
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A reappearance of a deadly zoonotic disease in children, in Romania
Gheorghiţă Jugulete1,2*†; Alexandra Bastian3†; Sabina Andrada Zurac3†; Carmen Pavelescu2†; Monica Luminița Luminos1,2; Mădălina-Maria Merișescu1,2
1“Matei Balş” National Institute for Infectious Diseases, No. 1, Calistrat Grozovici Street, 2nd District, 021105 Bucharest, Romania.
2Faculty of Medicine, University of Medicine and Pharmacy, “Carol Davila”, No. 37, Dionisie Lupu Street, 2nd District, 020021 Bucharest, Romania.
3Department of Pathology, “Colentina” Clinical Hospital, Bucharest, Romania; Department of Pathology,“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania.
†All authors contributed equally to this work.
*Corresponding Author : Gheorghiţa Jugulete
“Matei Balş” National Institute for Infectious Diseases, No. 1, Calistrat Grozovici Street, 2nd District, 021105 Bucharest, Romania.
Email: gheorghita.jugulete@umfcd.ro
Received : Apr 15, 2023
Accepted : May 10, 2023
Published : May 17, 2023
Archived : www.jcimcr.org
Copyright : © Jugulete G (2023).
Abstract
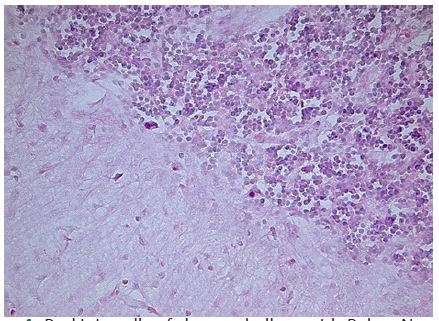
Rabies is a life-threatening and vaccine-preventable infectious disease and is triggered by an RNA virus, part of the Rhabdoviridae family, Lyssavirus genus. The rabies virus primarily spreads by saliva and is most frequently contracted through animal bites. It infects mammals, including humans, and generally causes fatal outcomes. Despite the systematic implementation program to eradicate rabies in Romania, the disease is still present as we notify a confirmed deadly case in children in 2022, after the last case in human was declared in 2012. Postexposure Prophylaxis (PEP) is standard and lifesaving if given early after exposure. We report the case of a ten-year-old female child, who was brought to the Paediatric Intensive Care Unit of the National Institute for Infectious Diseases„ Prof. Dr Matei Bals”, Bucharest, Romania with 10 days delay after being bitten by a domestic cat. We report the present patient, who was diagnosed antemortem by identifying the rabies virus in the cerebrospinal fluid based on Reverse Transcription-Polymerase Chain Reaction (RT-PCR) and post-mortem by a histopathological examination (which reveals the presence of Babes-Negri bodies in the hippocampus) and managed according to the Milwaukee Protocol. We want to highlight the importance of educating the public about the dangers of unvaccinated domestic animals, especially for cats and to limit human-animal rabies exposures. Due to management mistakes, child victims continue to surface, necessitating a public ongoing education campaign about the risks associated with unvaccinated pets.
Keywords: Rabies; Children; Postexposure prophylaxis; Zoonotic disease; Vaccine.
Citation: Jugulete G, Bastian A, Zurac SA, Pavelescu C, Luminos ML, et al. A reappearance of a deadly zoonotic disease in children, in Romania. J Clin Images Med Case Rep. 2023; 4(5): 2418.
Introduction
Rabies is a zoonotic disease determined by a single-stranded RNA virus, which belongs to the Lyssavirus genus, Order Mononegavirales, Rhabdoviridae family, that kills every year approximately 59000 people worldwide [1]. Rabies virus has various variations, and these variants are frequently found types of animals or in particular regions. Rabies infection is transmitted by exposure to saliva from a rabid animal, after animal bite, and the incubation period is variable. Among infectious diseases, rabies encephalitis has the greatest mortality rate. The neuronal mechanism which mediates rabies encephalitis to death is still unclear [1-4]. Postexposure Prophylaxis (PEP) is necessary to be started as early as possible and this estimates to prevent hundreds of thousands of rabies deaths annually [5]. Wound cleansing management and simultaneous administration of Rabies Immunoglobulin (RIG) combined with the Anti-Rabies Vaccine (ARV) is almost invariably effective even after high-risk exposure and should be started as early as possible after a contaminated event [6]. Fatal failures of PEP, when occur, are typically associated with insufficient or delayed PEP treatment. Nevertheless, insufficient therapy may result in delayed or suboptimal RIG administration, as well as inadequate injection of wounds which is constrained in pediatric patients by low body weight. If the body-weight-based RIG dose’s volume turns out to be insufficient, volume expansion through dilution will be required to achieve complete virus neutralization and adequate infiltration into all wounds. The profound coma while the patient is kept, the so-called “Milwaukee protocol”, uses anti-excitotoxic and antiviral measures. The fundamental tenet of this approach is that if the patient is supported through the strong excitotoxic phase, the natural host immune response will be able to eliminate the rabies virus [7,8].
