
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Correlation of serum hematopoietic growth
factors with breast cancer
Parisa Karimzadeh1,2ⴕ; Mahboobeh Razmkhah1ⴕ; Somayeh Rezaeifard1,3; Fatemeh Eghbali1; Zahra Faghih1*
1Shiraz Institute for Cancer Research, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
2Department of Health, West Chester University, West Chester, Pennsylvania, USA.
3Radboud University, Nijmegen, Netherlands.
ⴕThese authors have the same contribution to the study.
*Corresponding Author : Zahra Faghih
Associate Professor of Immunology, Shiraz Institute for Cancer Research, School of Medicine, Shiraz University of Medical Sciences, P.O. Box: 71345-1798, Shiraz, Iran.
Email: faghihz@sums.ac.ir
Received : Apr 06, 2023
Accepted : Apr 26, 2023
Published : May 03, 2023
Archived : www.jcimcr.org
Copyright : © Faghih Z (2023).
Abstract
Background and objective: Hematopoietic growth factors play a crucial role not only in hematopoiesis but also in the stimulating of nonhematopoietic cells proliferation, including tumor cells. This study aimed to measure the serum concentrations of a panel of hematopoietic growth factors in patients with Breast Cancer (BC) and healthy controls.
Methods: The serum levels of Granulocyte Macrophage-Colony Stimulating Factor (GM-CSF), Granulocyte-Colony Stimulating Factor (G-CSF), Macrophage-Colony Stimulating Factor (M-CSF), Stem Cell Factor (SCF), and Erythropoietin (EPO) were measured with a bead-based immunoassay technique in 62 pathologically confirmed patients with BC and 54 age-matched healthy controls.
Results: A higher EPO serum level was observed in the patients with BC than in the control group (P=0.001). G-CSF level was significantly higher in the advanced-staged patients (II and III) than those in stage I (P=0.036). An increase in SCF level was also observed in the patients with stage II compared to those in stage I (P=0.011). On the other hand, GM-CSF concentration significantly decreased with tumor progression from stage I to stage III (P=0.016). In addition, the Spearman rank correlation indicated a significant relationship between GM-CSF, G-CSF, and tumor size in the patients with tumors greater than 2 cm (P=0.014, R=0.317, and P=0.045, R=0.257, respectively). There was also a direct correlation between age and serum levels of EPO and GM- CSF in both patients and controls (P< 0.05). Significant positive correlations were also observed between the levels of EPO and GM-CSF (P=0.001), M-CSF (P=0.011), and G-CSF (P=0.039), as well as the SCF level and the levels of M-CSF (P=0.043) and GM-CSF (P=0.017).
Conclusion: Our study suggests EPO, G-CSF, and SCF as possible biomarkers for early BC detection. Besides, these HGFs may be used for determining the prognosis of BC using circulation as a non-invasive method. Large-scale studies are indeed required to generalize the results to all patients with BC.
Keywords: Breast cancer; Biomarkers; Hematopoietic growth factors; Prognosis.
Abbreviations: BC: Breast Cancer; GM-CSF: Granulocyte Macrophage-Colony Stimulating Factor; G-CSF: Granulocyte-Colony Stimulating Factor; M-CSF: Macrophage-Colony Stimulating Factor; SCF: Stem Cell Factor; EPO: Erythropoietin; HGFs: Hematopoietic growth factors; VEGF: vascular endothelial growth factor.
Citation: Karimzadeh P, Razmkhah M, Rezaeifard S, Eghbali E, Faghih Z. Correlation of serum hematopoietic growth factors with breast cancer. J Clin Images Med Case Rep. 2023; 4(5): 2398.
Background
Breast Cancer (BC) is one of the leading causes of death among women worldwide. Poor prognosis, rapid clinical progression, high rates of metastasis, and increased mortality are associated with this cancer [1]. Despite several risk factors being associated with the disease, the etiology of BC remains largely unknown. Tumor size and lymph node spread are strongly related to poor prognosis of BC [2]; accordingly, the detection of specific tumor markers is of vital importance to developing new measures and strategies for early detection and treatment [3].
