
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Juvenile nasopharyngeal angiofibroma:
A case report and literature review
Hemant Adhikari1*; Prajjwal Raj Bhattarai2; Sujan Singh Chhetri3; Nimesh Amatya4; Bikash Khadka5
1Junior Consultant, Department of Anesthesia and Pain Management, Nepal Mediciti Hospital, Nepal.
2Consultant, Department of Anesthesia and Pain Management, Nepal Mediciti Hospital, Nepal.
3Consultant, Department of Otorhinolaryngology & Head and Neck Surgery, Nepal Mediciti Hospital, Nepal.
4Resident, Departmentof Otorhinolaryngology & Head and Neck Surgery, Nepal Mediciti Hospital, Nepal.
5Registrar, Department of Anesthesia and Pain Management, Nepal Mediciti Hospital, Nepal.
*Corresponding Author : Hemant Adhikari
Junior Consultant, Department of Anesthesia and Pain Management, Nepal Mediciti Hospital, Nepal.
Email: hemantadhikari@gmail.com
Received : Apr 20, 2023
Accepted : May 05, 2023
Published : May 12, 2023
Archived : www.jcimcr.org
Copyright : © Adhikari H (2023).
Abstract
Introduction: Juvenile Nasopharyngeal Angiofibroma (JNA) is a rare tumor that affects almost exclusively adolescents and young males and is locally aggressive despite being benign. It presents with symptoms like epistaxis, and nose blocks. A preoperative biopsy is not recommended as the tumor is highly vascular. Diagnosis relies on imaging modalities.
Case presentation: We present a case of a 14-year-old male who presented with nosebleeds, bilateral nasal blockage, and occasional headaches. Radiological evaluation using a Contrast CT scan revealed a mass in the nasopharynx, which was suspected to be an angiofibroma. The patient underwent preoperative embolization and endoscopic removal of the mass under general anesthesia (hypotensive anesthesia) 24 hours later.
Clinical discussion: JNA should be considered in adolescent males who present with a history of nasal blockade and epistaxis.
Conclusion: JNA is a rare benign tumor that presents with nasal blockade and epistaxis and that can cause intractable bleeding if an inadvertent biopsy is done pre-operatively. Diagnosis is clinical and radiological. Definitive treatment is the surgical removal of the tumor, either open or endoscopically. Pre-operative embolization of the maxillary artery can be done to minimize surgical blood loss.
Keywords: Embolization; Hypotensive anesthesia; Juvenile Nasopharyngeal Angiofibroma (JNA); Vascular tumor.
Citation: Adhikari H, Bhattarai PR, Chhetri SS, Amatya N, Khadka B, et al. Juvenile nasopharyngeal angiofibroma: A case report and literature review. J Clin Images Med Case Rep. 2023; 4(5): 2413.
Introduction
Juvenile Nasopharyngeal Angiofibroma (JNA), a rare benign tumor that occurs almost exclusively in adolescents and young men, is locally aggressive and accounts for 0.5% of head and neck tumors [1]. JNA typically presents with symptoms such as epistaxis, obstructive symptoms, and chronic otomastoiditis. Contrast CT used for diagnosis of JNA, will show a vividly enhancing soft-tissue mass centered on the sphenopalatine foramen. MRI Shows low signal intensity on T1-weighted images, heterogeneous intermediate signal intensity on T2-weighted images, and avid enhancement with flow voids on contrast-enhanced images. The management of JNA is tricky, as biopsy is contraindicated because of the risk of intractable bleeding at the puncture site. The role of pre-operative embolization of the internal maxillary artery is important to aid in hemostasis during surgical resection [2]. The treatment of choice for JNA is surgical resection through open or endoscopic approaches. In this case report we discuss the multidisciplinary involvement of interventional radiologists, anesthesiologists, and otorhinolaryngologists in the successful management of JNA.
This case report has been reported in line with the SCARE 2020 standards [3].
