
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Assessment of rotational mechanics by 2D – speckle
tracking in heart transplant patients: A comparison
study with endocardial biopsy
Azin Alizadehasl1; Ahmad Amin2; Anita Sadeghpour3; Sepideh Taghavi2; Leila Nojoomizadeh2*; Kambiz Mozaffari4; Leila Jamshidi5
1Professor of Cardiology, Echocardiologist, Head of Cardio-Oncology Department and Research Center, Rajaie Cardiovascular, Medical and Research Center, Iran University of Medical Science, Tehran, Iran.
2Rajaie Cardiovascular, Medical and Research Center, Iran University of Medical Science, Tehran, Iran.
3Professor of Cardiology, Echocardiography Research Center, Rajaie Cardiovascular, Medical and Research Center, Iran University of Medical Science, Tehran, Iran.
4Associate Professor of Pathology, Rajaie Cardiovascular, Medical and Research Center, Iran University of Medical Science, Tehran, Iran.
5Department of Community & Preventive Medicine, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Leila Nojoomizadeh
Echocardiography Research Center, Rajaie Cardiovascular Medical & Research Center, Iran University Medical Science, Tehran, Iran.
Tel: +98 (21)23921;
Email: l.nojoomizadeh@gmail.com
Received : Apr 15, 2023
Accepted : May 11, 2023
Published : May 18, 2023
Archived : www.jcimcr.org
Copyright : © Nojoomizadeh L (2023).
Abstract
Background: Up to now, Endomyocardial Biopsy (EMB) is the gold standard for monitoring acute rejection in Heart Transplant (HTx) recipients. This study aims to investigate using the Left Ventricle (LV) deformity index derived from 2-Dimensional Speckle Tracking Echocardiography (2D-STE) for allograft rejection monitoring.
Methods: For a total of 30 EMBs performed in 19 HTx recipients, 2D-STE was done within 24 hours before or after each biopsy. The LV- torsional deformity indexes, including LV-twist, LV- rotation, and LV-torsion, were derived. These values were compared in HTx recipients, who were subsequently classified into either the ‘no rejection group’ or the ‘rejection group.’ The rejection group was then further sub-classified based on the grade of rejection.
Results: Among 30 EMBs, 12 biopsies showed no rejection, 15 displayed mild rejection, and 3 showed mild to moderate or moderate rejection. Mean twist and torsion values decreased more in the rejection group than in the no-rejection group (P=0.004, P=0.005, respectively). In LV-twist measurement, a cut-off point of 7.8 degrees had a sensitivity of 83% and a specificity of 67% in detecting the allograft rejection.
Conclusion: The LV–torsion values derived from 2D-STE could be a reliable, non-invasive, and valuable tool for screening rejection in HTx recipients.
Keywords: Speckle–tracking echocardiography; Left ventricular mechanics; Torsion; Twist; Heart transplantation; Cardiac allograft rejection diagnosis.
Citation: Alizadehasl A, Amin A, Sadeghpour A, Taghavi S, Nojoomizadeh L, et al. Assessment of rotational mechanics by 2D – speckle tracking in heart transplant patients: A comparison study with endocardial biopsy. J Clin Images Med Case Rep. 2023; 4(5): 2420.
Introduction
Heart transplant is the therapy of choice for patients with end-stage heart failure who remain refractory to medical treatment. Survival and quality of life after cardiac transplantation is excellent [1,2]. Data from the International Society for Heart and Lung Transplantation (ISHLT) indicates that the average annual rate of heart transplants has increased recently, reaching over 5500 heart transplants in 2016 worldwide [3].
Acute rejection is a frequent complication, particularly in the first year after transplantation. Among heart transplant recipients, most such cases are acute cellular-mediated rejections [4]. Improvement in immunosuppression therapy and also early diagnosis and treatment of allograft rejection have resulted in reduced mortality rates due to rejection [5]. Up to now, Endomyocardial Biopsy (EMB) is the gold standard for diagnosis of rejections [6,7]. This invasive method has several complications in 0.09% to 5.2% of cases, including myocardial perforation, tricuspid regurgitation, arrhythmia, etc [8].
Compared with EMB, there are some non-invasive alternatives for detection of rejection, such as Cardiac Magnetic Resonance Imaging (MRI), echocardiography, cardiac troponin level, etc., which have previously been used by specialists; however, none of them has replaced the pathologic finding derived from biopsy, since their reliability has not been established yet [6,9]. 2D-STE is an echocardiography modality for assessing myocardial function, providing the early subclinical diagnosis of ventricular dysfunction [8,10]. Previous studies using 2D-STE-derived myocardial deformity indexes have indicated that LV global longitudinal and circumferential strain, torsion, and twist may be helpful in the early detection of acute allograft rejection. The results are equivocal, and further evaluation is needed [8,10-12].
