
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Chronic pulmonary aspergillosis after post-tuberculosis
lung disorders misdiagnosed as tuberculosis, acquiring
more attention: Case series and literature review
Ying Liu; Su-Yue Sun; Xiao-Yan Gu; Chun-Mei Hu*
Department of Tuberculosis, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing 210003, China.
*Corresponding Author : Chun-Mei Hu, MD
The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, 1-1 Zhongfu Road, Gulou District, Nanjing 210003, Jiangsu Province, China.
Email: njyy003@njucm.edu.cn
Received : Apr 15, 2023
Accepted : May 12, 2023
Published : May 19, 2023
Archived : www.jcimcr.org
Copyright : © Chun-Mei H (2023).
Abstract
Background: Chronic Pulmonary Aspergillosis (CPA) is a destructive pulmonary disease caused by a fungal infection, a frequent complication of treated Tuberculosis (TB). Pulmonary Tuberculosis (PTB) is a major risk factor for Chronic Pulmonary Aspergillosis (CPA) due to residual structural destruction. Numerous studies and literatures show that CPA is the most common infection after PTB and incidences of CPA in high-TB-burden countries are significantly higher than in low TB-load countries. Differential diagnosis is quite difficult and used to be ignored. However, there is few systematic literature nor review summarizing their identification points. This article is aim to summarize the key points in the differential diagnosis of pulmonary aspergillosis and tuberculosis, and promote the awareness of clinician about differential diagnosis between them.
Methodology: Clinical data were collected from patients hospitalized in the Department of Tuberculosis, Nanjing Second Hospital, from August 2019 to March 2021, who were initially misdiagnosed with smear negative tuberculosis and finally diagnosed as CPA. Then retrospectively analyze the data and combine with literature review.
Results: Of 5638 patients, 4397 patients are diagnosed as pulmonary tuberculosis at first, hospitalized in Tuberculosis Department of Nanjing Second hospital. Of 4397, 659 patients were relapsed tuberculosis. Of 659 relapsed tuberculosis patients, 273 patients were initially judged as smear-negative recurrent PTB. And finally, 5 patients were eventually confirmed as CPA of the 273 patients.
Differential diagnosis between CPA and PTB relies on specific microbiological and serological tests due to the striking similarities in the clinical symptom and radiological manifestations, especially smear-negative PTB. However, Immunological evidence related to tuberculosis can be easily available on patients with Tuberculosis (TB) history. Aspergillus-specific IgG is particularly sensitive, playing an important role in distinguishing them. Aspergillus fumigatus Immunoglobin G (IgG) can be positive in 90% CPA patients. The sensitivity and specificity of the lavage Galactomannan (GM) test is much higher than serum GM test.Bacteriological testing is also essential but sometimes. If the diagnosis gets stuck, Metagenomic Next-Generation Sequencing (mNGS) can be a useful and available tool which can help catch pathogenetic evidence.
Conclusion: Differential diagnosis between CPA and PTB relies on specific microbiological and serological tests. Aspergillus-specific IgG is a key point in distinguishing CPA from tuberculosis recurrence. mNGScan beneficially improve the diagnosis of CPA with high sensitivity and specificity.
Keywords: Pulmonary tuberculosis; Chronic pulmonary aspergillosis; Misdiagnosis; Differential diagnosis.
Abbreviations: CT: Computed tomography; PTB: Pulmonary tuberculosis; CPA: Chronic pulmonary aspergillosis; TB: Tuberculosis; CPH: Chronic pulmonary histoplasmosis; ABPA: Allergic bronchopulmonary aspergillosis; PTBLD: Pulmonary tuberculosis lung disease; CCPA: Chronic cavitary aspergillosis; CFPA: Chronic fibrotic aspergillosis; PPD: Purified protein derivative; ELISA: Enzyme linked Immunosorbent sorbent assay; mNGS: Metagenomic next-generation sequencing; IgG: Immunoglobin G; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate; GM: Galactomannan.
Citation: Ying L, Su-Yue S, Xiao-Yan G, Chun-Mei H. Chronic pulmonary aspergillosis after post-tuberculosis lung disorders misdiagnosed as tuberculosis, acquiring more attention: Case series and literature review. J Clin Images Med Case Rep. 2023; 4(5): 2422.