Between 2012 and 2022, cases of rabies in human have been reported in countries like Belarus, Romania, Russia, Switzerland and Turkey, and the disease is still endemic in several Eastern European countries (eastern Poland, Romania, Ukraine, Belarus, and Russia, [9] (Table 1). See Rabies dynamics for 2022, Europe. All European countries with zero rabies were excluded from the list [9,10].
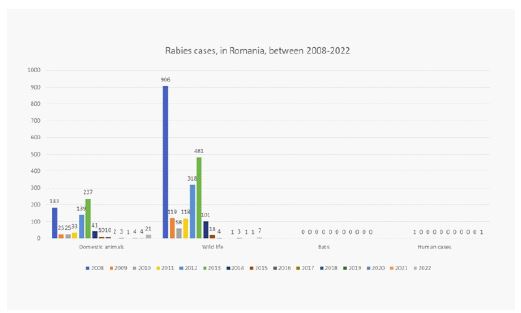
More than 95% of human rabies cases in rabies-endemic areas are caused by dog bites, with a tiny minority caused by transmission via wild animals, like foxes, bats, jackals, racoons, skunks, and wolves [9]. Romania has been regarded as one of Europe`s rabies affected nations until 2011, when the national strategic program focusing on rabies control has been implemented through oral vaccination campaigns of pets and wild animals twice a year, and throughout the nation since 2015. This tactic campaign resulted in a marked decline in the number of positive cases of rabies discovered in both domestic and wild animals [9,10]. In 2010 before the vaccination program, Romania reported 135 rabies cases in domestic animals. 2012 saw the final human instance of rabies, in Bacau County. 27 January 2021 saw the final wildlife cases in Satu Mare county, Gherta Mica locality. 1 dog case and 1 cow case in early July 2020, both near Moldova and the last year of occurrence of rabies in domestic animals was on the 5th of November 2021, Iasi County [9-11]. There haven’t been many autochthonous instances of rabies in humans in many European Union member states in recent years. The required vaccination of pets is a crucial element of the rabies control policy in Romania, in addition to oral vaccine programs [12]. Due to rabies control program in our country, the human rabies positive cases decreased, and between 2012 until 2022 Romania declared zero rabies, until the female child was diagnosed and reported (Figure 1).
Table 1: Rabies dynamics for 2022, Europe. All European countries with zero rabies were excluded from the list [9,10].
| Country | Domestic Animals | Wild Life | Bat | Human cases | Total |
|---|---|---|---|---|---|
| Total | 322 | 196 | 11 | 2 | 531 |
| France | 1 | 0 | 0 | 0 | 1 |
| Georgia | 30 | 1 | 0 | 1 | 32 |
| Germany | 0 | 0 | 6 | 0 | 6 |
| Hungary | 1 | 3 | 0 | 0 | 4 |
| Poland | 3 | 33 | 3 | 0 | 39 |
| Romania | 21 | 7 | 0 | 1 | 29 |
| Slovak Republic | 1 | 0 | 0 | 0 | 1 |
| Spain | 7 | 0 | 0 | 0 | 7 |
| Switzerland | 0 | 0 | 1 | 0 | 1 |
| Netherlands | 0 | 0 | 1 | 0 | 1 |
| Ukraine | 258 | 152 | 0 | 0 | 410 |
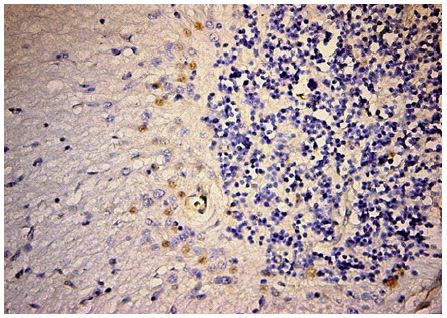
The rabies virus is transmitted from sick animals when infected saliva contact with open wounds such as those caused by bites or scratches, and when it meets the surfaces of the human mucosa [1,4,12]. The rabies virus usually penetrates the body through the wound produced by the bite of an infected animal (its saliva containing the virus) and by way of fillets, reaches the brain, triggering characteristic lesions. Literature accounted for some cases of rabies transmitted through aerosols or mucous membranes (accidentally in laboratories) [13-16]. The more the area where the bite is located is innervated (fingers, genital area) or closer to the brain (face) the shorter the time of incubation. From the clinical standpoint, there are two forms of rabies: furious and paralytic, both preceded by a prodrome with a characteristic clinical picture. The most frequently described cases are furious clinical forms with more rapid evolution towards death [17]. The rabies virus can be isolated by in situ hybridization methods (RT-PCR- polymerase chain reaction) that can identify the virus at the level of the wound, the saliva or the central nervous system. Postmodern diagnosis of rabies is established by anatomopathological examination which high lights, by immunohistochemistry techniques, the presence of Babes-Negri bodies, pathognomonic for rabies. Electronic microscopy can also evince the rabies virus in the hippocampus as well as in other tissues. Rabies treatment is only prophylactic (immunoglobulins and vaccination), with other methods (prolonged sedation, decrease in the body temperature) having recorded meaningful results, so far. Once obvious clinical signs have occurred rabies evolves severely, leading to death [18-21].
