
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Peripheral facial paralysis as the first manifestation
of temporal bone metastasis
Hugo Barcelos Figueiredo1,2*; Filipa Carvalho1,2; Carmo Miguéis1,2; António Carlos Miguéis1,2; Jorge Miguéis1,2
1Otorhinolaryngology Department of Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal.
2University Clinic of Otorhinolaryngology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
*Corresponding Author : Hugo B Figueiredo
Otorhinolaryngology Department of Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal.
Email: hugo.b.f@live.com.pt
ORCID: 0000-0002-4901-9568
Received : Apr 15, 2023
Accepted : May 04, 2023
Published : May 11, 2023
Archived : www.jcimcr.org
Copyright : © Figueiredo HB (2023).
Abstract
Peripheral facial paralysisis a rare manifestation of Temporal Bone Metastasis (TBM). We report a case of peripheral facial paralysisas the first manifestation of TBM of breast cancer.
A 55-year-old female patient was admitted to the emergency room with left peripheral facial paralysis with a day of evolution and no other symptoms. The patient denied any viral infection in the past months and had a personal history of breast cancer in 2007. Cranio-encephalic computed tomography scan demonstrated multiple bone lesions indicative of metastatic lesions. The positron emission tomography-computed tomography scan showed extensive bilateral lung, lymph node, hepatic, and bone metastases of a lytic nature, and a large hypermetabolic mass centered in the hilar region of the left lung associated with pleural effusion, suggestive of a primary lesion. A supraclavicular lymph node and liver biopsy were performed which showed metastasis of breast carcinoma.
Keywords: Peripheral facial paralysis; Temporal bone metastasis; Breast cancer; First manifestation.
Citation: Figueiredo HB, Carvalho F, Miguéis C, Miguéis AC, Miguéis J, et al. Peripheral facial paralysis as the first manifestation of temporal bone metastasis. J Clin Images Med Case Rep. 2023; 4(5): 2409.
Introduction
Peripheral Facial Paralysis (PFP) is commonly diagnosed in the emergency room. Its incidence ranges from 20 to 30 cases per 100.000 individuals/year) [1] and, despite being a benign condition in most cases (up to 70% are labeled as idiopathic [2], it could be the first manifestation of a distant carcinoma, such as breast cancer [3].
The patient with idiopathic PFP manifests suddenly painless facial muscle weakness, with lower motor neuron distribution, and an innocent otorhinolaryngological and neurological examination. If the clinical history and physical examination are consistent, there is no need for radiological or laboratory tests. However, PFP can occur as a result of trauma, infection (e.g. Ramsay Hunt Syndrome or neuroborreliosis), autoimmune disease (e.g. Guillain-Barré syndrome or multiple sclerosis), or neoplasm [4,5]. Some types of neoplasms can metastasize to the temporal bone, being the most common primary tumor locations, breast cancer (19.6%), lung cancer (16.1%), and prostatic cancer (8.6%) [6]. These etiologies should be considered, even if they are uncommon, particularly in cases where the course of PFP is atypical and/or the patient’s personal history is relevant [4].
Case report
A 55-year-old female patient was admitted to the emergency room for left PFP (House-Brackmann scale, grade IV), with one day of evolution and no other symptoms. The patient denied any history suggestive of viral infection in the past months and had a personal history of breast cancer in 2007. She was treated with neoadjuvant chemotherapy followed by left modified radical mastectomy. Subsequently, the patient had been treated with hormone therapy with tamoxifen, having been discharged and considered disease free. The physical examination was unremarkable, except for a left PFP. She was treated with 60 mg daily of oral steroids (1 mg/day/Kg) for 10 days and eye protection with an improvement of PFP (House-Brackmann scale, grade III). After six weeks of treatment, the patient went to the emergency room again and a physical examination revealed worsening PFP (House-Brackmann scale, grade V).
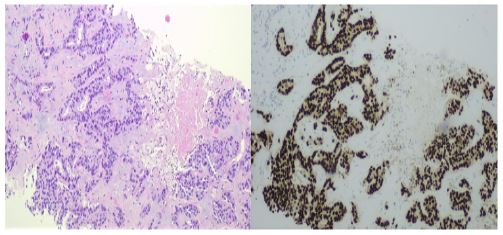
A cranio-encephalic computed tomography scan and magnetic resonance imaging were performed, revealing multiple bone lesions in the left mastoid, right parietal bone, frontal bone, and clivus region (Figure 1). This was suggestive of metastatic lesions of occult primary neoplasia. The positron emission computed tomography scan (Figure 2) demonstrated extensive bilateral lung, lymph node, hepatic, and bone metastases of a lytic nature. It also presented hypermetabolic nodular formations in the thyroid lobes and a lesion adjacent to the sigmoid colon with suspicious imaging features. A large hypermetabolic mass centered in the hilar region of the left lung, associated with pleural effusion, was suggestive of the primary lesion. A supraclavicular lymph node and liver biopsy were performed. Histopathological and immunohistochemical analysis revealed a HER2-negative, estrogen receptor, and progesterone-positive breast carcinoma (Figure 3).
The patient was referred to the Gynecology/Oncology department and underwent systemic palliative chemotherapy with paclitaxel. After 9 months since the diagnosis and under palliative treatment, there was no improvement in PFP, and a continuous degradation of the patient’s general state was observed.