Background
Tuberculosis (TB) is a contagious infection caused by Mycobacterium tuberculosis (MTB), which is still a major threat for global public health [1]. For many years, substantial resources are input for TB prevention and treatment, to achieve the “End TB” target. Recently, more and more attentions are paid for long-term outcomes of treated TB patients [2,3]. Although TB is curable through anti-TB chemotherapy, approximately two-thirds of pulmonary TB patients suffer from extensive structural lung changes after microbiological cure of active TB. These residual changes are called post-TB lung disease (PTBLD) [4], which is a risk factor for recurrent TB and other infectious complications [5].
Chronic Pulmonary Aspergillosis (CPA) is a severe destructive pulmonary disease caused by the mould Aspergillus, with a global prevalence of 42 per 100,000 population and 10-year mortality of upto 50% [6,7]. CPA is a frequent complication of treated PTB and 15-90% of CPA cases occur in patients with PTBLD [8,9]. There is great challenge for diagnosis of CPA because it is highly similar to pulmonary TB in regards of clinical presentation and radiological appearances [8]. CPA is often misdiagnosed as smear-negative pulmonary TB or relapsed TB, especially in high TB burden countries and regions, leading to treatment failure [10,11]. CPA post TB has become an emerging public healthconcern [12].
China is a high TB burden developing country, accounting for 8.5% of TB cases worldwide in 2020. In 2017, a retrospectively study screened 690 patients diagnosed with pulmonary aspergillosis in Beijing and found 10% of them were CPA [13]. Recently, another retrospective analysis summarized the clinical features and risk factors of pulmonary aspergillosis complicated with pulmonary TB, but not CPA [14]. To our knowledge, there is few published study on prevalence of CPA post TB in China, neither the case reports of CPA patients misdiagnosed as TB, indicating that there is not enough awareness for CPA. Our hospital, the Second Hospital of Nanjing, is a designed hospital for infectious diseases in Nanjing district, Southeast China. We retrospectively analyzed the electronic medical record of 5638 patients hospitalized in the Department of Tuberculosis from August 2019 to March 2021, and found 5 CPA patients were initially misdiagnosed as TB. Their clinical and radiological features were summarized. In particular, we emphasized one CPA case with Aspergillus-specific IgG negative was finally diagnosed by Metagenomic Next-Generation Sequencing (MNGS). Our study would help TB clinicians in resource-limited settings keep CPA in mind when suspecting smear-negative TB.
Methods
This retrospective study screened 5638 patients hospitalized in the Department of Tuberculosis, the Second Hospital of Nanjing, from August 2019 to March 2021. All of them were admitted because of TB. Their electronic medical records were analyzed, including age, sex, clinical symptom, serologic examination, image features, bronchoscopy, and microbiologic results.
Diagnostic criteria of CPA
The diagnostic criteria of CPA are referred to the European guideline [1]. First, there is a consistent appearance in thoracic imaging (preferably by CT). Second, there is direct evidence of Aspergillus infection or an immunological response to Aspergillus spp. Third, respiratory and/or constitutional symptoms have been present for at least 3 months, even if that duration is inferred and based on symptoms or progressive radiological abnormality. Fourth, some alternative diagnoses are excluded. Patients are usually not immunocompromised by HIV-infection, cancer chemotherapy or immunosuppressive therapy.
mNGS
BALF samples were collected from patients, and Mngs results of BALF were collected.
Results
From August 2019 to March 2021, 5638 patients were hospitalized in the Department of Tuberculosis, the Second Hospital of Nanjing. 4397 patients were diagnosed as pulmonary TB, among which, 659 (15%) patients were relapsed TB. Of these relapsed TB, 273 patients were initially diagnosed as smear-negative recurrent TB, among which 5 patients were finally diagnosed as CPA.
Demographic feature of CPA patients misdiagnosed as smear-negative recurrent TB 5 patients included 2 male and 3 female, aged 30-77 years, with an average age of 53 years and a median age of 54 years. Five patients were from different occupations and all had community-acquired infections. Two patients had a history of hepatitis B, and one patient had a history of diabetes. All patients tested negative for HIV.
Clinical symptom and laboratory examination
All 5 patients had cough and sputum, 3 patients had hemoptysis with a small amount of hemoptysis, no major hemoptysis, 1 patient had significant weakness during the course of the disease, and 2 patients had other atypical concomitant symptoms.After admission, the patient’s laboratory tests, leukocytes, CRP, ESR, serum G test and GM test were not significantly abnormal. G test and GM test of 1 patient are both positive. 4 patients were positive for Aspergillus IgG and 1 patient was negative. 2 patients found aspergillus sequence by NGS of lavage fluid and 1 patient sputum fungal culture: aspergillus positive (Table 1).