By 2030, the EU wanted to completely eliminates rabies in human, from both domestic and wild animals. The disease is still present in European countries, and Romania notify the new case of human rabies despite of how reachable the objective appeared to be. We want to report this new case in a child, as our data show that there is a need for education in population regarding pet’s vaccinations programs, improving access to PEP, to not tolerate fatalities from rabies in the future.
Case report
Between 2008-2022, Romania, declared 7 cases of human rabies, 57.14% in children, 71.43% were female. In 3 cases, the animal involved was domestic cat. Children are at high risk due to their inability to defend themselves from infected animals and most deaths occur with a particularly high incidence in this category (under the age of 15 years) [22].
We report the case of a ten-year-old female patient, admitted to the Paediatric Intensive Care Unit at National Institute for Infectious Diseases, Prof. Dr Matei Bals”, Bucharest with clinical rabies developed 10 days after she was bitten at the level of the hand by a domestic cat. No medical attention was sought, and no rabies post exposure prophylaxis was administered. The cat was known to the family, didn’t receive anti-rabies vaccination, and had aggressive behavior which raised the suspicion of animal rabies at hospitalization. The parents were counselled about her diagnosis and prognosis.
Upon admission, the patient presented a critically altered general state, with severe psychomotor agitation that alternated with rare periods of consciousness, visual and auditory hallucinations, significant hypersomnia, aerophobia and hydrophobia, tachycardia (VA- 170 b/min), polypnea (40-50/min), SpO2 - 95% in atmospheric air without signs of meningeal irritation. The onset of symptomology was 24 hours before hospitalization. On the first hospital day, the patient was afebrile (temperature, 36.4°C). Biological samples taken at the time of admission didn’t record significant changes, except for increased LDH (Lactate dehydrogenase) and muscle enzymes (CK) and hepatic cytolysis increased in day 18, as well as persistent elevated BUN (blood urea nitrogen) and creatinine levels. Inflammatory markers increased in day 5, with left shift WBC, increased CRP and high platelets. IgM serology for viral illnesses was negative, except for this aetiology. We also appealed to differential diagnosis, outlining all the diseases with a similar clinical picture (acute meningoencephalitis, acute encephalopathy, coma of various causes, acute intoxication).
On the first day of hospitalization, a lumbar puncture was performed, whose result was within normal ranges, while PCR taken from Cerebral Spinal Fluid (CSF) identified the rabies virus by a method which is used both in human and in veterinary medicine. This method was the patenting of the method diagnosis of postmortem human rabies, published in RABIES BULLETIN EUROPE, GenBank Bank It Submission ID:1976388 [11].
Based on the clinical signs, epidemiological data, and the identification of the rabies virus in CSF the diagnosis of rabies encephalitis-furious form- was established. Specific rabies immunoglobulin therapy, of equine origin, was initiated, with sensitivity testing and progressive desensitization, followed by anti-rabies vaccination (therapeutic scheme applied on days: 0, 3, 7, 14, 28) without any records of allergic incidents. Furthermore, until the rabies diagnostic was confirmed, we also introduced acyclovir treatment. Therapy was supplemented with anti-oedema drugs (Mannitol and Furosemide), anti-inflammatory steroids (Dexamethasone), unspecified human immunoglobulin, acid-base andhydro electrolytic rebalancing, and symptomatic drugs.