The Left Ventricle (LV) torsional parameters are sensitive indices for evaluating both systolic and diastolic function [13-16].
In definition, LV rotation is referred to as a wringing motion of the LV cavity away from its long axis. The apex and base of LV have counter-directional rotation. During systolic contraction, the base rotates clockwise (expressed with a negative value), and the apex rotates counter clockwise (expressed with a positive value) when viewed from the apex. The mode of contraction is related to the oblique and opposite directions of fibers in the subepicardium (left-handed direction) and subendocardium (right-handed direction). The orientation of apex and base rotation follows the fibers in the subepicardium, indicating that the subepicardium side is predominant as its radius is more than that of the subendocardium [13,14,17-20].
The LV twist, which is defined as the absolute difference in the rotational angle between base and apex, is expressed in degrees; LV torsion is referred to as this gradient along the longitudinal axis of the LV, expressed in degrees per centimeter [17,20,21].
In 1987, Hansen et al. investigated acute rejection, confirmed by EMB, in heart transplant recipients and documented an association between acute rejection and decreased LV torsion deformity, measured by intramyocardial markers [22]. A limited study has applied MRI to survey twist and torsion in pediatric transplanted hearts [23]. Two recent articles, one on monitoring acute rejections [6] and the other on clinically stable HTx recipients [24], have been published on the utility of torsion deformities derived from echocardiography.
To date, however, it seems that the data available are insufficient to justify echocardiography as a reliable diagnostic modality replacement for EMB to monitor acute rejection in heart transplant recipients. This study investigates the utility of the LV-deformity index derived from 2D-STE for screening heart transplant rejection. Likewise, we aim to determine a cut-off point for the LV deformity index, which can be used for predicting rejection in HTx recipients.
We, therefore, assessed the efficiency of LV torsion deformities obtained from 2D Speckle Tracking Echocardiography (2D-STE) for monitoring acute rejection in heart transplant recipients.
Methods
Study population
A total of thirty EMBs were performed in nineteen heart transplant recipients (18 men, one woman), transplanted at 25.8 ± 6.7 years of age, between Dec 2015 and Jun 2016. All heart transplant recipients had received standard immunosuppressive therapy, and as the routine protocol, heart catheterization was done to monitor the rejection. All the subjects provided written informed consent for participating in the study. Diagnosis of acute cellular rejection was based on the definition provided by the International Society for Heart and Lung Transplantation (ISHLT).
Echocardiography
For each case, an echocardiographic examination, including conventional and 2D-STE, was done less than 24 hours either before or after the biopsy, using a Philips EPIQ cardiology ultrasound machine with an X5-1 Transducer. The LV Ejection Fraction (EF) was measured by the Simpsons method, derived from both the apical 4- and apical 2-chamber views. Diastolic function was obtained via mitral inflow pulsed-wave Doppler and also tissue Doppler imaging. Furthermore, the structure and function of cardiac valves were evaluated. Interventricular Septum (IVS) thickness was also measured using 2D echocardiography. Data sets, including short-axis and apical views, were acquired for three consecutive heart cycles in a stable heart rate period. For minimizing respiration-related variations in HR, the end-expiration breath-holding acquisition setting was selected. Heart rate variation < 2-3 beats/minute was acceptable during the acquisition time. Exact supervision was performed to record imaging in an HR maintained stable through the examination period. This HR stability is also essential for adjusting time intervals (e.g., AVC) in the cardiac cycle. AVC point was representative of the end-systolic time, obtained from a 3-chamber apical view and applied to other views.
The LV short-axis views were acquired at basal, mid, and apical levels with appropriate frame rate (40-80 frames/s) to assess the LV mechanics, including LV rotation and circumferential strain. As far as possible, special attention was paid to obtaining circular cross-sectional views; the basal plane was acquired at the mitral valve level, whereas the mid and the apical plane were obtained at the papillary muscles level and just above the point of systolic cavity obliteration, respectively. The LV apical 2-, 3- and 4- chamber views were also applied to define LV-GLS, moreover; the apical 4-chamber view centered on the Right Ventricle (RV) was used to examine RV systolic function by Fractional Area Change (FAC), Tricuspid Annular Plane Systolic Excursion (TAPSE) and tissue Doppler imaging. Four sequential cardiac cycles were sequestrated and reserved for the subsequent off-line analysis using Q-lab software. Demarcation of endocardial borders was assigned in both the short axis and apical views manually. If needed, border readjustments were done by the operator.