Presentation of the case
We report a case of a 14-year-old male who presented to the Otorhinolaryngology OPD with a history of bilateral nasal obstruction, on and off epistaxis from the right nostril, and headache. The headache was intermittent and was relieved by Paracetamol. Nasal bleeding was spontaneous, scanty, and had been on and off for the past three months. Mouth breathing was evident, and the patient’s father revealed it was more while sleeping. There was no pallor and no external facial deformity. General physical examination was normal. Orodental examination was normal. Endoscopic examination revealed whitish, pale mass was seen arising from the area of left sphenopalatine foramen extending inferiorly to the floor of the nose,
CT was advised which showed a large isodense mass measuring 5.98(AP) x4, 17(CC)x2. 36(T) in the nasopharynx centered around the left sphenopalatine foramen. The mass had strong and heterogeneous enhancement, in the post-contrast study. The features were suggestive of Juvenile nasopharyngeal angiofibroma of the nasopharynx with minimal extension to the proximal part of the left pterygopalatine fossa through the widened left sphenopalatine foramen. Extension of this mass to the left nasal cavity, oropharynx, and left ethmoidal and sphenoidal sinus (Fisch Stage II).
Blood nnvestigations were normal.
Case management
A pre-anesthetic evaluation was done and blood was arranged.
Pre-surgery embolization of the internal maxillary artery feeding the tumor was done with gel foam slurry. Surgery was done under General anesthesia with Endotracheal intubation. Two wide bores (16 G) cannula were accessed in anticipation of the bleeding. Anesthesia was maintained with Oxygen, isoflurane, and intermittent dosing of Vecuronium. Invasive blood pressure monitoring was done. Dexmedetomidine infusion was started at the dose of 0.03-0.07 mcg/kg/hr to keep Heart Rate (HR) between 70-80/min and MAP target of 55 mmHg (hypotensive anesthesia) to reduce intraoperative bleeding in the surgical field, maintain the surgical plane and to execute the surgical procedure. Blood loss was closely monitored. The duration of the surgery was three hours. Intraoperative blood loss was 50 ml.
Surgical procedure
Endonasal surgical approach was done using Hopkins 0 degree rigid scope and coblation. A whitish, pale mass was seen arising from the area of left sphenopalatine foramen extending inferiorly to the floor of the nose, superiorly into the ethmoids eroding the floor and anterior wall of the left sphenoid sinus, posteriorly occupying the whole of the nasopharynx extending to the opposite posterior choanae. Medially the septum was pushed to the opposite side and laterally extending into the medial pterygopalatine fossa. Modified Denker’s approach with exposure of left maxillary antrum. Left nasolacrimal duct was transected and flushed to the bone. The posterior wall of the maxillary sinus was removed with Kerrison and careful dissection of the fossa was done. The internal maxillary artery supplying the tumor was identified laterally and ligated with Liga clips and transected in between.
Tumor was carefully dissected of the fossa, sphenopalatine foramen, ethmoids, sphenoid sinus, and septum maintaining hemostasis and coagulation of other vessels. The portion of tumor encroaching the opposite posterior choanae was dissected carefully from the posterior septum as well.
Tumour was removed en bloc through the oral cavity. Bilateral anteroposterior nasal packing was done with Rapid Rhino.
The patient was extubated and shifted to the Postoperative ward. The postoperative stay was uneventful. The patient was discharged on third post operative day. Post operative follow up at one month was normal on endoscopic examination.
Histological findings
Gross: The specimen was solid, grey-brown nodule measuring 4.0 x 3.0 x 3.0 cm. The outer surface appeared smooth grey-white to grey-brown and the Cut section showed a smooth, grey-white surface.
Microscopic: The Section examined showed tissue lined by stratified squamous epithelium. The subepithelium showed a tumor with a stromal and vascular component. Stroma consisted of fibroblastic cells with oval nuclei, vesicular chromatin, and occasionally conspicuous nucleoli. Mitosis or necrosis was not seen. The blood vessels were of various sizes and shapes, ranging from slit-like capillaries to irregularly dilated vessels. A final diagnosis of nasopharyngeal tissue consistent with Nasopharyngeal angiofibroma was made.
