
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Pericardial hemangioma presenting as chest pain
Priya Rao BS1; Ryan Thibodeau1,2*; Abtin Jafroodifar1; Ernest Scalzetti1
1Department of Radiology, SUNY Upstate Medical University, Syracuse NY, USA.
2Department of Radiology, Albany Medical Center, Albany NY. State University of New York Upstate Medical University, 750 East Adams Street, Syracuse, New York 13210, USA.
*Corresponding Author : Ryan Thibodeau
Department of Radiology, SUNY Upstate Medical University, Syracuse NY, USA.
Department of Radiology, Albany Medical Center, Albany NY, USA.
Email: DR-IR.Research@outlook.com
Received : Apr 05, 2023
Accepted : May 02, 2023
Published : May 09, 2023
Archived : www.jcimcr.org
Copyright : © Thibodeau R (2023).
Abstract
Cardiac hemangiomas are rare vascular neoplasms composed of endothelial cells that are often incidentally found in asymptomatic patients. We present a case of a young male who presented after worsening pleuritic chest pain and dyspnea on exertion. Computed tomography of the abdomen demonstrated a large, enhancing, well-defined and heterogenous epicardial mass abutting the cardiophrenic angle. On magnetic resonance imaging, a cardiac hemangioma appeared iso- to hyperintense on T1-weighted imaging and hyperintense on T2-weighted imaging with avid contrast enhancement. Enhancement is predominantly on the arterial phase though delayed or progressive enhancement may be seen. Histopathologic analysis of the resected mass revealed a pericardial hemangioma, a rare primary cardiac tumor.
Citation: Priya Rao BS, Thibodeau R, Jafroodifar A, Scalzetti E. Pericardial hemangioma presenting as chest pain. J Clin Images Med Case Rep. 2023; 4(5): 2406.
Introduction
Hemangiomas are common benign vascular tumors. As the term “hemangioma” broadly refers to vascular neoplasms, they can be found in all organs of the body with the most common types being congenital, infantile, and hepatic hemangiomas. Cardiac hemangiomas are extremely rare benign vascular malformations of the heart. The estimated incidence of primary cardiac tumors is approximately 0.02%, with pericardial hemangiomas only accounting for 2.8% of these benign tumors [1]. Although pericardial hemangiomas are most often asymptomatic and incidentally diagnosed, these tumors can also be associated with chest pain, dyspnea, weight loss. We present the clinical, radiological, and histopathological findings of a patient with a pericardial hemangioma.
Case presentation
A 22-year-old male with a past medical history of anxiety presented to the emergency department with three days of worsening left-sided, pleuritic, non-radiating chest pain that was associated with left upper extremity pruritis, dyspnea on exertion, and cough. No abnormal findings were seen on the physical examination. The laboratory workup, including CMP and CBC, was unremarkable. EKG and troponin T were also negative.
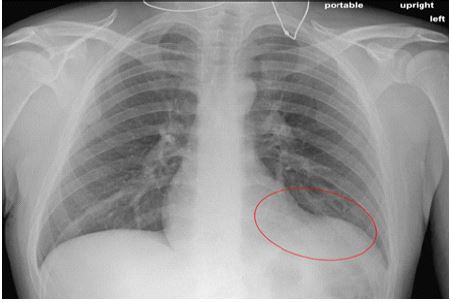
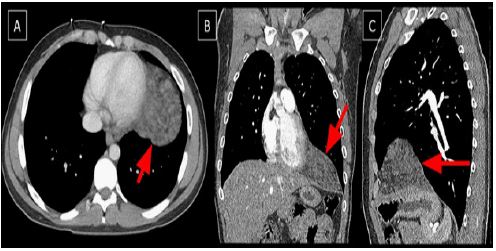
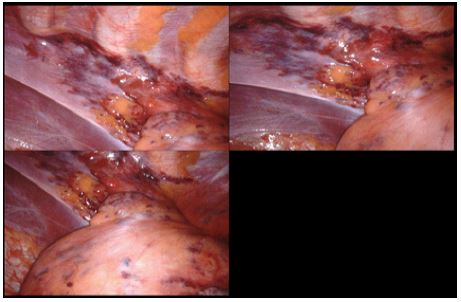
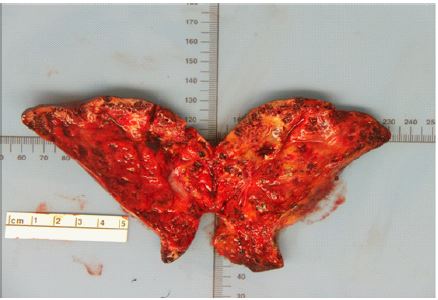
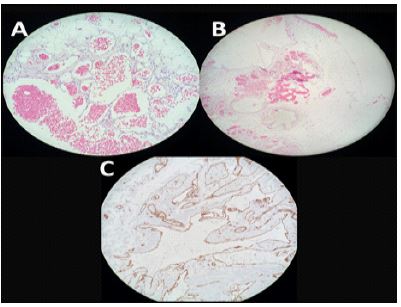
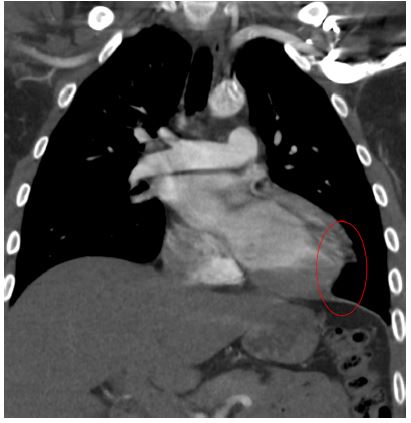
A chest radiograph demonstrated an opacity in the left lower lung with obliteration of the left heart border (Figure 1). He also had an elevated D-dimer and a Computed Tomography (CT) abdomen demonstrated a 9 x 10 x 8 cm epicardial mass with smooth borders and nodular densities in the left cardiophrenic angle, which was concerning for malignancy (Figure 2). Hematology/Oncology was consulted as the differential diagnoses based on these findings included lymphoma, germ cell tumor, or a solid malignancy. Further oncologic workup including a lactate dehydrogenase level, alpha-fetoprotein level, and serum germ cell