Hematopoietic Growth Factors (HGFs) are a group of cytokines that play essential roles in the growth and differentiation of hematopoietic progenitor cells and also in maturation and activation of neutrophils or macrophages [4]. Moreover, a growing body of evidence shows that HGFs have crucial effects not only on hematopoiesis but also on the proliferation of nonhematopoietic cells, including tumor cells [5]. In addition, high expression of HGFs and their receptors have been observed in various tumor types and implied their contributions to poor prognosis [6,7]. The crucial role of these cytokines in tumor invasion is also suggested in some studies while the stimulation of tumor cell proliferation is demonstrated by their effects [8]. Plenty of studies have also been made to demonstrate the role of these growth factors in the normal development of mammary epithelial cells and their progression to malignancy [7,9]. Elevated plasma levels of HGFs, including M-CSF or G-CSF in patients with BC, have been demonstrated in some recent stdies [10,11].
Considering the importance of detecting serum biomarkers for malignancies such as BC, this study aimed to determine the levels of hematopoietic cytokines (GM-CSF, G-CSF, M-CSF, SCF, EPO) in the sera of patients with BC in comparison with healthy subjects using a bead-based immunoassay technique. As compared to traditional ELISA methods, this method has a higher sensitivity and range of dynamic range.
Material and methods
Cases
The patients were 62 women with BC (age range of 26-70 years) referred to the hospitals affiliated with Shiraz University of Medical Sciences, and their cancers were confirmed by clinical and pathological analyses. Neither chemotherapy nor radiotherapy had been administered to any of the patients before sample collection. The clinical and pathological data of the patients were obtained from their records (summarized in Table 1). A group of 54 healthy females with no personal or family history of malignancy and autoimmune diseases and age-matched with the patients was also enrolled as a control group. Ethics approval was obtained from the research ethics committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1395.S222). A detailed explanation of the study’s purpose, safety and security measures was provided to patients and controls prior to their consent.
Serum separation from peripheral bloods
Five milliliters of peripheral vein blood sample were taken from both patients and controls. Patients’ samples were collected on the day prior surgery. To separate the sera, 30 minutes after coagulation, the samples were centrifuged for 10 minutes at 1000 ×g. The sera were then aliquoted and preserved at -70˚C till the experiment day.
Biochemical analyses
Serum levels of a panel of human growth factors, including EPO, G-CSF, GM-CSF, M-CSF, and SCF, were measured with LEGEND plex Human Growth Factor Panel Kit in accordance with the instructions provided by the manufacturer (Biolegend, USA). This is a bead-based immunoassay with the same basic principles as sandwich ELISA. Briefly, serum samples were diluted 2-fold with Assay Buer and mixed with 25 μL of pre-mixed beads. Then, 25 μL of detection antibody were added to each sample. At the same time, 25 μL of Matrix B and subsequently 25 μL of each standard were added to the standard wells. Preparation of standards C1-C7 was done according to the kit protocol. The tubes were protected from light and shaken for 2 hours at room temperature. Without washing, 25 μL of SA-PE were added to each tube and incubated for a further 30 min at room temperature while shaking at 1000 rpm. Afterward, the tubes were washed with 200 μL of 1X Wash Buer. The beads were finally resuspended in 200 μL of 1X Wash Buer and acquired on a FACS Calibur flow cytometer (BD Biosciences, USA). LEGENDplex Data Analysis Software (Biolegend) was applied to measure the serum levels of each growth factor based on five parameter curve fitting (Log Scale) analysis. A standard curve was then used to calculate the concentration of each analyte.
Statistical analysis
Statistical analyses were done by SPSS software version 16 (Chicago, SPSS Inc, USA). Since the data did not satisfy the normality, non-parametric tests (Kruskal-Wallis and Mann-Whitney) were done to compare the quantities between patients and controls as well as patients with different clinical and pathological characteristics, including histological tumor type, tumor size, axillary lymph node involvement, TNM-staging, in situ component, histological grade, tumor necrosis, and peritumoral lymphovascular invasion. Statistically significant differences were defined in cases of P< 0.05.
