
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Jejunal gastrointestinal stromal tumor, a rare small
bowel neoplasm that presents a diagnostic challenge
Pooja Mallipaddi, OMS IV1; Patrick Dolan, MS2*; Facs Kristin Dishongh3
1Medical Student, Arkansas College of Osteopathic Medicine, USA.
2General Surgeon, CHI St. Vincent Hot Springs, USA.
3Pathologist, CHI St. Vincent Hot Springs, USA.
*Corresponding Author : Patrick Dolan MS
General Surgeon, CHI St. Vincent Hot Springs, USA.
Email: poojamallipaddi@gmail.com
Received : Apr 20, 2023
Accepted : May 08, 2023
Published : May 15, 2023
Archived : www.jcimcr.org
Copyright : © Dolan P (2023).
Abstract
Small bowel neoplasms consist of adenocarcinomas, carcinoids or neuroendocrine tumors, lymphomas, Gastrointestinal Stromal Tumors (GISTs), and other sarcomas. GISTs are a type of mesenchymal tumors that arise from the intramuscular layer of the bowel wall and are considered a low-grade sarcoma. Small bowel GISTs often present with a wide variety of GI symptoms, including occult bleeding which can be difficult to localize and diagnose. There is abundant literature concerning the workup, staging, and treatment of GIST tumors, but not many emphasize the diagnostic difficulty and the importance of early detection of small bowel neoplasms. We discuss a case of an elderly woman who presented with anemia and melanotic stools secondary to a jejunal GIST that was not diagnosed on her initial admission. On a second emergency room visit six weeks later, a small jejunal GIST was found, which led to early intervention and good outcome for the patient.
Keywords: Gastrointestinal Stromal Tumors (GIST); Lower GI bleeding; Tumor imaging; Bowel resection; Jejunum.
Citation: Mallipaddi P, Dolan P, Dishongh FK. Jejunal gastrointestinal stromal tumor, a rare small bowel neoplasm that presents a diagnostic challenge. J Clin Images Med Case Rep. 2023; 4(5): 2414.
Introduction
GISTs are rare mesenchymal tumors that can arise anywhere in the GI tract but most commonly in the stomach (60%) and small bowel (30%). They constitute about 1-2% of all primary GI neoplasms [1]. They predominantly affect older adults in their late 60s and are equally common in both genders [2]. They are thought to arise from the Interstitial Pacemaker Cells of Cajal (ICCs) located in the muscularis propria layer of the bowel wall. ICCs function to aid bowel motility with their electrical slow wave activity [3]. Small bowel GISTs tend to have a greater malignant potential than gastric GISTs, and some suggest a worse prognosis [4]. Moreover, large tumors (>10 cm) exhibit a greater risk for metastasis and local recurrence. Small tumors (< 5 cm) are particularly difficult to localize and are often missed on CT scan [4,5]. The most important prognostic indicators include tumor size, mitotic rate, and anatomical location. According to the modified NIH classification of GIST, high risk categories include perforated tumors, tumor size >10 cm small bowel location, and a mitotic rate greater than 5/50 per high powered field [5].
Patients can present with a variety of symptoms including occult bleeding, abdominal distension, early satiety, and abdominal pain [6]. Physical findings are rare. Up to 18% of cases are diagnosed via incidental imaging studies in asymptomatic patients [5]. Occult small bowel bleeding cases can be very difficult to localize and diagnose. A GIST tumor should be considered in the differential diagnosis. Routine upper GI endoscopy and colonoscopy often fail to detect these small bowel neoplasms [7]. In addition, difficulties in diagnosing GIST in symptomatic patients often result in a delayed diagnosis. In this setting, metastatic disease is present in up to 20% of patients at the time of diagnosis [8].
Case presentation
An elderly female presented to the Emergency Department (ED) with diffuse, non-specific abdominal pain and bouts of dark melanotic stools, along with a past medical history of atrial fibrillation. Her medications included Eliquis. She denied both NSAID and heavy alcohol use. CT of the abdomen/pelvis with IV contrast was negative except for mild diverticulosis (Figure 1). Labs were significant for a mild anemia (hemoglobin 11.3, hematocrit 34) and a positive Fecal Occult Blood Test (FOBT). EGD and colonoscopy showed no evidence of a bleeding site. Her hospital course, however, was complicated by increasing RUQ abdominal pain. RUQ Ultrasound was normal. PIPIDA scan of the gallbladder showed a low ejection fraction of 20%, indicating biliary dyskinesia. She ultimately underwent robotic-assisted laparoscopic cholecystectomy and was discharged home with improved symptoms.