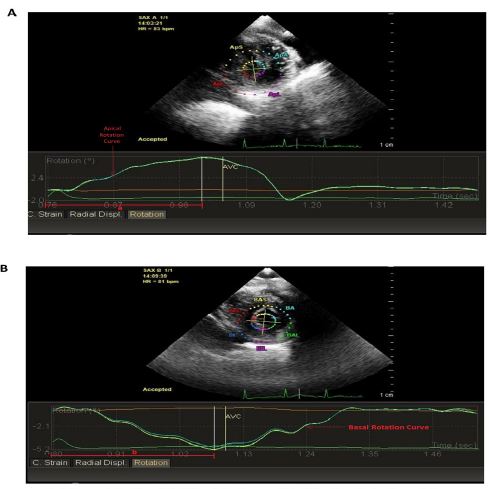
As viewed from the apex, the LV base rotated clockwise (expressed with a negative value). Reversely, the LV apex rotated counter clockwise (positive value). Two mean curves for each case were acquired, representing apical and basal end-systolic rotations (Figure 1 & Figure 2).

We also obtained the LV Global Longitudinal Strain (LV-GLS) and LV Global Circumferential Strain (LV-GCS) values through echocardiographic examination. LV GLS was calculated as the mean of peak systolic strain values, acquired from all segments in 4, 2- and 3- chamber views, whereas LV GCS was determined from the average of peak systolic strain quantities from basal, mid, and apical short-axis views, measured in all segments. By definition, the LV myocardium length changings through the base to the apex of LV and along the circumferential axis are expressed as longitudinal and circumferential strain, respectively [10,11,25-27].
Statistical analysis
Quantitative data are presented as mean ± SD, and qualitative data are evaluated as percentages. The normality of variables was assessed based on standard distribution plots and histograms. Biopsy groups were divided into three categocategories: І. No rejection; Π. Mild rejection and Ш. Mild to moderate rejection plus moderate rejection. Clinical characteristics, echocardiographic indexes, and hemodynamic variables were compared between groups by One-way Anova or Kruscalwalis analysis. Associations between quantitative variables were examined based on the Pearson or Spearman coefficient. Multiple linear regression was applied to predict the effect of confounding demographic variables on EF, such as age, with p values < 0.05 being considered significant. Finally, for analyzing all data obtained, SPSS software was applied.
Reproducibility
Intra-observer reproducibility was evaluated by repeating measurements in six random- cases about four weeks after the first analysis by the same operator on the same image sets. Inter-observer reproducibility was assessed by comparing measurements performed between first and second operators at different times in six random- cases on the same image sets. We assessed the reproducibility using Bland-Altman (BA) analysis. In this regard, variability percentages of twist deformity index were reported for Intra and inter-observer analysis with a Coefficient of Repeatability (CR) of 2.6% and 3.4%, respectively. The Intra and inter-operator absolute 95% limits of agreement (between -2.5% and + 2.6%) and (between -3.2% and +3.4%) described the validity of twist deformityin the order already mentioned.
Results
Table 1 shows the main clinical characteristics of the study. Among 30 EMB performed in this study, 12 biopsies (40%) showed no rejection, 15 (50%) showed mild rejection, and three biopsies (10%) showed mild to moderate and moderate rejection. Age was not significantly different between the groups at the time of transplant surgery.
Feasibility
In our study feasibility of obtaining 2D-STE analysis was 86%. A total of 35 individuals attended the examination. We included only subjects (n=30) in which visualization of the endocardial border and tracking quality was optimal in LV views needed for our measurements. Five individuals (14%) were excluded because of poor endocardial assessment and tracking quality.
Echocardiographic parameters
Conventional echocardiographic parameters, including the LV EF percentage, grading of diastolic dysfunction, and Right Ventricle (RV) systolic function, did not significantly differ amongst the groups. Likewise, the severity of Mitral Regurgitation (MR) and Tricuspid Regurgitation (TR), which could influence LV torsional deformities subsequently, were similar in the groups, i.e., not more than mild to moderate in severity (Table 2). The mean IVS thickness did not substantially vary in the different groups, as its value was within the normal range for all cases.
The values of mean twist and torsion, based on 2D-STE, were significantly reduced in the rejection groups in comparison with those without rejection (p=0.004, p=0.005, respectively); based on this, with each unit increase of rejection grade, the twist decreased by 1.04 units according to the linear regression formula.
At Receiver Operating Characteristic (ROC) curve, the twist showed a good predictive value to individuate rejection (AUC=0.80, p=0.006). A cut-off value of 7.8 degrees for LV twist had an 83% sensitivity and a 67% specificity to detect the rejection. There was a weaker but significant correlation between changes in rejection grades and values of torsion deformities; on the contrary, the absolute values of mean apical rotation and mean basal rotation were insignificantly correlated with rejection grades (p=0.552, p=0.548, respectively) (Table 3). Figures 1 and 2 show apical and basal rotational curves at short-axis views in patients without rejection and moderate rejection, respectively.
Moreover, both the time to peak apical and basal rotation were independently associated with rejection severity (p=0.01, p=0.004, respectively), such that more severe grades of rejection resulted in more time to peak apical and basal rotation values (Table 3).