Table 1: Clinical data of 5 patients included.
| Patient | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Sex | Male | Female | Female | Female | Male |
| Age | 30 | 49 | 77 | 54 | 54 |
| Symptom | Cough with blood | Hemoptysis, cough and sputum | Cough and sputum | Cough, weakness | Cough and sputum, with blood |
| Tuberculosis history | Yes | Yes | Yes | Yes | Yes |
| Underlying disease | None | Hepatitis B | None | None | Diabetes, hepatitis B |
| Sputum smear for acid-fast bacilli | Negative | Negative | Negative | Negative | Negative |
| Sputum Gene X-PERT | Negative | Negative | Negative | Negative | Negative |
| Sputum fungal culture | Negative | Negative | Negative | Negative | |
| Serum G GM test | Negative | Negative | Negative | Negative | Negative |
| Aspergillus fumigatus IgG | Negative | Positive | Positive | Positive | Positive |
| Chest Image | Exudative shadow in both upper lungs, cavity-like changes in the right upper lung | Solid left upper lung lesion with branched enlargement | Cavitation-like changes in the upper lobe of the left lung | Upper lung plaque shadow in both, right upper lung cavity | Right upper lung striae and nodular shadow, left lower lung cavity, hemi-branch expansion |
| Bronchoscopy | No abnormalities in the lumen | - | - | Hypertrophy of the luminal mucosa and narrowing of the lumen | - |
| BALF G, GMtest | Both positive | - | - | Both negative | - |
| Lavage solution mNGS | Aspergillus genus | - | - | Aspergillus genus | - |
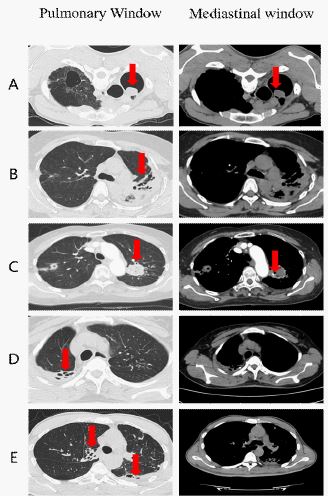
A: We performed prone CT on patient P1. Cavitation-like changes can be seen in the right upper lung with nodular changes and the position of aspergillus ballis affected with body position (in red arrow). B: Great damage of lung tissue was left. Bronchiectasis and multiple cavities can be seen in both lungs, especially in the left upper lung (in red arrow). C: A mass is seen in the left lung with calcification (in red arrow) and cavity is formed in the right lung. D: Patchy shadow in the right upper lung with multiple cavities (in red arrow), shaped like honeycombs. E: Bronchiectasis and hollow shadows are formed (in red arrow).
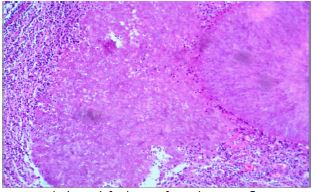
Table 2: Differential diagnostic key points between PTB and CPA.
| PTB | CPA | |
|---|---|---|
| Prevalent population | Immunocompetent or immunocompromised people | Immunocompromised people or people with destruction of lung parenchyma |
| Symptom | Cough, sputum, emaciation, night sweats, low fever in the afternoon, hemoptysis | Cough, sputum, hemoptysis (more common), wasting, weakness |
| Radiographic manifestations | It appears as fibrous, striated, calcified, and patchy lung tissue, with cavity formation and the typical "sprout sign" | Most of them are secondary to the destruction of lung tissue structure, cavity-like changes are common, there may be the formation of "varicose spheres" or the accumulation of necrotic material in the cavity, there may be halo signs, it may show fibrous, striated, patchy shadow, nodule-like changes, usually lymph nodes not involved |
| Serum immunological reference markers | PPD,T-SPOT,TB antibody | Aspergillus IgG, IgM, trichothecene precipitation, G, GM test |
| Bacteriological significance | Finding mycobacterium tuberculosis is gold standard for diagnosis | Aspergillus found in respiratory specimens, need to exclude the possibility of colonization |
| Structural basis of lung tissue | No special | structural destruction of lung tissue is risk factor |
| Bacteriological testing methods | Sputum smear for acid-fast bacilli, Gene X-PERT, mycobacterium tuberculosis DNA or RNA, mNGS | Sputum fungal culture mNGS |
| Pathological features | Granulomatous inflammation, anti-acid staining positive | Granulomatous inflammation, HE staining can be helpful |
Radiographic characteristic of CPA patients
Five patients underwent chest CT examinations, which showed varying degrees of destruction of lung tissue structure, with multiple solid patchy, nodular and striated changes in both lungs, accompanied by calcification and old tuberculosis-like changes of pleural thickening. Chest CT shows “cavitation” with fibrosis-like changes (Figure 1).