Discussion
PFP has an equal incidence in both sexes and affects both sides of the face [7]. The majority (up to 70%) of the PFP is considered idiopathic [2]. Nonetheless, PFP can result from infectious diseases [8], such as neuroborreliosis or Ramsay-Hunt syndrome, trauma, autoimmune diseases (such as Guillain-Barré syndrome and multiple sclerosis), and neoplasms [4,5].
Metastatic tumors to the temporal bone as the first manifestation of an occult primary neoplasm are rare and the most common sites of origin are the breasts, lungs, kidneys, stomach, and prostate [3,4]. This is no surprise, since these types of neoplasms are some of the most common cancers, as stated by Jones et al [6]. The main symptoms are PFP, hearing loss, otalgia, tinnitus, and vertigo, which may occur isolated or in association [3,4]. Patients can be asymptomatic in 32% of the cases according to Jones et al [6] and in a review of metastatic lesions of the temporal bone, a male predominance was observed (54.9%) [6].
The complete evaluation of a patient presenting PFP should include a detailed medical history, neurological examination, ear inspection, and otoscopy.
Metastatic lesions may occur through hematogenous dissemination, leukemic or lymphomatous spread, direct extension, or meningeal carcinomatosis from a primary intracranial lesion [9]. Hematogenous spread is the most common form of dissemination [9]. As found in the study carried out by Gloria-Cruz et al [10], our patient had other sites of metastasis beyond the temporal bone, however, the PFP was the only clinical manifestation.
In our patient’s case, considering the sudden onset of PFP and an innocent physical examination, the patient was initially diagnosed with idiopathic unilateral PFP, therefore, no laboratory or imaging testing was requested. Due to the absence of response to treatment, her medical history, and theworsening of the PFP, an additional investigation was performed.
Patients with PFP secondary to neoplastic etiology have a poor prognosis, with no evidence of improvement with the established therapy [11], as was our case. Most patients have a delay in etiological diagnosis which unfortunately worsens the prognosis [3,5,11]. Although idiopathic etiology is the most common cause of PFP, the metastatic disease should be considered in patients with PFP and a personal history of neopl.


Take home messages
A metastatic tumor should be considered a differential diagnosis in patients with peripheral facial paralysis or otologic symptoms, even if the personal history of the tumor dates back several years.ssssss
Declarations
Authors contributions HBF: review the literature and wrote the draft of the manuscript. Followed the patient in the out patient setting.
HBF, FC, CM, AM, and JM: Critical review of the article.
Acknowledgements: The authors would like to acknowledge Dr. Guilherme Fontinha, Pathological Anatomy resident from Centro Hospitalar e Universitário de Coimbra.
Funding source: The authors do not receivea specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Protection of humans and animals: The authors declare that the procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and to the Helsinki Declaration of the World Medical Association updated in 2013.
Competing interests: The authors declare that there is no competing interest.
Patient consent: Consent to publish the case report was not obtained. This report does not contain any personal information that could lead to the identification of the patient.
Data confidentiality: The authors declare having followed the protocols in use at their working center regarding patients´ data publication.
References
- Volk GF, Pantel M, Guntinas-Lichius O. Modern concepts in facial nerve reconstruction. Head Face Med. 2010; 6: 1-11.
- Plumbaum K, Volk GF, Boeger D, et al. Inpatient treatment of patients with acute idiopathic peripheral facial palsy: A population-based healthcare research study. Clin Otolaryngol. 2017; 42: 1267-1274.
- Hosseini M, Vafaei E, Ara RM, Asghari A, Nafissi N. Bell’s Palsy As a Rare First Presentation of Breast Cancer. 2016; 3: 66-69.
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical Practice Guideline: Bell’s Palsy Otolaryngol Neck Surg. 2013; 149: S1-S27.
- Kumar S, Verma S, Giridhar P, Phulware RH, Barwad A, Kumar R. Bell’s Palsy in a Treated Case of Breast Cancer—A Rare Presentation of Recurrence. Indian J Surg Oncol. 2020; 11: 40-43.
- Jones AJ, Tucker BJ, Novinger LJ, Galer CE, Nelson RF, et al. Metastatic Disease of the Temporal Bone: A Contemporary Review. Laryngoscope. 2021; 131: 1101-1109.
- Zimmermann J, Jesse S, Kassubek J, Pinkhardt E, Ludolph AC, et al. Differential diagnosis of peripheral facial nerve palsy: a retrospective clinical, MRI and CSF-based study.J Neurol. 2019; 266: 2488-2494.
- Abdel-Aziz M, Azab NA, Khalifa B, Rashed M, Naguib N. The association of Varicella zoster virus reactivation with Bell’s palsy in children. Int J Pediatr Otorhinolaryngol. 2015; 79: 328-331.
- Lan MY, Shiao AS, Li WY. Facial paralysis caused by metastasis of breast carcinoma to the temporal bone. J Chin Med Assoc. 2004; 67: 587-590. http://www.ncbi.nlm.nih.gov/pubmed/15720075.
- Gloria-Cruz TI, Schachern PA, Paparella MM, Adams GL, Fulton SE, et al. Metastases to Temporal Bones From Primary Nonsystemic Malignant Neoplasms. Arch Otolaryngol Neck Surg. 2000; 126: 209.
- Nguyen CN, Mallepally N, Tabilona JR, Lu LB. Not So Benign Bell’s Palsy: Malignant Peripheral Nerve Sheath Tumor of the Facial Nerve Involving the Temporal Bone. J Gen Intern Med. 2021; 36: 1102-1105.