markers were ordered and were all negative. A CT-guided transthoracic needle biopsy of the mass was performed (Figure 3), and histopathological examination revealed benign adipose tissue with patchy mild chronic inflammation. The presence of a mixed population of CD3 positive T-cells and CD20 positive B-cells indicated a reactive lymphoid infiltrate. There were no features of malignancy identified. The pathologic findings from the biopsy were suggestive of a lymphangioma or possible other benign vascular neoplasm. Given that lymphangiomas may be locally aggressive and cause mass effect on local structures (such as the adjacent neurovascular structures), the patient consented to left robotic-assisted thoracoscopic resection for complete and curative excision of the mass (Figure 4). Gross pathologic examination of the resected mass revealed a lobulated hemorrhagic mass with a spongy texture and variably sized cystic spaces (Figure 5). The histopathology of the resected mass, however, showed an abundance of blood vessels and vascular spaces intermixed with pericardial fat (Figure 6), consistent with a hemangioma.

He was admitted to the intensive care unit after surgery with subsequent placement of tracheostomy to water seal and an arterial line. Management included pain control with a patient-controlled analgesia pump, physical therapy/occupational therapy to return to his prior ambulatory baseline, and follow up imaging which showed successful resection of the mass (Figure 6). Following removal of his thoracostomy tube and lines, he was discharged home.
Discussion
Cardiac tumors are rare entities and are often classified depending on their histopathologic appearance. Among these tumors, cardiac hemangiomas are among the rarest primary tumors of the heart. Approximately only 2% to 5% of cardiac tumors are pericardial hemangiomas, which are benign vascular malformations [2]. They can arise from the endocardium, myocardium, or epicardium, most often at the level of the left ventricle and the right atrium. They occur predominantly intramural or based within the endocardium. Intramural hemangiomas are often poorly circumscribed, spongy masses that may be hemorrhagic or congested. Endocardial-based hemangiomas, however, are well-circumscribed, variably myxoid and soft [3].
Histologically, cardiac hemangiomas are composed of endothelial cells and can be categorized by their predominant vascular appearance, including cavernous, capillary, or arteriovenous. Cavernous hemangiomas are characterized by multiple thin-walled, dilated vessels. Capillary hemangiomas are predominantly composed of smaller capillary-like vessels, while arteriovenous hemangiomas are composed of thick-walled dysplastic arteries, venous-like vessels, and capillaries. Endocardial hemangiomas are usually capillary or mixed cavernous-capillary hemangiomas. They often have a myxoid stroma with a sparse inflammatory background. Intramural hemangiomas are histologically diverse and may be capillary, cavernous, or arteriovenous hemangiomas. Intramural cardiac hemangiomas may contain other tissue elements, particularly fat, and occasionally fibrous tissue, similar to intramuscular soft-tissue hemangiomas [4].
Most patients with cardiac hemangiomas are asymptomatic. As such, the tumor is often discovered as an incidental finding. Symptoms largely depend on the location and size of the hemangioma, which accounts for the wide array of potential symptoms. Symptoms often arise from compression of cardiac or adjacent structures or outflow tract obstruction. Patients most commonly present with dyspnea on exertion, though patients may also develop dysrhythmia, signs of heart failure, chest pain, jugular venous distension, pericarditis or pericardial effusion, cough, or dysphagia [5,6].