Two months later, the patient returned to the ED with worsening epigastric pain and intermittent dark stools. On examination, the patient had diffuse abdominal tenderness and was hemodynamically stable. Labs were only significant for anemia (hemoglobin 9.7, hematocrit 31.1), FOBT was not repeated. CT of the abdomen/pelvis with IV contrast showed an 3.1 cm arterial enhancing mass in the proximal jejunum (Figure 2). GI was unable to reach the lesion on repeat EGD. No tissue diagnosis was obtained preoperatively due to its small size and location.

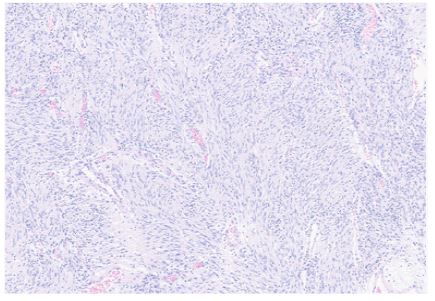
She underwent a robotic small bowel resection. Histopathology report of the jejunal mass revealed a 3.7 x 3.5 x 1.5 cm GIST (unifocal, spindle cell type, negative margins, KIT (CD117) positive and DOG1 positive (Figures 3 and 4). Subsequent PET scans did not reveal metastatic disease. Oncology was consulted and adjuvant treatment was not recommended. The patient recovered with no postoperative complications, and was closely followed as an outpatient. She remained asymptomatic and disease-free at one year follow-up.

Discussion
Despite the overall rarity of GIST, they are still considered the most common mesenchymal tumors occurring in the GI tract. Small bowel GISTs may present evidence of GI bleeding. Tumor markers (CEA, CA-19) are not helpful in diagnosing GIST. The CT of abdomen/pelvis is the imaging modality of choice for GISTs [9]. This imaging is useful for tumor staging, obtaining a tissue diagnosis via CT guided biopsy, and postoperative patient surveillance. On CT, jejunal GISTs often appear as large, smooth walled, enhanced masses whose brightness is aided by tumor necrosis and bleeding [9]. However, CT detection rate is relatively low in tumors smaller than 3.5 cm and with intraluminal growth [10,11]. MRI and PET scans are also utilized but are not significantly better at diagnosing small tumors [9]. In this study, although the patient had a small tumor, the CT enhancement was aided by intermittent GI bleeding. Previous studies investigated the use of interventional Digital Subtraction Angiography (DSA) for locating, diagnosing small bowel GISTs in patients with GI bleeding [7]. Other diagnostic procedures such as upper endoscopy with Endoscopic Ultrasound (EUS) and wireless capsule endoscopy can also be useful [12]. With active bleeding, laparotomy with push enteroscopy with the colonoscope is also a diagnostic option.
Tumor size and mitotic rate play a crucial role in determining the malignancy of the tumor. Complete resection with negative margins is the mainstay treatment for localized GISTs [13]. Preoperative diagnosis is recommended to rule out non-GIST subepithelial tumors in the GI tract when appropriate. Our patient did not undergo a biopsy due to an increased risk of perforation considering the relatively small tumor size of 3.7 cm and difficulty accessing the lesion with endoscopy. According to the NIH modified scale, our patient would be in the low risk category due to tumor size in 2.1-5 cm range, mitotic count < 5/50 in any site along GI tract [5]. GISTs rarely metastasize to regional lymph nodes [14]. Recurrences are unlikely in small bowel GISTs < 5 cm in size, and low mortality has been linked in GISTs with low mitotic rates.
The diagnosis of GISTs is confirmed with histoimmunochemistry. Histologically, GISTs present as spindle cell type (70%), epithelioid cell type (20%), or mixed cell type (10%) [15]. Histopathological hallmark of GISTs is the presence of either receptor tyrosine kinase KIT (CD117) or Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) markers. Nearly 95% of GISTs are positive for KIT, and those negative for KIT are usually positive for PDGFRA [5]. Imatinib, a tyrosine kinase inhibitor, is used as neoadjuvant and adjuvant therapy. Neoadjuvant therapy is utilized to reduce tumor burden especially in large, locally advanced tumors. Adjuvant therapy is used postoperatively if a high risk of recurrence is suspected [5]. This patient was not a candidate for imatinib therapy due to low mitotic rate, small tumor size, and a negative PET-CT scan.