Evolution was rapidly unfavorable, see Figure 2, with the onset of an acute cardio-respiratory failure that required the induction of coma (the “Milwaukee protocol” was used, however without success) and orotracheal intubation with mechanical ventilation, in less than 24 hours from admission. Also, to preserve the brain functions we induced hypothermia by decreasing the body temperature to 34oC, however without any positive outcomes. Oxygen delivery was optimized to maintain the hemoglobin level at more than 10 g per deciliter, and mechanical ventilation targeted arterial normoxia.
Biochemical evidence of hemolysis and acidosis was detected by the seventh hospital day. The hemoglobin level declined from 12.7 to 10.5 g per deciliter, whereas the lactate dehydrogenase level rose from 400 to 1220 U per liter over seven days. Increased levels of liver aminotransferase (82 IU per liter), and computed tomography of her head were normal. Despite the complex treatment, evolution was unfavorable with the onset of Multiple Organ Dysfunction Syndrome (MODS) (kidney, liver, hematologic, neurologic) and mechanical ventilation-associated bronchopneumonia, the patient presented a clinical picture of brain death, was extubated, and died 30 days after admission.
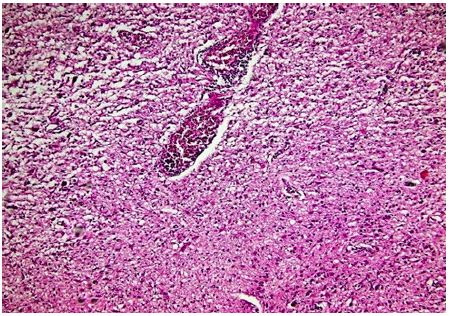
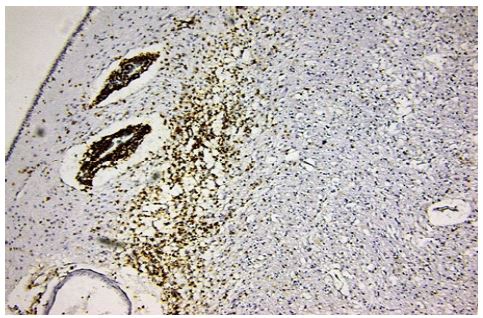
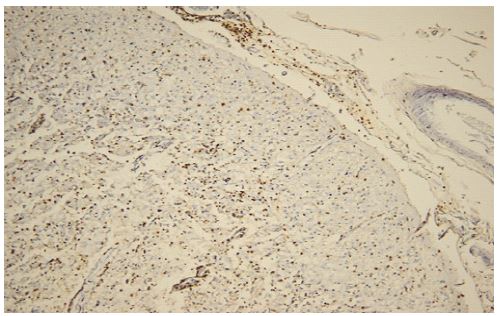
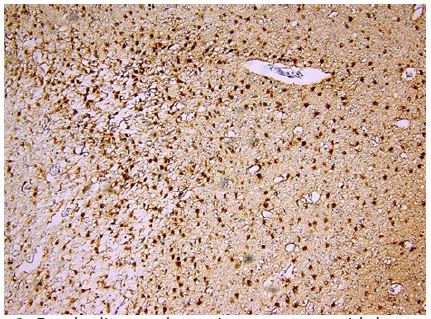
Subsequently, the anatomopathological examination confirmed the established diagnosis. All brain samples were positive for rabies virus, and the principal findings on autopsy revealed subacute encephalomyelitis with numerous Negri bodies found principally in the cerebellum, hippocampus, thalamus, brain stem, and on the dorsal root ganglia of the spinal cord. (Figures 3 - 12).