Results
Characteristics of the patients and controls
Serum levels of HGFs were measured among 116 females, including 62 patients in different stages of BC and 54 age-sex matched healthy adults as the control group. The mean age of the patients was 48.37 ± 11.78 years (26-70 years), and the mean age of healthy individuals was 45.07 ± 8.93 years (26-65 years). The clinicopathological characteristics of the patients are provided in Table 1. The stage of cases was determined based on the Tumor-Node-Metastasis (TNM) staging system developed by the American Joint Committee on Cancer Classification and Stage Grouping (7th edition) [12]. Accordingly, our patients were mainly in stage II (24/64, 38.70%). The most common tumor type was IDC (54/62, 87.1%), and tumor-affected lymph node was observed among 56.5% of the patients (35/62).
Serum levels of EPO, G-CSF, GM-CSF, M-CSF, and SCF in patients with BC and controls
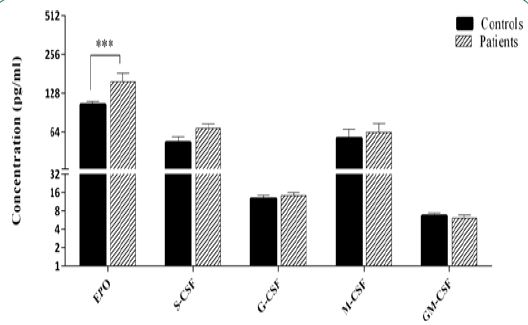
We determined the serum levels of a panel of HGFs including EPO, SCF, G-CSF, M-CSF, and GM-CSF using a cytokine bead array test. Table 2 shows the maximum, minimum, mean, and median range of HGFs levels in both patients and healthy controls. EPO showed the highest mean concentration in both patients and controls (156.84 and 104.45 pg/ml, respectively), while GM- CSF had the lowest mean level in both groups (6.11 and 6.61 pg/ml, respectively). Comparing the concentrations between patients and controls, statistical analysis indicated that EPO serum level was significantly higher in the patients compared to the control group (P=0.001). A trend to a higher level of SCF was also observed in the patients compared with the controls (P=0.062) (Figure 1).
Levels of hematopoietic growth factors among patients with different clinicopathological characteristics
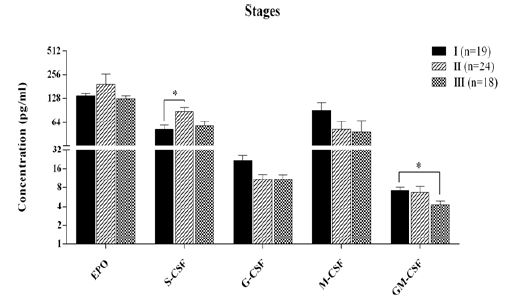
In the next step, we assessed the relationships of investigated markers with clinical and pathological features of the patients. Regarding the stage, a significant increase in SCF level was observed in the patients with stage II compared to those in stage I (P=0.011). On the other hand, GM-CSF concentration significantly decreased with tumor progression from stage I to stage III (P=0.016, Figure 2). Classifying the patients into low (0/I) and high (II/III) stage groups indicated that G-CSF level was significantly higher in the advanced-staged patients (II/III) in comparison to those in stage I (P=0.036) while GM-CSF was lower in high-stage patients (P=0.020).
An increasing trend was also observed in the serum level of GM-CSF in the patients with Progesterone Receptor (PR)-positive tumors compared to those with PR-negative ones; however, it was not statistically significant (P=0.056). No other significant differences were observed in the levels of HGFs in the patients with tumor necrosis, tumor calcification, peritumoral lymphatic invasion, perineural invasion, vascular invasion, and axillary node involvement.