Despite having a positive correlation between adjusted time to peak basal rotation as a percentage of R-R cycle length with rejection severity (p=0.015), there was no meaningful association between the time to peak apical rotation/R-R cycle length and grade of rejection (p=0.08). Furthermore, both the time to onset of apical and basal rotation were not associated with rejection grading (p=0.8, p=0.53, respectively) (Table 3).
Consequently, additional data was also obtained using 2D-STE. The absolute values of LV-GCS were lower in HT patients with rejection than those without rejection (p=0.001), while no significant differences were observed in LV-GLS between rejection and no rejection groups (p=0.53) (Table 3).
Alternatively, in this study, we assayed the relation between LVEF and torsional deformities. To some extent, LVEF was directly correlated with twist and torsion values (p=0.033, p=0.008, respectively). Although LVEF was not associated with basal rotation values, it directly correlated with apical rotation (p=0.3, p=0.04, respectively). In addition, there was a meaningful correlation between the absolute values of both GLS and GCS with the LV ejection fraction (p=0.001 for both) (Table 4).
Table 1: Clinical characteristics of participants.
| Parameters | No rejection | Mild rejection | Mild to moderate rejection & Moderate rejection | P-value |
|---|---|---|---|---|
| Age at transplantation (years) | 28.5 ± 7.7 | 24.3 ± 6.5 | 22.1 ± 0.28 | 0.19 |
| Age at examination (years) | 30.5 ± 7.5 | 25.6 ± 7. 8 | 23.4 ± 0.57 | 0.16 |
| Post-transplant duration (weeks) | 109 ± 20.9 | 65.6 ± 8.79 | 78.6 ± 3.22 | 0.74 |
| Male, N (%) | 11 (37.9%) | 15 (51.7%) | 3 (10.3%) | 0.46 |
| Female, N (%) | 1 (100%) | - | - | |
| Body surface area (BSA) | 1.77 ± 0.18 | 1.78 ± 0.26 | 2.13 ± 0.28 | 0.06 |
| Blood pressure (SD) | 103/78 ± 2.2 | 101/75 ± 3.1 | 98/72 ± 2.7 | 0.7 |
| Heart Rate (SD) | 89 ± 1.7 | 92 ± 3.8 | 93 ± 3.2 | 0.89 |
Table 2: Conventional echocardiographic parameters.
| Parameters | No rejection | Mild rejection | Mild to moderate & Moderate rejection | P-value |
|---|---|---|---|---|
| PAP, (mmHg) | 26.3 ± 6.05 | 29.2 ± 5.03 | 25.6 ± 6.35 | 0.33 |
| LVEF (%) | 56.2 ± 2.5 | 53.7 ± 3.2 | 56.9 ± 3.7 | 0.4 |
| MR, n (%) Mild Mild to moderate Moderate Severe |
12(100%) - - - |
15(100%) - - - |
(100%) - - - |
0.81 |
| TR, n (%) Mild Mild to moderate Moderate Severe |
9(75%) 3(25%) - - |
10(80%) 5(20%) - - |
2(61.5%) 1(38.5%) - - |
0.662 |
| Diastolic function, n (%) Normal Grade1 diastolic dysfunctionGrade2 diastolic dysfunctionGrade 3 diastolic dysfunction |
(25%) 9(75%) - - |
8(80%) 7(20%) - - |
2(46%) 1(53%) - - |
0.23 |
| RV function, n (%), assessed by TAPSE & tissue Doppler
Normal Mild RV dysfunction Mild to moderate RV dysfunction Moderate RV dysfunction Severe RV dysfunction |
- 7(58%) 5(42%) - - |
- 8(53.3%) 6(40%) 1(6.6%) - |
- 2(66.6%) 1(33.3%) - - |
0.88 |
| RV function, n (%), assessed by FAC Normal (>35%) Mild RV dysfunction (25-34%) Moderate RV dysfunction (18-24%) Severe RV dysfunction (< 17%) |
12(100%) - - - |
11(73.3%) 3(20%) 1(6.66%) - |
12(100%) - - - |
0.52 |
| PAP: Pulmonary Artery Pressure; LVEF: Left Ventricle Ejection Fraction; MR: Mitral Regurgitation; TR: Tricuspid Regurgitation; RV: Right Ventricle; FAC: Fractional Area Change.