Conclusion
Occult small bowel bleeding sites can be a challenge to both localize and identify the etiology. Although jejunal GISTs are rare, they should be considered in the differential diagnosis of small bowel bleeding to aid early detection. Our case highlights those difficulties in diagnosis, especially in a patient with a small tumor. Early diagnosis benefited our patient as most GISTs are identified much later when they are large and more difficult to treat. Enhancement on CT imaging usually suggests the diagnosis. Gene mutations leading to GISTs involve c-KIT and PDGFRA, and these mutations are targets for antineoplastic therapy. Surgical resection is recommended. GISTs are notorious for recurrences, therefore close surveillance is important.
References
- Menge F, Jakob J, Kasper B, Smakic A, Gaiser T, et al. Clinical Presentation of Gastrointestinal Stromal Tumors. Visc Med. 2018; 34: 335-340.
- Soreide K, Sandvik OM, Soreide JA, et al. Global epidemiology of Gastrointestinal Stromal Tumours (GIST): A systematic review of population-based cohort studies. Cancer Epidemiol. 2016; 40: 39-46. 10.1016/j.canep.2015.10.031
- Al-Shboul OA. The importance of interstitial cells of cajal in the gastrointestinal tract. Saudi J Gastroenterol. 2013; 19: 3-15. 10.4103/1319-3767.105909
- Miettinen M, Lasota J. Gastrointestinal stromal tumors: Review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med. 2006; 130: 1466-1478.
- Miettinen M, Lasota J. Gastrointestinal stromal tumors: Review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med. 2006; 130: 1466-1478.
- Parab TM, DeRogatis MJ, Boaz AM, Grasso SA, Issack PS, et al. Gastrointestinal stromal tumors: A comprehensive review. J Gastrointest Oncol. 2019; 10: 144-154.
- Scherubl H, Faiss S, Knoefel WT, et al. Management of early asymptomatic gastrointestinal stromal tumors of the stomach. World J Gastrointest Endosc. 2014; 6: 266-71. 10.4253/wjge.v6.i7.266
- Chen YT, Sun HL, Luo JH, Ni JY, Chen D, et al. Interventional digital subtraction angiography for small bowel gastrointestinal stromal tumors with bleeding. World J Gastroenterol. 2014; 20: 17955–17961.
- Gasparotto D, Rossi S, Bearzi I, et al. Multiple primary sporadic gastrointestinal stromal tumors in the adult: An underestimated entity. Clin Cancer Res. 2008; 14: 5715.
- Tateishi U, Hasegawa T, Satake M, Moriyama N, et al. Gastrointestinal stromal tumor. Correlation of computed tomography findings with tumor grade and mortality. J Comput Assist Tomogr. 2003; 27: 792.
- Rondonotti E, Pennazio M, Toth E, Menchen P, Riccioni ME, et al. Small-bowel neoplasms in patients undergoing video capsule endoscopy: A multicenter European study. Endoscopy. 2008; 40: 488–495.
- Cheung DY, Lee IS, Chang DK, Kim JO, Cheon JH, et al. Capsule endoscopy in small bowel tumors: a multicenter Korean study. J Gastroenterol Hepatol. 2010; 25: 1079–1086.
- Akahoshi K, Sumida Y, Matsui N, Oya M, Akinaga R, et al. Preoperative diagnosis of gastrointestinal stromal tumor by endoscopic ultrasound-guided fine needle aspiration. World J Gastroenterol. 2007; 13: 2077-2082.
- Lee SY, Goh BK, Sadot E, et al. Surgical Strategy and Outcomes in Duodenal Gastrointestinal Stromal Tumor. Ann Surg Oncol. 2017; 24: 202.
- Giuliano K, Nagarajan N, Canner J, et al. Gastric and small intestine gastrointestinal stromal tumors: Do outcomes differ? J Surg Oncol. 2017; 115: 351.
- Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Int J Surg Pathol. 2002; 10: 81.