- Klenke FM, et al. Giant cell tumor of bone: risk factors for recurrence. Clin Orthop Relat Res. 2011; 469: 591-599.
- Domovitov SV, JH Healey. Primary malignant giant-cell tumor of bone has high survival rate. Ann Surg Oncol. 2010; 17: 694-701.
- Caudell JJ, et al. Radiotherapy in the management of giant cell tumor of bone. Int J Radiat Oncol Biol Phys. 2003; 57: 158-165.
- Miszczyk LJ Wydmanski, J Spindel. Efficacy of radiotherapy for giant cell tumor of bone: Given either postoperatively or as sole treatment. Int J Radiat Oncol Biol Phys. 2001; 49: 1239-1242.
- Chawla S, et al, Denosumab in patients with giant-cell tumour of bone: A multicentre, open-label, phase 2 study. Lancet Oncol. 2019; 20: 1719-1729.
- Presneau N, et al, Diagnostic value of H3F3A mutations in giant cell tumour of bone compared to osteoclast-rich mimics. J Pathol Clin Res. 2015; 1: 113-123.
- Gomes CC, et al, The highly prevalent H3F3A mutation in giant cell tumours of bone is not shared by sporadic central giant cell lesion of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014; 118: 583-585.
- Luke J, et al, H3F3A mutation in giant cell tumour of the bone is detected by immunohistochemistry using a monoclonal antibody against the G34W mutated site of the histone H3.3 variant. Histopathology. 2017; 71: 125-133.