Data are presented as mean ± standard deviation. |
||||
Table 3: Speckle tracking echocardiographic parameters..
| Parameters | No rejection | Mild rejection | Mild to moderate & Moderate | P-value |
|---|---|---|---|---|
| Apical rotation (degrees) | 5.09 ± 2.3 | 4.5 ± 1.52 | 2.2 ± 0.43 | 0.552 |
| Basal rotation (degrees) | -3.51 ± 2.6 | -3.41 ± 0.9 | -3.02 ± 0.4 | 0.548 |
| Time to peak apical rotation (msec) | 220 ± 0.04 | 460 ± 0.01 | 730 ± 0.02 | 0.01 |
| Time to peak basal rotation (msec) | 250 ± 0.05 | 440 ± 0.04 | 550 ± 0.11 | 0.004 |
| Time to peak apical rotation/R-R | 0.32 ± 0.001 | 0.35 ± 0.004 | 0.71 ± 0.001 | 0.08 |
| Time to peak basal rotation/R-R | 0.28±0.005 | 0.39±0.003 | 0.74 ±0.02 | 0.015 |
| Time to onset of apical rotation (msec) | 32.5 ± 0.06 | 36.5 ± 0.01 | 41.5 ± 0.02 | 0.8 |
| Time to onset of basal rotation (msec) | 54.8 ± 0.1 | 61.5 ± 0.1 | 64.8 ± 0.2 | 0.53 |
| LV Torsion (degrees/cm) | 1.24 ± 0.25 | 1.03 ± 0.22 | 0.7 ± 0.25 | 0.005 |
| LV Twist (degrees) | 9.53 ± 1.94 | 7.92 ± 1.6 | 5.2 ± 0.28 | 0.004 |
| Global longitudinal strain (%) | -17.6 ± 2.2 | -16.5 ± 2.17 | -15.7 ± 1.1 | 0.53 |
| Global circumferential strain (%) | -27.2 ± 2.3 | -23.5 ± 1.78 | -22.5 ± 2.34 | 0.001 |
R-R indicates R-R interval on ECG.
Table 4: Correlation between LV deformities and EF.
| LV Ejection Fraction | ||
|---|---|---|
| Parameters | Correlation coefficient | P-value |
| LV Torsion | 0.58 | 0.008 |
| LV Twist | 0.62 | 0.033 |
| Apical Rotation | 0.6 | 0.04 |
| Basal Rotation | 0.3 | |
| Global longitudinal strain | 0.59 | 0.001 |
| Global circumferential strain | 0.577 | 0.001 |
| Time to peak apical rotation/RR | 0.18 | 0.36 |
| Time to peak basal rotation/RR | 0.03 | 0.88 |
| LV: Left Ventricle, R-R indicates: R-R interval on ECG | ||
Discussion
The LVEF doesn’t differ significantly between a normal heart and a transplanted heart. But strain values of the entire LV are considered to be meaningfully lower in HT patients than those in healthy individuals. In this regard, GLS is the first strain that is reduced early after transplantation. Furthermore, LV twist and rotation values of HT patients are significantly lower compared with healthy individuals. LV remodeling, as a sequence of various factors such as reperfusion injury and immunosuppression therapy, leads to myocardial damage, which is responsible for the impairment of GLS, twist, and rotation values in the transplanted heart. On the other, in healthy individuals, the pericardium maintains cardiac twisting and torsional movement properly. It is assumed that deterioration of LV twist and rotation values in HT patients could be related to eliminating the pericardium supportive role too [8,28].
In this study, we ascertained that the LV torsion and twist values were reduced in rejected hearts compared to those derived from non-rejected hearts. Additionally, the study results demonstrated a significant correlation between LV twist and rejection severity. A cut-off point of 7.8 degrees for LV twist enables us to predict rejection in heart transplant recipients with good sensitivity and specificity. Actually, the novelty of our study was the determination of a threshold value in one of the STE parameters, i.e., twist, which assists us in distinguishing the HT rejection group from the non-rejection one. Furthermore, we found that time to peak apical and basal rotation had an independent correlation with rejection grades.
Acute rejection is an important cause of mortality in the first year after heart transplantation. Early diagnosis, particularly in the subclinical phase, is critical. EMB is the gold standard for detection of rejection, although this method is invasive and associated with severe complications [29].
In 1987, reduced LV-torsion values were reported in heart transplants with high-grade rejection by calculating torsion parameters by invasively applying myocardium markers [22]. However, in our study, as a non-invasive method for measuring LV-torsion, we used 2D-STE; moreover, we determined a cut-off point for specifying the rejections, which is not necessarily limited to the so-called high grade of rejection; hence this study is based on analysis of LV-torsion, which can identify relatively low grades of rejection. Other than echocardiography, MRI has been employed for measuring LV-torsion, although it is an expensive and time-consuming procedure [14]. Conversely, 2D-STE has been known as a non-invasive and easily available method for measuring LV-Torsion parameters [6].
Data from echocardiographic studies support the substitution of echocardiography as a non-invasive, readily available, and sensitive method for diagnosing acute rejection. In 2015, Ambardekar et al. concluded that strain and strain rate derived from STE are unable to predict acute rejection in HTx recipients [30].