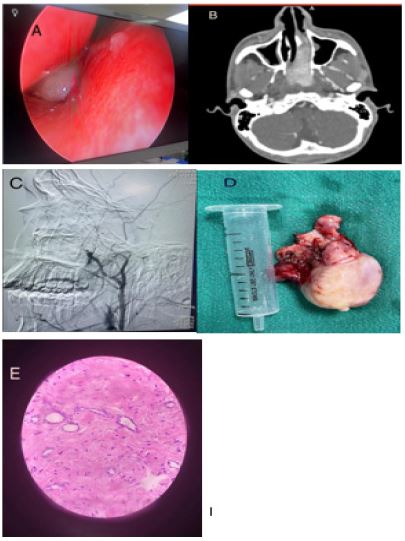
B: Contrast CT showing enhancement of the mass
C: Angiography and embolization of Internal maxillary Artery
D: Excised mass
E: Microscopic picture
Discussion
Although benign, Juvenile Nasopharyngeal Angiofibroma (JNA) is a tumor that poses a significant local threat due to its highly vascular nature and tendency to grow and spread aggressively within the surrounding tissues. It occurs exclusively in males, typically in the age range of 5-25 years, as the tumorexpresses androgen and testosterone receptors, but lacks estrogen receptors. Few case reports in females have also been described [4]. Originating from the sphenopalatine foramen, JNA spreads locally and can present with symptoms such as nasal blockage, epistaxis, facial swelling, otomastoiditis, anosmia, and dacryocystitis [5]. Our case presented with nasal obstruction and epistaxis. Bony erosion is also common in JNA. It can extend into the orbit causing proptosis and intracranial extension can cause cranial nerve palsies and loss of vision [6]. The tumor is characterized by local invasiveness, but its morphological appearance can be deceivingly bland. It typically exhibits thin-walled vessels without smooth muscle, often with staghorn-shaped patterns, set in a fibrous to myxoid stroma.
The tumor may extensively involve the nasal cavity and paranasal sinuses and sometimes invade the skull base. Intraoperative bleeding can be significant and potentially life-threatening [7]. Preoperative measures to reduce blood loss, such as tumor embolization, may be clinically beneficial. In recent studies, preoperative embolization with polyvinyl alcohol has been reported to have a significant role in reducing blood loss during tumor resection, particularly in highly vascular tumors like nasopharyngeal angiofibroma [2]. Therefore, preoperative embolization of the feeder vessels with gel foam slurry was performed in our case 24 hours before the planned surgery. The use of Cellsaver for intraoperative salvage to prevent allogenic blood transfusion has also been described in the literature [8]. Radiologically, CT scans typically reveal a non-capsulated, soft tissue density mass originating from the sphenopalatine foramen, with post-contrast enhancement indicating the vascularity of the tumor which was similar to our finding. The Holman-Miller sign, which refers to the anterior bowing of the posterior maxillary wall, is a characteristic finding of Juvenile Nasopharyngeal Angiofibroma (JNA) on axial CT imaging. This sign is caused by the tumor located in the pterygomaxillary space, which pushes the posterior maxillary wall anteriorly.
MRI is considered superior to CT in detecting the intracranial extension of a tumor into the soft tissues of the skull base. The characteristic imaging findings of Juvenile Nasopharyngeal Angiofibroma (JNA) on MRI include low signal intensity on T1-weighted images, heterogeneous intermediate signal intensity on T2-weighted images, and avid enhancement with flow voids on contrast-enhanced images. These features, in addition to the patient’s age, can help differentiate JNA from other nasopharyngeal lesions. Postoperatively, MRI is also useful in detecting any residual or recurrent tumor, as well as monitoring the effects of radiotherapy. Therefore, MRI is an important imaging modality in the diagnosis and management of JNA [9]. Angiography can be useful for pre-operative embolization to identify major feeding vessels and is typically performed between 24 and 72 hours before surgery.
Surgical resection is the primary treatment of JNA but radiotherapy can be an adjuvant in case of residual or recurrent disease and in the setting of tumors with intracranial extensions where they may not be completely resectable.