Correlations among hematopoietic growth factors, tumor size and age
Regarding the tumor size and age, the Spearman rank correlation indicated a significant relationship between GM-CSF, G-CSF, and tumor size in the patients with tumors greater than 2 cm (P=0.014, R=0.317, and P=0.045 R=0.257, respectively). In addition, there was a direct correlation between age and serum level of EPO in both patients and controls (P=0.016, R=0.307, and P=0.001, R=0.650, respectively). A similar correlation was also observed in the case of GM-CSF (P=0.001, R=0.466, and P=0.02, R=0.316, respectively). Among HGFs, significant positive correlations were observed between the EPO serum level and GM-CSF (P=0.001, R=0.603), M- CSF (P=0.011, R=0.324), G-CSF (P=0.039, R=0.265) concentrations. There were also significant positive correlations between the SCF level and the levels of M-CSF (P=0.043, R=0.260) and GM- CSF (P=0.017, R=0.325).
Table 1: Clinicopathological characteristics of patients with breast cancer.
| Characteristics | Value |
|---|---|
| Age (years) | 48.37 ± 11.78 |
| Lymph node status | |
| Free (N0) | 27 (43.5%) |
| Involved | 35 (56.5%) |
| N1 | 20 (32.8%) |
| N2 | 8 (13.1%) |
| N3 | 7 (11.5%) |
| Stage | |
| I | 20 (32.3%) |
| II | 24 (38.7%) |
| III | 18 (29%) |
| Tumor type | |
| IDC | 54 (87.1%) |
| ILC | 4 (6.5%) |
| DCIS | 3 (4.8%) |
| MC | 1 (1.6%) |
| Tumor size | |
| T1 (≤2 cm) | 30 (49.2%) |
| T2 (2-5 cm) | 24 (39.3%) |
| T3 (>5 cm) | 7 (11.5%) |
| Unreported* | 1 |
| Histological grade | |
| Well differentiated (I) | 16 (28.1%) |
| Moderately differentiated (II) | 26 (45.6%) |
| Poorly differentiated (III) | 15 (26.3%) |
| Unreported | 5 |
| Estrogen receptor (ER) | |
| Negative | 13 (22.8%) |
| Positive | 44 (77.2%) |
| Unreported | 5 |
| Progesterone receptor (PR) | |
| Negative | 16 (28.1%) |
| Positive | 41 (71.9%) |
| Unreported | 5 |
| Her2 expression | |
| Negative | 28 (49.1%) |
| Positive | 11 (19.3%) |
| Equivocal | 18 (31.6%) |
| Unreported | 5 |
*Unreported data are excluded from the calculations. IDC: invasive ductal carcinoma; MC: Invasive carcinoma with medullary features; ILC: invasive lobular carcinoma; DCIS: ductal carcinoma in situ.
Table 2: Human growth factors’ serum levels in breast cancer patients and healthy individuals.
| Growth factor | Patients (n=62) | Controls (n=54) | ||||||
|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean ± SD | Median (IQR25-75) | Min | Max | Mean ± SD | Median (IQR25-75) | |
| EPO | 25.42 | 1686.00 | 156.84 ± 203.91 | 130.87 (98.33-158.03) | 2.27 | 220.72 | 104.45 ± 42.63 | 104.78 (76.31-134.99) |
| SCF | 0.17 | 249.19 | 68.14 ± 45.01 | 62.78 (40.22-88.34) | < 0.001 | 187.00 | 52.97 ± 41.28 | 52.11 (16.93-80.38) |
| G-CSF | 0.64 | 57.59 | 14.18 ± 13.61 | 8.81 (4.64-21.87) | 0.03 | 50.27 | 12.62 ± 12.14 | 8.97 (4.13-15.67) |
| M-CSF | 0.52 | 334.07 | 63.48 ± 83.22 | 24.55 (3.78-106.08) | < 0.001 | 262.49 | 57.13 ± 71.69 | 29.19 (3.45-85.29) |
| GM-CSF | 0.20 | 35.48 | 6.11 ± 5.62 | 4.51 (2.73-7.48) | < 0.001 | 25.92 | 6.61 ± 5.69 | 5.39 (2.47-8.52) |
EPO: Erythropoietin; SCF: stem cell factor; G-CSF: granulocyte-colony stimulating factor; GM- CSF: granulocyte macrophage-colony stimulating factor; M-CSF: macrophage-colony stimulating factor.