Fiberoptic bronchoscopy results
Case 1 and Case 4 underwent fiberoptic bronchoscopy after being hospitalized, bronchoscopy lavage liquid pathogenic assays test indicate: smear of lavage fluid to look for acid-resistant bacilli: negative, gene x-pert: negative, TB-DNA: negative. G and GM test of case 1 are both positive but of Case 4 are both negative. The pathology of the lavage fluid showed a large number of degenerated epithelioid cells, a large number of acute and chronic inflammatory cells, no malignant cells, and no aspergillus mycelium.
mNGS
To further ascertain the etiological agent, we decided to conduct Metagenomic Next-Generation Sequencing (mNGS) with the lavage fluids since Patient 1 and Patient 4 accepted fiberoptic bronchoscopy. To our interest, mNGS found 522 and 130 Aspergillus reads for Patient 1 and Patient 4, respectively.
Pathology
Case 1 finally received lung surgery, and pathology shows that chronic inflammatory cell infiltration and fungal mycelial masseswere observed (Figure 2).
Discussion
Literature review
We searched for literature after 2000 with “chronic pulmonary aspergillosis, misdiagnosis, tuberculosis” as keywords and conducted a literature search in PubMed. 11 relevant papers were retrieved [2-12], including 7 papers related to CPA, 2 papers related to ABPA, 1 paper related to invasive pulmonary aspergillosis, and 1 paper related to Chronic Pulmonary Histoplasmosis (CPH). Among the 7 CPA-related papers, 2 papers reported cases of CPA misdiagnosed as pulmonary tuberculosis, with a cumulative total of only 7 reported cases (5HIV-negative and 2 HIV-positive), 3 papers conducted statistical analysis and studies related to CPA misdiagnosed as pulmonary tuberculosis, and 1 paper emphasized the role of aspergillus antibodies in CPA and tuberculosis, and one article described the importance of trichothecene antibodies in the differential diagnosis of CPA and tuberculosis. In all, CPA is a common sequel after tuberculosis. Distinguish between them relies on laboratory test and CT.
Relationship between CPA and PTB
Tuberculosis is a chronic respiratory infection caused by mycobacterium tuberculosis. The 2022 WHO Global Tuberculosis Report shows that about one quarter of the global population is infected with mycobacterium tuberculosis, which is the number one killer among infectious diseases and poses a great threat to global public health [13]. There is still irreversible destruction of lung tissue structure caused by tuberculosis after being cured, leaving structural lung disease, including bronchiectasis, bronchial stenosis, fibrosis, and residual cavitation. Some studiessuggest about 2/3 of patients with tuberculosis had extensive structural changes in the lungs after cure, involving the lung parenchyma, blood vessels, airways, pleura and even the mediastinum [14-16]. Based on destroyed structure, various infections follow up and CPA is the most common after tuberculosis [7]. Residual cavities can be left after cure in 20-40% of patients [17,18]. PTBLD including structural changes and residual cavities provide a place for aspergillus spores to settle and multiply.
CPA is a rare fungal infection pulmonary disease, characterized by slowly progressivedestruction of lung parenchyma, in the form of single of multiple cavities, nodules, infiltrates or fibrosis, with or without an aspergilloma. Patients with preexisting pulmonary pathology or immune suppression can be infected. Research suggests pulmonary tuberculosis seems to be a relevant driver for CPA [19-21]. Besides, CPA is likely to occur secondary to pre-existing cavitary or herpetic lung disease. Estimates suggest about 3 million people are affected worldwide causing high rates of morbidity and mortality and making great burden to global health. Approximately, 1.2 million people with CPA have been affected by tuberculosis [22]. Infections after PTB lead to tremendous stress for countries of high TB burden and the incidence of CPA is significantly higher in high TB burden countries than in low TB burden countries [19]. China is one of high TB burden countries in the world and due to the geographical difference in medical level, especially in primary hospitals with relatively backward medical level, CPA after TB used to be misdiagnosed as bacillus-negative TB or drug-resistant TB due to the lack of awareness and backward management level, even in the absence of positive laboratory results., resulting in over-treatment of TB and waste of medical resources, and delaying patient treatment and bringing bad prognosis.Some of these patients are probably commenced on re-treatment anti-TB regimens, which are unnecessary and even potentially harmful in terms of toxicity. Also, in many conditions, people with continuous respiratory symptoms after TB cure may be believed to be recurrence of tuberculosis making poor prognosis.
