
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Diversion colitis
Constantine P. Spanos, MD, FACS, FASCRS1*; Paschalis Paschos, MD2
1Professor of Surgery, Aristotelian University, Thessaloniki, Greece.
2Consultant Gastroenterologist, Papageorgiou Hospital, Thessaloniki, Greece.
*Corresponding Author : Constantine P Spanos
1st Department of Surgery, Aristotelian University School of Medicine, Thessaloniki, Greece
Email: costasspanos@hotmail.com
Received : Apr 06, 2023
Accepted : May 01, 2023
Published : May 08, 2023
Archived : www.jcimcr.org
Copyright : © Spanos CP (2023).
Abstract
We present a case of diversion colitis in a 45-year-old male with rectal adenocarcinoma who underwent a low anterior resection of the rectum with diverting ileostomy. Diversion colitis is a frequent sequela of fecal stream diversion. Endoscopic and microscopic findings mimic inflammatory bowel disease. Most patients are asymptomatic. The disorder almost always resolves after reconstitution of the gastrointestinal tract.
Keywords: Diversion colitis, colostomy, ileostomy, short-chain fatty acids.
Citation: Spanos CP, Paschos P. Diversion colitis. J Clin Images Med Case Rep. 2023; 4(5): 2403.
Case description
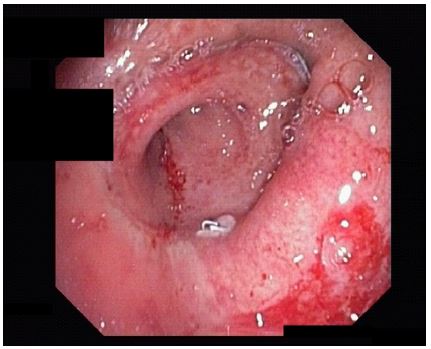
A 45-year-old male underwent a low anterior resection for rectal adenocarcinoma following a course of preoperative chemotherapy and radiation therapy. A diverting ileostomy was fashioned at operation. The patient reported occasional episodes of mucous discharge with small amount of bleeding. Prior to planned ileostomy takedown, colonoscopy was performed to exclude anastomotic dehiscence, stenosis, or disease recurrence. Endoscopic findings included aphthous ulcerations (Figure 1, descending colon), as well as mucosal friability, erythema and bleeding (Figure 2, colorectal anastomosis). These findings were consistent with diversion colitis.
Diversion colitis is an inflammatory process that occurs in most patients after surgical diversion of the fecal stream with colostomy or ileostomy. The onset of this condition most frequently occurs 3 to 36 months after fecal diversion [1]. The etiopathogenesis may be associated with bacterial overgrowth in the diverted intestinal segment, or a deficiency of short-chain fatty acids (SCFAs), which are trophic for the colonic epithelium. [1-3]. Most patients are asymptomatic. However, patients may present with abdominal pain, tenesmus, rectal bleeding, and mucous discharge [2,3]. Macroscopic findings include mucosal erythema, friability, apthous ulcerations, and frank bleeding [1]. Microscopic examination of the intestinal mucosa may reveal crypt abscesses, mucin granulomas and lymphoid follicular hyperplasia [1-3]. Both endoscopic and pathological findings simulate active inflammatory bowel disease. Several treatment regimens have been utilized to treat diversion colitis. These include enemas containing steroids, aminosalicylates or SCFAs [1-3]. However, the most effective treatment remains closure of the surgical stoma [1-3]. Nearly all cases of diversion colitis resolve after reconstitution of the gastrointestinal tract and fecal stream.

References
- Harig JM, Soergel KH, Komorowski RA, Wood CM. Treatment of diversion colitis with short-chain-fatty-acid irrigation. N Engl J Med. 1989; 320:23-8
- Tominaga K, Kamimura K, Takahashi K, Yokoyama J, Yamagiwa S, Terai S. Diversion colitis and pouchitis: a mini review. World J Gastroenterol. 2018; 24(16): 1734-47
- Kabir SI, Kabir SA, Richards R, Ahmed J, MacFie J. Pathophysiology, clinical presentation and management of diversion colitis: a review of current literature. Int J Surg 2014; 12: 1088-92