Discussion
Cancer biology has recently put more emphasis on the cytokines since increased cytokine production have demonstrated in the patients with different kinds of cancers [5,13]. It has been shown that they can not only be produced by tumor cells but also influence the malignant processes, including tumor progression, metastasis, angiogenesis, and metalloproteinase production [5]. In the present study, we determined the association of serum levels of a panel of human growth factors (EPO, G-CSF, GM-CSF, M-CSF, SCF) with BC susceptibility and prognosis. Our data indicated higher EPO and SCF serum levels in the patients with BC than in healthy controls. An association was also observed between G-CSF and SCF and higher stages of the disease, while GM-CSF showed a decrease with the tumor progression.
GM-CSF is a hematopoietic growth factor playing an essential role in the survival and maintenance of hematopoietic lineages. It can be produced by different cell types such as activated T cells, B cells, macrophages, endothelial cells, fibroblasts, and tumor cells [14]. Although no difference was found between patients and controls, we observed lower GM-CSF plasma levels in patients with higher stages than those with a lower stage of the disease. However, to the best of our knowledge, there is no direct report in BC, but similarly, lower expression of GM-CSF was reported in CD4+helper subsets in draining lymph nodes of patients with progressed tumors of the bladder (having involved node or higher stages) [15]. This reduction could be attributed to GM-CSF suppression following tumor growth and progression, implying a potential antitumor role for GM-CSF in BC.
In this regard, it has been shown that GM-CSF stimulates monocytes to exhibit antitumor behavior and also increases antigen presentation by macrophages and therefore increases immune responsiveness [16]. Consistently, in vitro studies showed the potential role of GM-CSF in promoting monocytes and macrophages’ survival and also stimulating inflammatory mediators release to kill tumor cells [17]. Concordantly, Eubank et al. showed that in the murine model, GM- CSF stimulates monocytes to secrete soluble Vascular Endothelial Growth Factor (VEGF) receptor- 1 (sVEGFR-1), which resulted in the inhibition of tumor progression and metastasis through VEGF inactivation and blockage of angiogenesis [18,19]. Furthermore, more sensitivity towards anticancer drugs was observed in GM-CSF over expressing MCF-7 cells in Chaubey’s study [20]. In contrast, several studies have shown GM-CSF secretion from tumor cells and stimulation of their progression [13,21]. The elevated serum levels of GM-CSF were also observed in lung carcinomas [22], indicating its contribution to disease progression. This discrepancy may result from different tumor types or sample sizes in various studies. However, no difference was detected between cancer patients and the control group and in clinicopathological features in the present study M-CSF, produced by lymphocytes, fibroblasts, and endothelial cells, induces differentiation, proliferation, and activation of phagocytes [23]. Different studies showed serum M-CSF levels correlation with tumor size, metastasis, and poor outcomes in various human malignancies [8,24]. The presence of M-CSF-expressing cells in the tumors has been associated with a more clinically aggressive attitude and adverse prognosis related to extensive macrophage infiltration [25]. Moreover, elevated levels of M-CSF were also reported in the sera, ascites, and pleural effusions of patients with an advanced stage of BC [10,24].
G-CSF is another growth factor that has been found in different cancers since the original finding of G-CSF producing tumors [26]. Previous studies showed a correlation between the ectopic secretion of G-CSF and induction of primary and metastatic cancers [27,28]. and its serum level and tumor stage [13,29]. Moreover, the G-CSF value as a diagnostic marker in comparison to classic tumor markers, such as CEA and CA19-9, suggested the use of G-CSF measurement in colorectal cancer diagnosis [30]. In this study, we observed an increasing pattern in G-CSF serum levels of node-positive patients and patients with lymphatic invasion, although it was not statistically significant. Our result is in line with Bordbar et al., which showed an increase in G- CSF levels in Iranian patients with BC having more than three involved lymph nodes [31]. The Natori et al. study suggested a potential role of G-CSF through its ability to stimulate tumor- associated angiogenesis and cancer development [32]. These findings collectively imply a tumorigenic role for G-CSF in patients with BC.
