
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Acinetobacter baumannii: A non-classical case with
an unregular management
Fatima A Dirani1*; Hadia M Abou Hamdan1; Racha S Zaraket2; Khalil I Maatouk2; Noura M Shakaroun3
1Faculty of Medical Sciences, Lebanese University, Lebanon.
2Faculty of Medicine, Balamand University, Lebanon.
3Pulmonologist and ICU Physician, Private Hospital, Lebanon.
*Corresponding Author : Fatima A Dirani
Faculty of Medical Sciences, Lebanese University, Lebanon.
Email: fatimadirani14@gmail.com
Received : Apr 04, 20230
Accepted : May 03, 2023
Published : May 10, 2023
Archived : www.jcimcr.org
Copyright : © Dirani FA (2023).
Abstract
Introduction: Acinetobacter is a gram negative cocco-bacillus that is ubiquitous and can be found in hospital settings. A baumannii can colonize ICU wards in hospitals leading to infection of multiple systems in hospitalized patients including the skin, soft tissue, urinary tract, and mainly the respiratory tract. Pneumonia caused by A. baumannii is a threatening condition in mechanically ventilated patients.
Case description: A 47-year-old man had a sudden cerebro-vascular accident that lead to a decreased level of consciousness and intubation of the patient. Few days later he started deteriorating and was discovered to develop a necrotizing pneumonia mainly of the right lung. The causative agent was found to be multi-drug resistant organism A. baumannii and was treated successfully with a combination of antibiotics and surgical lobectomy.
Discussion: When facing a complicated case of necrotizing pneumonia caused by a multi-drug resistant organism in a mechanically ventilated patient, it is required to think out of the box and considering treatment options that are not used in daily cases. Thus, antibiotic combination therapy with lobectomy was the management of choice for such patient.
Conclusion: Decreasing the frequency of nosocomial infections is becoming a must in the countries of the developing world. This requires cooperation of physicians and infection control specialists.
Keywords: Acinetobacter baumannii; Necrotizing pneumonia; Multi-drug resistance; Lobectomy.
Citation: Dirani FA, Abou Hamdan HM, Zaraket RS, Maatouk KI, Shakaroun NM. Acinetobacter baumannii: A non-classical case with an unregular management. J Clin Images Med Case Rep. 2023; 4(5): 2408.
Introduction
The genus Acinetobacter was discovered in 1971. With time more species are being discovered due to the DNA hybridization. It is gram-negative, non-spore-forming, nonmotile, nonfermentative, aerobic cocco-bacillary germ. An important element that differentiates Acinetobacter from other gram negative organisms such as Pseudomonas, Neisseria, and Moraxella is that Acinetobacter species are oxidase negative. It is considered ubiquitous because it can be isolated from different natural reservoirs such as soil, water and animals. Within the hospitals, it is being isolated from sinks, trolleys, suctioning equipment, ventilators, food and others.
Epidemiologically, Acinetobacter species can be colonizing the skin of 40% of healthy adults mainly those working within hospitals. Also, it can be isolated from the respiratory tracts of humans. This later is the most frequent site of infection [1].
In particular, Acinetobacter baumannii poses a significant risk for ICU patients who are chronically ill and are exposed to different hospital equipment such as ventilators, catheters, sutures and others.
Pneumonia is the main threat of ICU admitted patients especially those who are mechanically ventilated due to the ability of A. baumannii to form biofilms on endotracheal tubes and lead to lower respiratory tract colonization and infection. Rarely do A. baumannii result in necrotizing pneumonia which is the case of the patient presented in this article.
Case presentation
History and presentation
A case of 47 years old male, whose medical history comprises of hypertension well controlled on Amlodipine 5 mg and Bisoprolol 5 mg with hypothyroidism treated with Levothyroxine, presented to a peripheral health care facility complaining of a sudden onset of severe headache. Soon after his arrival to that hospital, he had sudden loss of consciousness. Patient was immediately intubated due to low Glasgow Coma Scale and failure of maintenance of secured airways.
Vital signs after intubation were as follows: SpO2 = 97% on FiO2 = 40% and BP 16/9. Workup started to investigate the event with an ECG (electrocardiography) that showed no abnormalities with a regular sinus rhythm. This was followed by a CT (computed tomography) scanner of the brain showing a 21 mm intra-parenchymal hemorrhage at the level of the posterior aspect of the midbrain associated with intraventricular bleed seen at level of lateral and fourth ventricles.
At that hospital, patient was admitted to the ICU, but 5 days later and due to the poor medical equipment at that facility, the patient was transferred intubated to our hospital and admitted to the ICU under the supervision of our medical team composed of a neurosurgeon and an intensive care specialist.