In 2016, although Kato et al. also applied strain rate imaging, derived from tissue Doppler, to monitor HTx recipients, they reported that strain rate imaging could predict acute rejection [29]. However, tissue Doppler is an angle-dependent method, and for more accuracy, it is necessary to have the patient lying in a lateral position [29]. In our study, torsion deformity derived from 2D-STE, an angle-independent method, was applied for monitoring HTx recipients.
Sato et al. recently reported that LV-torsion values obtained from 2D-STE are helpful in diagnosing rejections [6]; this study was conducted following Takahiro’s observation to confirm his results. Furthermore, in our study, we investigated the direct correlation of rejection severity with time to peak apical and basal rotation values independently.
In parallel, we also evaluated GLS & GCS values derived from 2D-STE in the HTx recipient groups. By definition, changes in the myocardium length from the base to the apex of LV and along the circumferential axis of LV are expressed as longitudinal and circumferential strain, respectively [25]. Previous studies have aimed to assess the reliability of STE-derived strain measurements, including GLS and GCS, as a non-invasive method for early detection of acute rejection in HTx. Unfortunately, there were significant discrepancies in the results [8,10,11,30]. Andrew et al. investigated that GCS is significantly decreased in patients with rejection, while there was no significant difference in GLS values between rejection and no rejection groups [8]. Conversely, another study concluded that lower absolute values of GLS were present in acute rejection HT patients compared with those without rejection [31]. In this study, we verified no meaningful difference in the LV longitudinal strain between no rejection and rejection groups. Conversely, lower absolute values of the LV circumferential strain were present in the rejection group compared to those without rejection. From the results of studies, GLS is impaired in normal HT patients. Decreased GLS values occur soon after transplantation as a consequence of injuries (e.g., reperfusion injury, cell rejection reaction after surgery, immunosuppressive agents). It appears that preserved GCS value is the main strain deformation that maintains LV function in HT patients. After acute subclinical rejection, GCS is impaired, resulting in cardiac dysfunction. In this setting, LVEF and other 2D echocardiographic parameters could still be within normal limitation [8].
It seems that more evaluation is needed via further studies to clarify these discrepancies.
Clinical implications
EMB is the gold standard for early diagnosis of acute rejection in heart transplants, which is an invasive method accompanied by several complications. Up to now, no non-invasive modality has replaced the biopsy. Echocardiography is an available method for evaluating cardiac dysfunction resulting from acute HT rejection. As we know, LVEF impairment occurs relatively late in acute rejection HT patients when extensive myocardial damage has been established. Early detection of acute rejection in the subclinical stage has an important clinical implication, and it seems to be one of the indications for using 2D -STE. In the present study, we demonstrated that the utility of some deformity indexes derived from STE could be helpful for the early diagnosis of acute rejection. In this regard, we ascertained that mean twist and torsion values were significantly reduced with rejection. It was determined a threshold value for twist deformity to detect rejection.
Furthermore, we found that absolute values of LV-GCS were decreased in acute rejection. These deformity impairments proceed of reduction in LVEF, which occurs late. It appears that 2D-STE deformity indexes could serve as a reliable method for assessing HT rejection. Hopefully, in the future, EMB will replace with non-invasive tools for monitoring HT patients.
Limitations
This study has some limitations; firstly, since our study was conducted in a short time, we could not follow each heart transplant recipient after heart surgery up to their regular consecutive rejection screening by EMB; as far as possible, we compared different patients with each other; secondly, we were unable to evaluate transplant vasculopathy, because of which we could not consider its effect on the transplanted heart and subsequent changes in the LV-torsion deformities; thirdly, considering the low rate of heart transplantation surgeries, the number of HTx recipients was limited, hence our small sample size.Finally, despite the advantages served by 2D-STE, this modality has several limitations. The main limitation of 2D-STE is the difficulty of acquiring high-quality images with optimal echocardiographic visual assessment of the endocardial border. This limitation leads to excluding subjects with suboptimal-quality images. (About 14% in our study). In appropriate low or high frame rates, obtaining views with foreshortening of the LV, and incorrect positioning of the standard anatomic landmarks are other limitations of 2D-STE [15,32,33]. Some 2D-STE limitations could be overcome by 3D-STE. But 3D-STE by itself has multiple limitations too, that have made it more used as a research modality rather than a routine clinical tool. 3D-STE image acquirement requires cooperative patients for breath-holding. Achievement of optimal quality data is an essential factor for analyzing 3D-STE too. Patients with irregular heart rhythms are another limitation for using 3D-STE because 3D-STE needs multi-beats’ utility for imaging acquisitions. Besides, 3D echocardiography has a low temporal and spatial resolution. Ultimately, lack of practical experience leads to 3D-STE modality for clinical purposes [34]. On the other hand, the restricted availability of 3D echocardiography, prevents the routine utility of this technique. For these reasons, we didn’t apply 3D-STE in our study.