Stem Cell Factor (SCF) is a cytokine with a stimulatory effect on primitive hematopoietic stem cells’ growth and development both in vitro and in vivo [33]. Enhanced levels of SCF has also been demonstrated in the serum of patients with BC [34]. In the present study, a trend for a higher level of SCF was observed in the patients compared with the controls, as well. An increase in the SCF level was also found in the patients with stage II compared to those in stage I. Not many studies have been done on circulating SCF and their significance in BC, justifying the variable results and demonstrating the need for further studies in this area.
Erythropoietin (EPO) has long been considered to have a key role as a hematopoietic growth factor in stimulating erythroid proliferation and differentiation. In addition, recent studies have emerged EPO as a pleiotropic cytokine with proangiogenic and tissue-protective effects in an anti-apoptotic and/or mitogenic manner in numerous nonhematopoietic cells and tissues, including malignant ones [35,36]. This may be in line with our results that showed an increase in the patients’ EPO level in comparison to the control group that suggested a role for EPO in stimulating cancer cell proliferation and/or survival. Consistently, co-expression of EPO and its receptor has also be end etected in various tumors of adult reproductive tissues [37,38]. The results of Arcasoy et al. [39], confirmed by study of Trošt and his colleagues [40]. Also demonstrated the induction of BC cells by EPO. In addition, they demonstrated an EPO-induced MCF-7 proliferation with a time- and concentration-dependent manner [40]. Additionally, in tumor xenografts of malignant uterine tumors and BC, EPO signaling deprivation induces the death of tumor cells and capillary endothelial cells [38,41]. However, we did not detect a meaningful relationship between serum EPO level and clinicopathological variables.
In addition, we evaluated growth factors’ correlation with each other which showed a direct and strong statistically significant correlation between EPO and GM-CSF, G-CSF, and M-CSF. Besides, a similar relationship was detected between S-CSF and M-CSF. These correlations were in both patients and the control group, which could imply that regardless of cancer, specific growth factors have some control mechanisms, regulators, or synergistic functions, in common.
Conclusion
Our data collectively suggests EPO, G-CSF, and SCF as possible biomarkers for early BC detection or determining its prognosis using circulation as a non-invasive method. Large-scale studies are certainly required to generalize the results to all patients with BC.
Declarations
Availability of data and materials: As a result of restrictions related to the privacy of patients or consent, raw data is not publicly available. Only the corresponding author can provide de-identified data upon reasonable request.
Conflict of interest: The authors declare no conflict of interest.
Acknowledgments: The authors would like to thank the patients and all the participants for their kind contribution in this project.
Funding: This work was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran (Grant No.95-01- 01-12700) and Shiraz Institute for Cancer Research (ICR-100-500 and -504).
Ethics approval and consent to participate: Ethics approval was obtained from the research ethics committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1395.S222). A detailed explanation of the study’s purpose, safety and security measures was provided to patients and controls prior to their consent.S
Contributions: MR and ZF designed the study. PK and FE collected the samples and underwent the Biomedical analysis through the immunoassay and then statistical analysis carried out by SR and PK. Pk and ZF drafted the manuscript which then revised and proofread by ZF and MR. The final version of the manuscript was read and approved by all authors.
References
- Feng Y, Spezia M, Huang S, Yuan C, Zeng Z, et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes & diseases. 2018; 5: 77-106.
- Min SK, Lee SK, Woo J, Jung SM, Ryu JM, et al. Relation between tumor size and lymph node metastasis according to subtypes of breast cancer. Journal of Breast Cancer. 2021; 24: 75.
- Nicolini A, Ferrari P, Duffy MJ. Prognostic and predictive biomarkers in breast cancer: Past, present and future. Seminars in cancer biology: Elsevier; 2018; 56-73.
- Metcalf D. Hematopoietic cytokines. Blood. 2008; 111: 485-491.
- Dunlop RJ, Campbell CW. Cytokines and advanced cancer. Journal of pain and symptom management. 2000; 20: 214-232.