Diagnostic focus and assessment
Upon his arrival and after thorough assessment of the patient’s history and clinical state, the neurosurgeon decided that no interventions are needed at this state. On the other hand, a chest X-ray was done revealing mild basal infiltrates of the right lung. Also, a cardiologist was consulted to perform a cardiac echography that may unveil an underlying disease, but the results came back with an ejection fraction of 60% and normal valves. Patient was still intubated and maintained on intravenous antibiotics (ceftriaxone and vancomycin).
Few days later, the patient developed high grade fever associated with increased secretions from the endotracheal tube and an increase in the oxygen requirements. Immediately, blood samples were taken and sent for laboratory testing that showed an elevation in inflammatory markers (results shown in Table 1). A portable CXR was done and revealed right lower lobe consolidation suggesting lobar pneumonia associated with right sided pleural effusion (image not available). Moreover, a Deep Tracheal Aspirate (DTA) sample was taken for culture.
Before the results of the DTA culture came back, the patient was shifted from ceftriax one and vancomyc in to linezolid and meropenem. Despite this change, the fever did not show spacing so a multi-drug resistant organism was suspected.
Table 1: Laboratory results of the patient following the febrile episode.
| Test | Result | Test | Result |
|---|---|---|---|
| Hemoglobin (g/L) | 10.6 | BUN (mg/dL) | 20 |
| White blood cells (cu/mm3) | 18,400 | Creatinine (mg/dL) | 0.9 |
| Hematocrit (%) | 33 | Sodium (mEq/L) | 139 |
| Mean cell volume (fL) | 80 | Potassium (mEq/L) | 4.7 |
| Platelets (cu/mm3) | 250,000 | HCO3 (mEq/L) | 18 |
| Neutrophil (%) | 63 | Chloride (mEq/L) | 100 |
| Lymphocyte (%) | 33 | CRP (mg/dL) | 250 |
| Eosinophil (%) | 0 | SGPT (IU/L) | 27 |
Table 2: Antibiogram of Acinetobacter baumannii present in DTA culture of the patient.
| Drug | Susceptibility |
|---|---|
| Colistin | Sensitive |
| Amikacin | Resistant |
| Gentamycin | Resistant |
| Imipenem | Resistant |
| Piperacillin/Tazobactam | Resistant |
| Ceftazidime | Resistant |
| Cefepime | Resistant |
| imethoprim/Sulfamethoxazole | Sensitive |
| Ciprofloxacin | Resistant |
| Tetracycline | Resistant |
| Tigacycline | Intermediate |
Later, DTA culture came back showing Acinetobacter baumanniiwith multi-drug resistance according to the antibiogram shown in Table 2.
Accordingly, infectious disease consultant suggested shifting to intravenous Colistin and Bactrim for a total of 6 weeks.
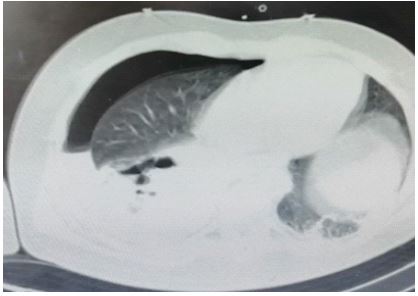
Also, CT scan of the chest was done (Figure 1) and revealed right hydro-pneumothorax (3 cm) in thickness with large consolidation in the right lower lobe and a 3 cm cavitary lesion in the middle lobe of right lung with in filtrates in the posterior segment of the lower lobe of the left lung.
Therapeutic focus and assessment
Based on the previously mentioned results, the patient was started on Colistin and high dose extended infusion of meropenem with Trimethoprim/Sulfamethoxazole (TMP-SMX). To be added, a chest tube was inserted to the right lung and pleural fluid drained and sent to analysis which showed an exudative fluid that was most probably due to a para-pneumonic effusion. Also, this fluid was sent to culture that came back negative. Later TMP-SMX was discontinued due to the occurrence of acute kidney injury.

Then bronchoscopy was done with Broncho-alveolar lavage showing the following:
- >100,000 CFU/ml Acinetobacter baumannii (antibiogram with same sensitivity as DTA culture done earlier)
- Acid fast bacilli stain was negative
- Galactomannan assay was negative ruling out aspergellosis
- PCR for non-tuberculous mycobacteria was negative
One week later, despite the double coverage of the germ with Colistin and Bactrim, the inflammatory markers were still increasing and the patient was still febrile, so a series of CT scans of the chest with DTA cultures were taken to check response to therapy.
The DTA cultures taken also showed the persistence of the Acinetobacter baumannii, so patient was started on nebulized Polymyxin which was also uneffective in eliminating the germ.