There have been reports of a rare malignant transformation of Juvenile Nasopharyngeal Angiofibroma (JNA), with most cases resulting in well-differentiated tumors after undergoing radiotherapy. However, there are also cases where JNA transforms into undifferentiated sarcomas, which are associated with a poorer prognosis [10]. Hormonal therapy in the way of androgen receptor blockers such as flutamide has also been described which helps to reduce the tumor size prior to surgical resection and in cases of recurrence but they aren’t curative on their own [11]. Large nasal masses can have a differential diagnosis that includes sinonasal polyp, neurofibroma, hypertrophy of adenoids, and malignant neoplasms like nasopharyngeal carcinoma, lymphoma, or rhabdomyosarcoma. Nasopharyngeal carcinoma typically presents as a nonhomogeneous mass arising from the nasopharyngeal mucosa or submucosal space, with erosion of the skull base or intracranial extension. Lymphoma may be associated with lymphadenopathy, and a tumor mass can be seen in the nasopharynx or Waldeyer’s ring. Rhabdomyosarcoma appears as a soft-tissue mass that erodes the bone, with mild enhancement on CT and marked enhancement on MRI. Therefore, multiplanar imaging with CT and/or MRI is important in differentiating these various entities and determining the most appropriate management approach [12]. Specific radiological features of JNA, such as a soft tissue mass in the nasopharynx and pterygopalatine fossa, along with the erosion of the posterior osseous margin of the sphenopalatine foramen, have been identified in previous studies as indicative of JNA and were consistent with the findings in our case.
Conclusion
Though rare JNA is the most common benign tumor of the head and neck which is highly vascular, and it affects exclusively male adolescents. The diagnosis is clinical and radiological as pre-operative tissue biopsy might cause intractable bleeding. Preoperative tumor embolization is useful and can help to prevent intraoperative bleeding. Surgery either open or endoscopic is the treatment of choice which is aidedby hypotensive anesthesia.
References
- Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM. Diagnosis and treatment of juvenile nasopharyngeal angiofibroma. Eur Arch Otorhinolaryngo. 2001; 258:120–124.
- Meher R, Kathuria S, Wadhwa V, et al. Preoperative emobilisation of juvenile nasopharyngeal angiofibroma. Am J Otolaryngol. 2022; 43: 103532.
- Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, et al. SCARE Group. The SCARE 2020 Guideline: Updating Consensus Surgical CAseREport (SCARE) Guidelines. Int J Surg. 2020; 84:226-230.
- Ralli M, Fusconi M, Visconti IC, Martellucci S, de Vincentiis M, Greco A, et al. Nasopharyngeal angiofibroma in an elderly female patient: A rare case report. Mol Clin Oncol. 2018; 9: 702-704.
- Makhasana JA, Kulkarni MA, Vaze S, Shroff AS. Juvenile nasopharyngeal angiofibroma. J Oral MaxillofacPathol. 2016; 20: 330.
- Alves FRA, Granato L, Soares M, Lambert E. Surgical approaches to juvenile nasopharyngeal angiofibroma - case report and literature review. Intl. Arch. Otorhinolaryngol. 2006; 2: 162–166.
- Sánchez-Romero C, Carlos R, Díaz Molina JP, Thompson LDR, de Almeida OP, et al. Nasopharyngeal Angiofibroma: A Clinical, Histopathological and Immunohistochemical Study of 42 Cases with Emphasis on Stromal Features. Head Neck Pathol. 2018; 12: 52-61.
- Wasl H, Mc Guire J, Lubbe D. Avoiding allogenic blood transfusions in endoscopic angiofibroma surgery. J Otolaryngol Head Neck Surg. 2016; 45: 25.
- Alimli, AG, Ucar M, Oztunali C, Akkan K, Boyunaga O, et al. Juvenile Nasopharyngeal Angiofibroma: Magnetic Resonance Imaging Findings. Journal of the Belgian Society of Radiology. 2016; 100: p.63.
- Allensworth JJ, Troob SH, Lanciault C, Andersen PE. High-grade malignant transformation of a radiation-naïve nasopharyngeal angiofibroma. Head Neck. 2016; 38 Suppl 1:E2425-E2427.
- Scholfield DW, Brundler MA, McDermott AL, Mussai F, Kearns P, et al. Adjunctive Treatment in Juvenile Nasopharyngeal Angiofibroma: How Should We Approach Recurrence?. J Pediatr Hematol Oncol. 2016; 38: 235-239.
- Mishra S, Praveena NM, Panigrahi RG, Gupta YM. Imaging in the diagnosis of juvenile nasopharyngeal angiofibroma. J Clin Imaging Sci. 2013; 3:1.