The subtypes of CPA mainly include Chronic Cavitary Aspergillosis (CCPA), Chronic Fibrotic Aspergillosis (CFPA), aspergilloma (simple aspergilloma), aspergillus nodule (aspergillus nodule) and Invasive Pulmonary Aspergillosis (SAIA). CCPA is the most common form [23]. Chest imaging plays an important role in diagnostic finding, especially CT scan [24].
Differential diagnosis between CPA and PTB
The clinical manifestations are both non-specific and can be manifested as chronic cough, hemoptysis, weakness, chest tightness, wasting and other symptoms in PTB and CPA, and some patients even have no clinical symptoms. These symptoms are difficult to distinguish from each other. What is more, progressive cavitation, fibrosis, and pleural thickening can be seen in radiological presentation in both [14,25]. CPA is often secondary to PTB, diagnostic basis for bacillus-negative tuberculosis can be easily obtained therefore. However, the lack of awareness and low index of suspicion for CPA among clinicians, as well as the non-availability of essential diagnostics for CPA, are associated with misdiagnosis of CPA because of non-specific clinical presentation and similar imaging features.CCPA is the most common type of CPA after tuberculosis. All patients included in had a history of tuberculosis leaving destruction of lung tissue structure.
The five patients included in this study all had chronic cough and sputum symptoms, and had cavitation, fibrosis, plaque, and nodular shadow on chest CT. Tuberculosis pathogenicity indicators were negative including Gene X-PERT, but due to the clinicians’ initial lack of knowledge about CPA, they were empirically diagnosed with bacillus-negative tuberculosis without ruling out CPA or other pathogenic infections.
Given the similarity of the clinical and imaging manifestations of CPA and tuberculosis, the differential diagnosis between them is more dependent on laboratory and microbiological tests. Serum specific aspergillus IgG occupies an important position in the differential diagnosis of CPA and bacillary-negative PTB [19,23,26,27]. ELISA assay is more sensitive than traditional aspergillus trichothecene precipitation test, but immunodeficient patients may have the possibility of false negatives due to antibody immune non-response [26,28,29]. The sensitivity and specificity of the lavage GM test is much higher than that of the serum GM test, so the diagnosis of CPA should focus on the lavage GM test. Metagenomic second-generation sequencing, as a novel pathogenic microbial gene detection tool, can theoretically detect all pathogens in samples, including bacteria, fungi and viruses in a rapid and unbiased manner. Compared to traditional pathogenic detection methods, it beneficially improves the diagnosis of fungal infectious lung diseases with high sensitivity and specificity, making great improvement for the early diagnosis of CPA [29-31].
Diagnosis of CPA is complex. Discovering aspergillus fumigatus in sputum is not diagnostic of CPA, due to the prevalence of aspergillus presence, and the possibility of colonization needs to be excluded [19]. In the five patients included in this study, aspergillus was detected in the respiratory tract of three patients, and the clinical diagnosis of CPA was made after combining the patients’ clinical symptoms, chest CT imaging findings, and serum immunological indexes. Therefore, the diagnosis of CPA is more dependent on clinical evidence and imaging manifestations, and requires a comprehensive judgment by the clinician. However, etiologic evidence is the “gold standard” for tuberculosis. The diagnosis is made once mycobacterium tuberculosis is found in the sputum or lavage fluid. Currently, only 63% of TB patients worldwide are Gene X-PERT positive [13], and China is still a developing country with some economically underdeveloped areas that do not yet have the capability of Gene X-PERT testing and insufficient diagnostic capability for TB. The diagnosis of bacillus-negative tuberculosis relies on immunological tests for tuberculosis: PPD, T-SPOT, blood tuberculosis antibody-related indicators, in combination with the patient’s imaging, to make the clinical diagnosis. The immunological evidence can often be readily found in patients with relapsed PTB.Therefore, in primary hospitals and less developed areas, it is easy to make misdiagnosis and underdiagnosis of CPA, resulting in poor prognosis. The five patients in this case all had calcification, fibrous striae, pleural thickening on CT lung imaging, and overlap of lesion sites with TB predilection sites, cavities in the lung lesions. Imaging manifestations are highly consistent with pulmonary TB, and all had a previous history of TB, which was initially misdiagnosed as TB by the receiving physician due to the limitations of the tuberculosis specialty. After admission to the hospital, the aspergillus IgG test was perfected to seek the pathogenic basis and find the differential diagnosis, and combined with the patient’s chest CT imaging performance, the diagnosis of CPA was finally confirmed, and after receiving antifungal treatment, the follow-up prognosis was all good. In addition, the pathological features of both PTB and CPA can be manifested as granulomatous inflammation. And the differentiation of the two needs to be done with the help of special staining. Positive antacid staining is a pathological feature of PTB, and pathology of CPB can find aspergillus filaments or aspergillus clusters, and HE staining can help in the diagnosis (Table 2).