Patient was deteriorating clinically with no response to antibiotics with inflammatory markers rising to CRP= 270 mg/dL and WBC= 24000 cu/mm3 so the decision was taken for decortication. A cardiothoracic surgeon performed the operation successfully.
After surgery, patient started improving rapidly. Repeated CT scan of the chest showed a decrease in the size of the previously seen cavitary lesions and the inflammatory markers had a drop to a CRP of 24 mg/dL and WBC of 13000 cu/mm3
Two DTA cultures done one week apart following the surgery showed absence of Acinetobacter baumannii.
The patient continued to improve clinically and he was fortunately extubated. No more febrile episodes took place and minimal respiratory secretions were noticed. Also, the chest tube was removed. He stayed at the hospital until he completed the course of antibiotics for a total of 6 weeks and was transferred to a nursing facility.
Discussion
Acinetobacter baumannii which is a gram negative ubiquitous organism, has been found to cause infection in multiple systems of the human body mainly the skin, soft tissue, respiratory tract and digestive system. It is known that A. baumannii has been isolated from different units within hospitals especially the ICU where it poses a great risk on patients who are mechanically ventilated. According to a study done in the United States about 6% of Ventilator-Assocaited Pneumonias (VAP) are caused by A. baumannii [2].
The patient described above suffered from ventilator associated pneumonia and what made it worse is the fact that the germ was a multi-drug resistant organism that was resistant to several combinations of antibiotics. By definition, Acinetobacter is considered multi-drug resistant when it is not susceptible to at least one agent in three or more antibiotic groups including third- or fourth-generation cephalosporins, aminoglycosides, carbapenems, fluoroquinolones, ampicillin-sulbactam, piperacillin-tazobactam [3]. A study performed in Lebanon found out that infections caused by multi-drug resistant A. baumannii increased markedly since 2007 so that it became the number one cause of VAP in hospitals [4].
Moreover, as mentioned above the patient developed necrotizing pneumonia which is a very rare complication of A. baumannii infection. Necrotizing pneumonia is an inflammatory process of the lung tissue that leads to consolidation, necrosis and formation of multiple cavities that compresses the bronchial and pulmonary blood supply leading to loss of lung parenchyma. Loss of blood supply to the area leads to poor antibiotic delivery to the lung tissue and ending by an uncontrolled infection. This is why surgical approach was the last life-saving option available during the treatment of the above patient.
This required the cooperation of the whole medical team in order to save his life. Infectious disease specialist was responsible for choosing the appropriate antibiotics regimen, pulmonologists and ICU specialists were responsible for rapid response to any clinical deterioration and keeping an eye on the therapy effectiveness, and finally the cardiothoracic surgeon who performed the lobectomy which was a great turning point in the management of the patient and let the team reach to a favorable outcome.
Regarding the antibiotic options for Acinetobacter, the choice of the drug depends on the location of the infection, the state of the patient (comorbidities and severity of infection), and on the susceptibility profile of the germ. For the case mentioned above where the germ is highly resistant and the infection is a severe necrotizing pneumonia, the optimal option is a triple therapy consistent of a combination of high-dose extended-infusion ampicillin-sulbactam with any two of the following: high-dose extended infusion of meropenem, polymyxin, or a tetracycline derivative. To be mentioned that some studies recommend that colistin be given inhaled due to the low bioavailabilty of intravenous form in the lung parenchyma. To be added, that surgical intervention has multiple indications one of which is an unresponsive necrotizing pneumonia to the suitable antibiotic protocol.
Conclusion
Acinetobacter baumannii is posing a great threat for the hospitalized patients in the developing world, especially cases of multi-drug resistant A. baumannii that requires prolonged courses of non-classical antibiotic combinations. Clinicians and infection control teams must augment their efforts to minimize such outbreaks that are expensive on both the humanitarian and financial aspects.
Declarations
Declaration of interest: We declare that we have no conflict of interest.
Informed consent: An informed consent was signed by the patient family and they agreed to publish the above information and data.
References
- Hartzell JD, Kim AS, Kortepeter MG, Moran KA. Acinetobacter pneumonia: A review. Med Gen Med. 2007; 9: 3.
- Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Crit Care Med. 1999; 27: 887-892.
- Centers for Disease Control and Prevention, Antimicrobial-resistant phenotype definitions. 2022. [Online]. Available: https://www.cdc.gov/nhsn/pdfs/ps-analysis-resources/phenotype_definitions.pdf . [Accessed August 2022].
- Kanafani ZA, Zahreddine N, Tayyar R, Sfeir J, Araj GF, et al. Multi-drug resistant Acinetobacter species: A seven-year experience from a tertiary care center in Lebanon. Antimicrob Resist Infect Control. 2018; 22: 7.