Discussion
Although rabies may be prevented, it remains a serious public health concern both internationally and domestically since it is a lethal illness once it manifests. The high risk of mortality and the fact that it can be prevented by vaccination and protection, emphasize the importance of prophylaxis following exposure to rabies risk. Through the present material, we outlined a case of pediatric rabies, the clinical furious form, having as the source of infection a domestic animal (rabid cat - without diagnostic confirmation) who, initially, didn’t receive specific prophylaxis (only 10 days after the infecting bite, in our clinic). The clinical course of human rabies starts with the length of the incubation period which depends on the location and severity of the bite, the amount of inoculated virus and the patient’s age. The next clinical stage is the prodromal period when the patient develops the early symptoms of rabies. At this stage, the diagnosis remains difficult. The neurological phase is the third stage, and the virus reaches the brain stem. We are facing two clinical forms of rabies, when most patients develop the encephalitic or furious form with classical symptoms such as hypersalivation, hydrophobia, aerophobia, pharyngeal spasms, muscle spasms, rigidity, seizure, hydrophobia, aerophobia, pharyngeal spasms, hypersalivation, most of which occurred in our patient, and are described in the literature. The other clinical form is the paralytic one, which is more difficult to diagnose and less frequent than the furious form. In both cases, the death march almost usually ensues. However, intravital diagnosis is often difficult to make while negative results or atypical symptoms should not rule out the diagnosis of rabies. Early administration (within the first hours from the infectious bite) of passive prophylaxis (anti-rabies immunoglobulin) followed by anti-rabies vaccination would have led to a better outcome in terms of evolution and prognostic. From the standpoint of positive diagnostic, this was established based on clinical and epidemiological data, and unfortunately with histopathology confirmation (postmortem). Likewise, the diagnostic was confirmed antemortem by identifying the rabies virus in CSF by PCR, a diagnostic method due to being patented in humans (currently it is only being used in animals, in our country). In our clinic we have also used this method of diagnosis in a child with rabies, a case presented and published in the journal, Rabies Bulletin Europe” [11]. This method is useful because it helps clinicians establish an early diagnosis of rabies, with the introduction of specific treatment which ultimately would trigger a better prognostic for this affection. Evolution was unfavorable, despite the complex treatment (anti-rabies, pathogenic, symptomatic drugs, induced coma with intubation and mechanical ventilation, hypothermia), the patient dying due to Multiple Organ Dysfunction Syndrome (MODS) and complications associated with prolonged mechanical ventilation (30 days). The particularity of this case highlights the need for an early diagnosis and warns parents to come to the hospital as soon as a bite occurs, regardless of the type of animal that was involved. The greater the distance from the aggressive contact to the presentation to the doctor, the lower the survival [23].
Romania appears to be the country with the highest number of cases of human rabies in the European Union, with endemic transmission. Six instances of human rabies were documented between 2008 and 2012, in Romania, with two of them happening in the district of Bacău. Four girls and two males represented half of the cases, while adults formed up the other half. Three of the incidents featured domestic cats, two involved animals from the wild, and one involved a stray dog biting the victims. Many bites occurred on the hands and legs, however one patient claimed to have been bit in the face, and another patient had a neck bit. The attempts to replicate the “Milwaukee protocol,” in contrast to the affected individual, have typically been ineffective [24,25]. This has been shown to occur in both domestic and wild animal bite cases of rabies in the past. Long-term survival in rabies patients who followed the protocol is probably due more to excellent intensive care and supportive care than to the protocol itself. There isn’t a readily implementable palliative care protocol for rabies patients that could be used, despite numerous attempts to treat rabies encephalitis.
Even if Romania is declared a rabies-free country, and no human case was reported since 2012 until our case report, there is a risk that once an aggressive event occurs, it could lead to the confirmation of a fatal rabies diagnosis because Romania has a significant number of domestic animals with rabies. It appears that domestic animals, especially cats, are a significant source of human rabies transmission in our country. Therefore, vaccination following cat attacks should be considered. Specific actions are urgently required to raise public consciousness of the issue.
Conclusion
Rabies is an extremely severe disease that causes death in almost all cases once the neurological clinical picture is installed. In our case report, the “Milwaukee protocol” for the therapy of rabies has not been successfully replicated, as adequately describe. In Romania PEP is free of charge and is included in the national rabies control program. Vaccination after animal bites should be done immediately unless the animal can be proven negative for rabies within 48 h after contact, and this could maintain the rabid-free program in Romania.
Declarations
Author contributions All authors have the same contribution.
Funding This research received no external funding.
Institutional review board statement: all procedures and experimental protocols comply with the European Communities Council Directive of 24 November 1986 (86/609/EEC).
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data availability statement: The data that support the findings of this study are available on request to the corresponding author.
References
- Amarasinghe GK, Bào Y, Basler CF, et al. Taxonomy of the order Mononegavirales: Update 2017. Archiv Virol. 2017; 162: 2493-2504
- WHO. Fact-sheet rabies. Available: https://www.who.int/news-room/fact-sheets/detail/rabies [Accessed 11 Nov 2022].
