
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
“E-sign” in imaging: Debunking congenital bipartite
from isolated medial cuneiform fracture
Richa Yadav*; SSK Venkatesh; Sivanand Gamangatti
Department of Radiodiagnosis, All India Institute of Medical Science, New Delhi, India.
*Corresponding Author : Richa Yadav
Department of Radiodiagnosis, All India Institute of Medical Science, New Delhi, India.
Ph: 8826067121;
Email: shinericha@gmail.com
Received : Mar 22, 2023
Accepted : Apr 21, 2023
Published : Apr 28, 2023
Archived : www.jcimcr.org
Copyright : © Yadav R (2023).
Abstract
Bipartite medial cuneiform is a rare congenital normal variant at the Lisfranc joint that is a potential trap for isolated medial cuneiform fracture or midfoot injury. Misinterpretation of imaging may lead to unnecessary surgical intervention. The morphology of the bipartite medial cuneiform is further subdivided into completely or partially bipartite. The “E-sign” is a useful imaging sign that is present in all cases of the complete bipartite medial cuneiform. Knowledge of the “E sign” can help the radiologist recognize and distinguish this form from a fracture.
Keywords: Bipartite; Medial wedge shape; Fracture; e-sign.
Citation: Yadav R, Venkatesh S, Gamangatti S. “E-sign” in imaging: Debunking congenital bipartite from isolated medial cuneiform fracture. J Clin Images Med Case Rep. 2023; 4(4): 2391.
Introduction
Bipartite medial cuneiform fracture is a rare bony developmental variant of the midfoot that is usually inconspicuous and asymptomatic but can be symptomatic with concomitant midfoot injury. Surgeons and radiologists need to recognize this bony variant because it can be misdiagnosed as a fracture or missed cause of nontraumatic or traumatic foot pain and sometimes even requires surgical treatment. We report the imaging features of an incidentally discovered complete bipartite medial wedge with associated fracture of the base of the 1st metatarsal.
Clinical and imaging Findings
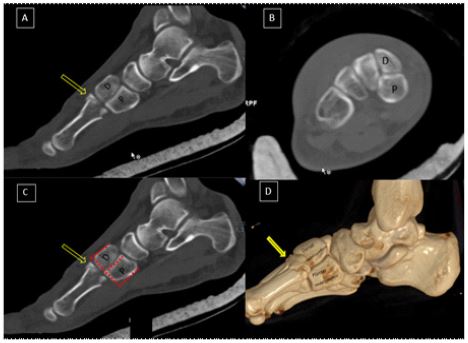
A young patient presented to the emergency department complaining of left metatarsal pain after an RTA. A radiograph of the foot was performed, followed by Non-Contrast Computed Tomography (NCCT). The radiograph of the foot showed a fracture of the base of the 1st metatarsal. NCCT confirmed the finding of an isolated fracture of the base of the 1st metatarsal (no Lisfranc injury) (Figure 1A). CT showed two bony, well-corticated segments at the expected location of the medial wedge shape separated by a horizontal, well-bounded gap (Figure 1A,B,C,D). The medial segment was larger than the dorsal segment, and both were connected anteriorly to the base of the 1st metatarsal, which is fractured, and posteriorly to the navicular bone. These findings were suggestive of a Bipartite Medial Cuneiform Fracture (BMC). The remainder of the bone appeared normal. Given the isolated non-Lisfranc injury at the base of the 1st metatarsal with incidentally discovered BMC, the patient’s foot was immobilized with a cast.
Discussion
The 1st most cuneiform is the medial cuneiform bone, the largest of the three cuneiform bones of the foot. In most cases, it has a wedge-shaped morphology arising from a single primary ossification center, but in some cases, it may be bisected by two non-fused primary ossification centers due to an embryologic segmentation defect [1]. These two non-fused ossification centers (dorsal and plantar segments) remain separated by a fibrous/cartilaginous synchondrosis [1]. The two segments are also referred to as os cuneiform dorsale and os cuneiform plantare [1]. The morphologic bifurcation of the medial cuneiform is further subdivided into complete and incomplete bi-partitions.
Epidemiologically, the estimated incidence is ~1%, with slight male predilection and bilaterality in 60% of cases [2]. In most clinical cases, BMC is discovered incidentally; in some cases, it may cause chronic midfoot pain due to altered biomechanical factors [5].
Imaging plays a vital role in the diagnosis and differentiation of fractures. The plain radiograph is the first investigation, but it can be easily overlooked because of the superimposition of bones. NCCT with multiplanar reconstruction and 3D virtual rendering is the investigation of choice in trauma to detail the bipartite medial cuneiform (BMC). BMC is a bipartition of the medial cuneiform into two ossicles (dorsal and planter) with a well-defined horizontal line. The gap in the joint space between the ossicles and the 1st ray creates a rift in the “E- configuration,” which is why the “characteristic “E- sign” is seen on sagittal reconstructed images (Figure 1A,B,C,D). These two ossicles are well demarcated with a conserved overall shape in a horizontal orientation, with a larger combined volume than expected [3,4]. The base of the 1st metatarsal is also larger at articulation with two articulation facets (Figure 1A,B,C).
The close differential diagnosis to BMC is an isolated fracture of the medial cuneiform bone, which is very rare. The overall preserved shape, the “E- sign,” and the size of the base of the first metatarsal help distinguish these two forms. The cleavage plane in a fracture is irregular and usually splits into an anterior and posterior fragment with a vertical orientation [5]. When BMC is symptomatic, treatment includes immobilization, steroid injections, or surgery, including arthrodesis and removal of the bone fragments [6].
Conclusion
Bipartite medial cuneiform is a very rare congenital segmentation anomaly of the midfoot. In trauma, it can be misinterpreted as a fracture on imaging. The most important imaging clues to distinguish a bipartite medial cuneiform from a fracture are the presence of the “E- sign,” the cleavage plane’s horizontal orientation, and the size of the base of the 1st metatarsal.
Teaching points
The “E-Sign” on the lateral radiograph of the foot or Sagittal images on CT /MRI suggests Complete Bipartite Medial cuneiform over the fracture. It presents in all the cases of BMC.
Orientation of the Cleavage Plane in BMC: horizontal with smooth corticated margins.
Orientation of the Cleavage Plane in fracture: in Coronal plane with irregular margins.
References
- Jashashvili T, Ponce de León M S, Lordkipanidze D, & Zollikofer CP. First evidence of a bipartite medial cuneiform in the hominin fossil record: a case report from the Early Pleistocene site of Dmanisi. Journal of anatomy. 2010; 216; 705-716.
- Burnett SE, Case DT. Bipartite medial cuneiform: New frequencies from skeletal collections and a meta-analysis of previous cases. Homo. 2011; 62: 109-125.
- Dellacorte MP, Lin PJ, Grisafi PJ. Bilateral bipartite medial cuneiform. A case reports. J Am Podiatr Med Assoc. 1992; 82: 475-478.
- Fulwadhva U, Parker RJ. Symptomatic bipartite medial cuneiform. Applied Radiology. 2007; 3: 42-44.
- Chang GH, Chang EY, Chung CB, & Resnick DL. Bipartite medial cuneiform: case report and retrospective review of 1000 magnetic resonance (MR) imaging studies. Case reports in medicine. 2014.
- O’Neal ML, Ganey TM, Ogden JA. Fracture of a bipartite medial cuneiform synchondrosis. Foot Ankle Int. 1995; 16: 37-40.