- Xue Y, Lim S, Yang Y, Wang Z, Jensen LDE, et al. PDGF-BB modulates hematopoiesis and tumor angiogenesis by inducing erythropoietin production in stromal cells. Nature medicine. 2012; 18: 100.
- Lin EY, Nguyen AV, Russell RG, Pollard JW. Colony-stimulating factor 1 promotes progression of mammary tumors to malignancy. Journal of Experimental Medicine. 2001; 193: 727- 740.
- Kacinski BM. CSF‐1 and its receptor in breast carcinomas and neoplasms of the female reproductive tract. Molecular Reproduction and Development: Incorporating Gamete Research. 1997; 46: 71-74.
- Ławicki S, Będkowska G, Wojtukiewicz M, Szmitkowski M. Hematopoietic cytokines as tumor markers in breast malignancies. A multivariate analysis with ROC curve in breast cancer patients. Advances in medical sciences. 2013; 58: 207-215.
- Ławicki S, Szmitkowski M, Wojtukiewicz M. The pretreatment plasma level and diagnostic utility of M-CSF in benign breast tumor and breast cancer patients. Clinica chimica acta. 2006; 371: 112-116.
- Negm RS, Verma M, Srivastava S. The promise of biomarkers in cancer screening and detection. Trends in molecular medicine. 2002; 8: 288-293.
- Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Annals of surgical oncology. 2010; 17: 1471-1474.
- Mroczko B, Szmit kowski M, Okulczyk B. Hematopoietic growth factors in colorectal cancer patients. Clinical chemistry and laboratory medicine. 2003; 41: 646-651.
- Fleetwood AJ, Cook AD, Hamilton JA. Functions of granulocyte-macrophage colony- stimulating factor. Critical Reviews™ in Immunology. 2005; 25.
- Ariafar A, Zareinejad M, Soltani M, Vahidi Y, Faghih Z, et al. GM-CSF-producing lymphocytes in tumor-draining lymph nodes of patients with bladder cancer. European Cytokine Network. 2021; 32: 1-7.
- Armstrong CA, Botella R, Galloway TH, Murray N, Kramp JM, et al. Antitumor effects of granulocyte-macrophage colony-stimulating factor production by melanoma cells. Cancer research. 1996; 56: 2191-2198.
- Takahashi G, Andrews D. 3d, Lilly MB, Singer JW, Alderson MR. Effect of granulocyte- macrophage colony-stimulating factor and interleukin-3 on interleukin-8 production by human neutrophils and monocytes Blood. 1993; 81: 357.
- Eubank TD, Roberts R, Galloway M, Wang Y, Cohn DE, GM-CSF induces expression of soluble VEGF receptor-1 from human monocytes and inhibits angiogenesis in mice. Immunity. 2004; 21: 831-842.
- Eubank TD, Roberts RD, Khan M, Curry JM, Nuovo GJ, Kuppusamy P, et al. Granulocyte macrophage colony-stimulating factor inhibits breast cancer growth and metastasis by invoking an anti-angiogenic program in tumor-educated macrophages. Cancer research. 2009; 69: 2133-2140.
- Chaubey N, Ghosh SS. Overexpression of granulocyte macrophage colony stimulating factor in breast cancer cells leads towards drug sensitization. Applied biochemistry and biotechnology. 2015; 175: 1948-1959.
- Ławicki S, Będ kowska GE, Gacuta-Szumarska E, Szmitkowski M. Hematopoietic cytokines as tumor markers in gynecological malignancies: A multivariate analysis with ROC curve in endometrial cancer patients. Growth Factors. 2012; 30: 29-36.
- Hamilton JA. GM-CSF as a target in inflammatory/autoimmune disease: current evidence and future therapeutic potential. Expert review of clinical immunology. 2015; 11: 457-465.
- Sehgal A, Irvine KM, Hume DA. Functions of macrophage Colony Stimulating Factor - (CSF1) in development, homeostasis, and tissue repair. Seminars in Immunology: Elsevier. 2021; 101509.