- Walker PJ, Blasdell KR, Calisher CH, Dietzgen RG, Kondo H, et al. ICTV Report Consortium. ICTV Virus Taxonomy Profile: Rhabdoviridae. J Gen Virol. 2018; 99: 447-448.
- Scott TP, Nel LH. Lyssaviruses and the Fatal Encephalitic Disease Rabies. Front Immunol. 2021; 12: 786953.
- WHO. WHO Guide for Rabies Pre- and Post-exposure Prophylaxis în Humans. World Health Organization. Available at http://www.who.int/rabies/ PEP_prophylaxis_guidelines_June10.pdf. Accessed: October 18, 2022
- Hemachudha T, Ugolini G, Wacharapluesadee S, Sungkarat W, Shuangshoti S, et al. Human rabies: Neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013; 12: 498-513.
- Willoughby RE Jr, Tieves KS, Hoffman GM, Ghanayem NS, Amlie-Lefond CM, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005; 352: 2508-2514.
- Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014; 384: 1389-1399.
- https://rr-europe.woah.org/wp-content/uploads/2022/03/sge_rab3_romania.pdf
- World Health Organization. Rabies vaccines: WHO position paper. Wkly. Epidemiol. Rec. 2018; 93: 201–220.
- Luminos M, Barboi G, Streinu Cercel A, Staniceanu F, Jugulete Gh, Visan A, et al. Rabies Buletine Europe,“Human Rabies in a Romanian boy – an ante mortem case study”. 2011; 35: 5–8. (www.who-rabies-bulletin.org)
- Jakel V, König M, Cussler K, Hanschmann K, Thiel HJ, et al. Factors influencing the antibody response to vaccination against rabies. Dev Biol (Basel). 2008; 131: 431–437.
- Warrell MJ. The dilemma of managing human rabies encephalitis. Trop Med Int Health. 2016; 21: 456-457.
- Pieracci EG, Pearson CM, Wallace RM, Blanton JD, Whitehouse ER, et al. Vital signs: trends in human rabies deaths and exposures - United States. MMWR Morb Mortal Wkly Rep. 2019; 68: 524–528.
- Mahadevan A, Suja MS, Mani RS, Shankar SK. Perspectives in diagnosis and treatment of rabies viral encephalitis: insights from pathogenesis. Neurotherapeutics. 2016; 13: 477–492.
- Vişan A, Luminos M, Vasile M, et al. Viral encephalitis caused by respiratory viruses. BMC Infect Dis. 2013; 13: P78. https://doi.org/10.1186/1471-2334-13-S1-P78
- Mallewa, M. et al. Rabies encephalitis in malaria-endemic area, Malawi, Africa. Emerg. Infect. Dis. 2007; 13: 136–139. This is a case study report from Malawi showing that rabies is regularly misdiagnosed if a clinical diagnosis is undertaken without laboratory confirmation of rabies.
- Jugulete G, Bastian AE, Zurac SA, Merisescu MM, Luminos ML, et al. Rabies encephalomyelitis in children-paralytic form.Case report. Rom J Leg Med. 2020; 28: 218-222.
- Chacko K, Parakadavathu RT, Al Maslamani M, Nair AP, Chekura AP, Madhavan I. Diagnostic difficulties in human rabies: A case report and review of the literature. Qatar Med J. 2016; 2: 15.
- Wadhwa A, Wilkins K, Gao J, et al. A Pan-Lyssavirus Taqman real-time RT-PCR assay for the detection of highly variable rabies virus and other lyssaviruses. PLoS Negl Trop Dis. 2017; 11: e0005258.
- Prosniak M, Faber M, Hanlon CA, Rupprecht CE, Hooper DC, Dietzschold B, et al. Development of a cocktail of recombinant-expressed human rabies virus-neutralizing monoclonal antibodies for postexposure prophylaxis of rabies. J Infect Dis. 2003; 188: 53-56.
- Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, et al. Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015; 9: e0003709.
- Zeiler FA, Jackson AC. Critical Appraisal of the Milwaukee Protocol for Rabies: This Failed Approach Should Be Abandoned. Can J Neurol Sci. 2016; 43: 44-51.
- Manesh A, Mani RS, Pichamuthu K, Jagannati M, Mathew V, et al. Case Report: Failure of Therapeutic Coma in Rabies Encephalitis. Am J Trop Med Hyg. 2018; 98: 207-210.
- Tinsa F, Borgi A, Jahouat I, Boussetta K. Rabies encephalitis in a child: A failure of rabies post exposure prophylaxis? BMJ Case Rep. 2015; 2015: bcr2014206191.