Conclusion
LV torsion deformity index derived from 2D-STE could be a useful method for non-invasive screening of acute rejection in HTx recipients. Further research is required to underscore the usefulness of LV-torsion deformities obtained from echocardiography as an alternative non-invasive, simple, and reliable screening method for EMB in the diagnosis of rejection in heart transplant patients.
Declarations
Conflict of interests & ethics: The authors of this research wish to confirm that there are no conflicts of interest associated with this publication. No financial support was received for this work from any institution or persons that could have influenced its outcome.
The terms of this arrangement have been reviewed and approved by the “Echocardiography Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.” The Approval ID of this studycertified by the Ethics Committee of Rajaie Cardiovascular Medical and Research Center is: “RHC.AC.IR.REC.1395.11”
Acknowledgments: We would like to acknowledge the head and personnel of the Adult Echocardiography ward of the Rajaie Cardiovascular Medical and Research Center, who sincerely cooperated with us in this research.
Disclosure statement: “Drs. A.A.aaz, A.A., A.S., S.T., L.N., K.M., and L.J. have no conflicts of interest or financial ties to disclose.”
References
- Alraies MC, Eckman P. Adult heart transplant: indications and outcomes. J Thorac Dis. 2014; 6: 1120-1128.
- Westerdahl DE, Kobashigawa JA. Heart Transplantation for Advanced Heart Failure. Cardiac Intensive Care. 2019; 504-524 e2.
- Khush KK, Cherikh WS, Chambers DC, Goldfarb S, Hayes D, Kucheryavaya AY, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth Adult Heart Transplantation Report-2018; Focus Theme: Multiorgan Transplantation. J Heart Lung Transplant. 2018; 37: 1155-1168.
- John R, Rajasinghe HA, Chen JM, Weinberg AD, Sinha P, Mancini DM, et al. Long-term outcomes after cardiac transplantation: An experience based on different eras of immunosuppressive therapy. The Annals of Thoracic Surgery. 2001; 72: 440-449.
- Grauhan O, Müller J, v Baeyer H, Volk HD, Fietze E, Cohnert T, et al. Treatment of humoral rejection after heart transplantation. J Heart Lung Transplant. 1998; 17: 1184-1194.
- Sato T, Kato TS, Komamura K, Hashimoto S, Shishido T, Mano A, et al. Utility of left ventricular systolic torsion derived from 2-dimensional speckle-tracking echocardiography in monitoring acute cellular rejection in heart transplant recipients. J Heart Lung Transplant. 2011; 30: 536-543.
- Strecker T, Rösch J, Weyand M, Agaimy A. Endomyocardial biopsy for monitoring heart transplant patients: 11-years-experience at a german heart center. Int J Clin Exp Pathol. 2013; 6: 55-65.
- Tseng AS, Gorsi US, Barros-Gomes S, Miller FA, Pellikka PA, Clavell AL, et al. Use of speckle-tracking echocardiography-derived strain and systolic strain rate measurements to predict rejection in transplant hearts with preserved ejection fraction. BMC cardiovascular disorders. 2018; 18: 241.
- Dengler TJ, Zimmermann R, Braun K, Müller-Bardorff M, Zehelein J, Sack FU, et al. Elevated serum concentrations of cardiac troponin T in acute allograft rejection after human heart transplantation. J Am Coll Cardiol. 1998; 32: 405-412.
- Cruz C, Hajjar LA, Bacal F, Lofrano-Alves MS, Lima MSM, Abduch MC, et al. Usefulness of speckle tracking echocardiography and biomarkers for detecting acute cellular rejection after heart transplantation. Cardiovasc Ultrasound. 2021; 19: 6.
- Olymbios M, Kwiecinski J, Berman DS, Kobashigawa JA. Imaging in Heart Transplant Patients. JACC Cardiovasc Imaging. 2018; 11: 1514-1530.
- Sera F, Kato TS, Farr M, Russo C, Jin Z, Marboe CC, et al. Left ventricular longitudinal strain by speckle-tracking echocardiography is associated with treatment-requiring cardiac allograft rejection. J Card Fail. 2014; 20: 359-364.
- Gustafsson U, Lindqvist P, Mörner S, Waldenström A. Assessment of regional rotation patterns improves the understanding of the systolic and diastolic left ventricular function: An echocardiographic speckle-tracking study in healthy individuals. Eur J Echocardiogr. 2009; 10: 56-61.
- Rüssel IK, Tecelão SR, Kuijer JP, Heethaar RM, Marcus JT. Comparison of 2D and 3D calculation of left ventricular torsion as circumferential-longitudinal shear angle using cardiovascular magnetic resonance tagging. J Cardiovasc Magn Reson. 2009; 11: 8.