- Kacinski BM. CSF-1 and its receptor in ovarian, endometrial and breast cancer. Annals of medicine. 1995; 27: 79-85.
- Yee LD, Liu L. The constitutive production of colony stimulating factor 1 by invasive human breast cancer cells. Anticancer research. 2000; 20: 4379-4383.
- Ikeda T, Ohgaki K, Miura M, Aishima S, Shimizu T, et al. Granulocyte-colony stimulating factor-producing gallbladder cancer without recurrence more than 2 years after resection: report of a case. Surgery today. 2005; 35: 590-593.
- Bahar B, Cayci B, Coskun U, Buyukberber S, Benekli M, et al. Granulocyte colony stimulating factor (G-CSF) and macrophage colony stimulating factor (M-CSF) as potential tumor markers in non small cell lung cancer diagnosis. Asian Pacific J Cancer Prev. 2010; 11: 709-712.
- Shalom G, Sion-Vardy N, Dudnik J, Ariad S. Leukemoid reaction in lung cancer patients. The Israel Medical Association journal: IMAJ. 2010; 12: 255-256.
- Mroczko B, Szmitkowski M, Okulczyk B. Granulocyte-Colony Stimulating Factor (G-CSF) and macrophage-colony stimulating factor (M-CSF) in colorectal cancer patients. Clinical chemistry and laboratory medicine. 2002; 40: 351-5.
- Mroczko B, Groblewska M, Wereszczynska-Siemiatkowska U, Kedra B, Konopko M, e t al. The diagnostic value of G-CSF measurement in the sera of colorectal cancer and adenoma patients. Clinica chimica acta. 2006; 371:143-147.
- Bordbar E, Malekzadeh M, Ardekani MTF, Doroudchi M, et al. Serum levels of G-CSF and IL-7 in Iranian breast cancer patients. Asian Pacific Journal of Cancer Prevention. 2012; 13: 5307-5312.
- Natori T, Sata M, Washida M, Hirata Y, Nagai R, et al. G-CSF stimulates angiogenesis and promotes tumor growth: potential contribution of bone marrow-derived endothelial progenitor cells. Biochemical and biophysical research communications. 2002; 297: 1058-1061.
- Czygier M, Lawicki S, Stankiewicz I, Szmitkowski M. Stem Cell Factor (SCF) in the plasma and phagocytic functions of granulocytes in breast cancer patients. Przeglad lekarski. 2007; 64: 1014-1017.
- Hines SJ, Litz JS, Krystal GW. Coexpression of c-kit and stem cell factor in breast cancer results in enhanced sensitivity to members of the EGF family of growth factors. Breast cancer research and treatment. 1999; 58: 1-10.
- Hardee ME, Arcasoy MO, Blackwell KL, Kirkpatrick JP, Dewhirst MW. Erythropoietin biology in cancer. Clinical Cancer Research. 2006; 12: 332-339.
- Debeljak N, Solár P, Sytkowski AJ. Erythropoietin and cancer: The unintended consequences of anemia correction. Frontiers in immunology. 2014; 5.
- Yasuda Y, Fujita Y, Masuda S, Musha T, Ueda K, Tanaka H, et al. Erythropoietin is involved in growth and angiogenesis in malignant tumours of female reproductive organs. Carcinogenesis. 2002; 23: 1797-1805.
- Arcasoy MO, Amin K, Karayal AF, Chou S-C, Raleigh JA, et al. Functional significance of erythropoietin receptor expression in breast cancer. Laboratory investigation. 2002; 82: 911.
- Arcasoy MO. The non‐haematopoietic biological effects of erythropoietin. British journal of haematology. 2008; 141: 14-31.
- Trošt N, Hevir N, Rižner TL, Debeljak N. Correlation between erythropoietin receptor (s) and estrogen and progesterone receptor expression in different breast cancer cell lines. International journal of molecular medicine. 2013; 31:717-725.
- Yasuda Y, Musha T, Tanaka H, Fujita Y, Fujita H, et al. Inhibition of erythropoietin signalling destroys xenografts of ovarian and uterine cancers in nude mice. British journal of cancer. 2001; 84: 836.