Chest radiography will likely be the first imaging modality obtained in patients presenting with many of the common complaints. While chest radiography is nonspecific, it may reveal underlying pathology that needs further investigation, especially in patients with no previous medical history. Chest radiography may demonstrate cardiomegaly and blurring of the pulmonary vasculature [6]. Transthoracic Echocardiography (TTE) findings depend on the site and size of the hemangioma. On TTE, tumors near a cardiac valve may indicate signs of outlet obstruction, such as ventricular enlargement and hypertrophy. The mass itself may be visualized as a circular/oval, hyperechoic, homogenous, mobile mass [6,7].
On non-enhanced CT, cardiac hemangiomas appear as well-defined, soft-tissue density heterogenous masses. Calcifications may or may not be seen. After contrast administration, the mass intensely enhances [7]. On T1-weighted Magnetic Resonance Imaging (MRI), hemangiomas appear as a heterogenous mass with intermediate-to-high intensity signal due to the slow blood flow within the lesion. A diffusely high intensity signal is seen on T2-weighted MRI. Following contrast administration, the mass enhances equal to the adjacent myocardium and intraventricular blood pool. There is rapid and intense contrast enhancement in the contrast arterial phase given the vascularity within the tumor. There may be delayed or progressive enhancement after contrast administration which may indicatea delayed, slow blood flow within the lesion [7,8]. To further characterize the lesion, coronary arteriography may be performed which further demonstrates an avid blood supply to the tumor. A vascular blush, especially in the setting of a capillary and/or arteriovenous-type hemangioma, indicates rapid blood flow within the lesion. Contrary to this, cavernous hemangiomas have slow flow due to large vascular spaces and therefore do not typically avidly enhance on angiography [8].
The prognosis of an untreated cardiac hemangioma is unpredictable as the size and location can vary. These tumors may involute, cease growth, or proliferate indefinitely. If these tumors continue to grow (or the heart itself structurally changes), they may lead to ventricular tachycardia, local progression, systemic dissemination, or sudden death [9]. Surgical resection is indicated for symptomatic cardiac hemangiomas and the prognosis of such patients is generally favorable. Recurrence is very rare, but has been reported in the literature [10,11]. Surgical outcome is generally favorable with usually an abrupt alleviation of the patients’ symptoms post-operatively. However, surgically resectable tumors depend on the location and adjacent involvement of the tumor. For instance, tumor involvement of the myocardium, coronary arteries, or great vessels often makes the tumor too complicated or risky for resection. Thorough evaluation of the tumor with CT and MRI by radiologists and surgeons is crucial to determine the tumor’s size, location, morphology, and involvement of adjacent mediastinal structures. Given the risks of operative repair, radiologists should be familiar with the imaging features of cardiac hemangiomas, as well as what features indicate a resectable mass.
Declarations
Acknowledgements: none.
Declarations of interest: none.
References
- McAllister H, Fenoglio J. Tumors of the Cardiovascular System. Atlas of Tumor Pathology. Series 2. Washington: Armed Forces Institute of Pathology. 1978.
- Vargis RS, Phansalkar M, Padhi S, Phansalkar D, Nair SR. Pericardial Haemangioma: A Common Tumour in an Unusual Location: Case Report and Review of Literature. J Clin Diagn Res. 2017; 11: ED15-ED17.
- Burke A, Johns J, Virmani R. Hemangiomas of the heart. A clinicopathologic study of ten cases. undefined. Published online. 1990.
- Jacob D, Pratap T, Kumar A, Rashmi R, Vishnu AK. Benign Pericardial Hemangioma-A Rare Cause of Cardiac Tamponade. Indian J Radiol Imaging. 2021; 31: 754-757.
- Brizard C, Latremouille C, Jebara VA, Acar C, Fabiani JN, et al. Cardiac hemangiomas. Ann Thorac Surg. 1993; 56: 390-394.
- Lee KJ, Shin JH, Choi JH, Lee J, Kim TY, et al. A Case of Arteriovenous Type Cardiac Hemangioma. Korean J Intern Med. 1998; 13: 123-126.
- Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR. Primary cardiac and pericardial neoplasms: Radiologic-pathologic correlation. Radiographics. 2000; 20: 1073-103; quiz 1110-1, 1112.
- Newell JD, Eckel C, Davis M, Tadros NB. MR Appearance of an arteriovenous hemangioma of the inverventricular septum. Cardiovasc Interv Radiol. 1988; 11: 319-321.
- Tomizawa Y, Endo M, Nishida H, Kikuchi C, Koyanagi H, et al. Reconstruction of the left ventricle in a patient with cardiac hemangioma at the apex. Ann Thorac Surg. 2001; 71: 2032-2034.
- Colli A, Budillon AM, DeCicco G, Agostinelli A, Nicolini F, et al. Recurrence of a right ventricular hemangioma. J Thorac Cardiovasc Surg. 2003; 126: 881-883.
- Cabot RC, Scully RE, Mark EJ, McNeely BU, Ryan TJ, et al. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 4-1983. A 15-year-old girl with a right ventricular mass. N Engl J Med. 1983; 308: 206-214.