- Mora V, Roldán I, Romero E, Romero D, Bertolín J, Ugalde N, et al. Comprehensive assessment of left ventricular myocardial function by two-dimensional speckle-tracking echocardiography. Cardiovascular ultrasound. 2018; 16:16.
- Nottin S, Ménétrier A, Rupp T, Boussuges A, Tordi N, et al. Role of left ventricular untwisting in diastolic dysfunction after long duration exercise. European Journal of Applied Physiology. 2012; 112: 525-533.
- Nakatani S. Left ventricular rotation and twist: why should we learn? J Cardiovasc Ultrasound. 2011; 19: 1-6.
- Park SJ, Nishimura RA, Borlaug BA, Sorajja P, Oh JK, et al. The effect of loading alterations on left ventricular torsion: A simultaneous catheterization and two-dimensional speckle tracking echocardiographic study. Eur J Echocardiogr. 2010; 11: 770-777.
- Rüssel IK, Götte MJ, Bronzwaer JG, Knaapen P, Paulus WJ, van Rossum AC, et al. Left ventricular torsion: An expanding role in the analysis of myocardial dysfunction. JACC Cardiovasc Imaging. 2009; 2: 648-655.
- Sengupta PP, Khandheria BK, Narula J. Twist and untwist mechanics of the left ventricle. Heart Fail Clin. 2008; 4: 315-324.
- Omar AM, Vallabhajosyula S, Sengupta PP. Left ventricular twist and torsion: Research observations and clinical applications. Circ Cardiovasc Imaging. 2015; 8.
- Hansen DE, Daughters GT, 2nd, Alderman EL, Stinson EB, Baldwin JC, Miller DC, et al. Effect of acute human cardiac allograft rejection on left ventricular systolic torsion and diastolic recoil measured by intramyocardial markers. Circulation. 1987; 76:998-1008.
- Donofrio MT, Clark BJ, Ramaciotti C, Jacobs ML, Fellows KE, Weinberg PM, et al. Regional wall motion and strain of transplanted hearts in pediatric patients using magnetic resonance tagging. Am J Physiol. 1999; 277: R1481-R1487.
- Cameli M, Ballo P, Lisi M, Benincasa S, Focardi M, Bernazzali S, et al. Left ventricular twist in clinically stable heart transplantation recipients: A speckle tracking echocardiography study. Int J Cardiol. 2013; 168: 357-361.
- Johnson C, Kuyt K, Oxborough D, Stout M. Practical tips and tricks in measuring strain, strain rate and twist for the left and right ventricles. Echo Res Pract. 2019; 6: R87-R98.
- Sugimoto T, Dulgheru R, Bernard A, Ilardi F, Contu L, Addetia K, et al. Echocardiographic reference ranges for normal left ventricular 2D strain: Results from the EACVI NORRE study. Eur Heart J Cardiovasc Imaging. 2017; 18: 833-840.
- Pryds K, Larsen AH, Hansen MS, Grøndal AYK, Tougaard RS, Hansson NH, et al. Myocardial strain assessed by feature tracking cardiac magnetic resonance in patients with a variety of cardiovascular diseases - A comparison with echocardiography. Sci Rep. 2019; 9: 11296.
- Wang D, Zhang L, Zeng Q, Xie M. Assessment of left ventricular performance in heart transplant recipients by three-dimensional speckle tracking imaging. Medicine. 2017; 96: e8129.
- Kato TS, Oda N, Hashimura K, Hashimoto S, Nakatani T, Ueda HI, et al. Strain rate imaging would predict sub-clinical acute rejection in heart transplant recipients. Eur J Cardiothorac Surg. 2010; 375: 1104-1110.
- Ambardekar AV, Alluri N, Patel AC, Lindenfeld J, Dorosz JL, et al. Myocardial strain and strain rate from speckle-tracking echocardiography are unable to differentiate asymptomatic biopsy-proven cellular rejection in the first year after cardiac transplantation. J Am Soc Echocardiogr. 2015; 28: 478-485.
- Mingo-Santos S, Moñivas-Palomero V, Garcia-Lunar I, Mitroi CD, Goirigolzarri-Artaza J, Rivero B, et al. Usefulness of Two-Dimensional Strain Parameters to Diagnose Acute Rejection after Heart Transplantation. J Am Soc Echocardiogr. 2015; 28: 1149-1156.
- Blessberger H, Binder T. NON-invasive imaging: Two dimensional speckle tracking echocardiography: Basic principles. Heart (British Cardiac Society). 2010; 96: 716-722.
- Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Journal of the American Society of Echocardiography : Official publication of the American Society of Echocardiography. 2015; 28: 183-193.
- Muraru D, Niero A, Rodriguez-Zanella H, Cherata D, Badano L, et al. Three-dimensional speckle-tracking echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovascular diagnosis and therapy. 2018; 8:101-117.