The patients included in this study all perfected the aspergillus IgG test. What is more, clinicians tried to search for the pathogenic basis in order to catch the differential diagnosis evidence. Combining with the patient’s chest CT imaging performance, the final diagnosis of CPA was confirmed.After receiving antifungal treatment, the follow-up prognosis was good.
Conclusion
Because of similar symptom and chest image, CPA can be misdiagnosed as smear-negative PTB especially in resource-limited areas. Differential diagnosis between CPA and PTB relies on specific microbiological and serological tests. Aspergillus-specific IgG is a key point in distinguishing CPA from tuberculosis recurrence. mNGS can beneficially improve the diagnosis of CPA with high sensitivity and specificity. Greater awareness of PTBLD among clinicians is therefore warranted in order to avoid overtreatment of tuberculosis and waste of medical resources.
Declarations
Ethics approval and consent to participate: This study was reviewed and approved by the ethics committee of the Second Hospital of Nanjing (2019-LS-ky004). All patients were fully informed of the risks and provided written informed consent before enrolment.
Consent for publication: Not applicable.
Availability of data and materials: Data relating to this study are contained and presented in document. Other materials are available from the corresponding authors on reasonable request.
Competing interests: No competing interests conflicts.
Funding: Not applicable.
Authors’ contributions: Chun-Mei Huand Xiao-Yan Gu designed the study, performed the operation, and revised the manuscript critically. YingLiu, Su-Yue Sun were responsible for collecting the date and writing the article, referring to the related literature. All authors read and approved the final manuscript.
Acknowledgements: Not applicable.
References
- DW Denning, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management [J]. Eur Respir J. 2016; 47: 45-68.
- J Baker, Kosmidis C, Rozaliyani A, et al. Chronic Pulmonary Histoplasmosis-A Scoping Literature Review [J]. Open Forum Infect Dis. 2020; 7: a119.
- A Rozaliyani, Rosianawati H, Handayani D, et al. Chronic Pulmonary Aspergillosis in Post Tuberculosis Patients in Indonesia and the Role of LDBio Aspergillus ICT as Part of the Diagnosis Scheme [J]. J Fungi (Basel). 2020; 6.
- R Kwizera, Katende A, Bongomin F, et al. Misdiagnosis of chronic pulmonary aspergillosis as pulmonary tuberculosis at a tertiary care center in Uganda: A case series [J]. J Med Case Rep. 2021; 15: 140.
- F Setianingrum, Rozaliyani A, Adawiyah R, et al. A prospective longitudinal study of chronic pulmonary aspergillosis in pulmonary tuberculosis in Indonesia (APICAL) [J]. Thorax. 2021.
- X Ma, Wang K, Zhao X, et al. Prospective study of the serum Aspergillus-specific IgG, IgA and IgM assays for chronic pulmonary aspergillosis diagnosis [J]. BMC Infect Dis. 2019; 19: 694.
- K Jabeen. Pulmonary infections after tuberculosis [J]. Int J Mycobacteriol. 2016; 5: S73.
- R Prasad, Garg SR. Progressive increase in cavitation with the evolution of fungus ball: A clue to the diagnosis of chronic necrotizing pulmonary aspergillosis [J]. Lung India. 2009; 26: 95-97.
- MH Nguyen, Jaber R, Leather HL, et al. Use of bronchoalveolar lavage to detect galactomannan for diagnosis of pulmonary aspergillosis among nonimmunocompromised hosts [J]. J Clin Microbiol. 2007; 45: 2787-2792.
- N Iqbal, Amir Sheikh-MD, Jabeen K, et al. “Allergic bronchopulmonary aspergillosis misdiagnosed as smear negative pulmonary tuberculosis; a retrospective study from Pakistan” [J]. Ann Med Surg (Lond), 2021; 72103045.
- M Zhang, Gao J. Clinical Analysis of 77 Patients with Allergic Bronchopulmonary Aspergillosis in Peking Union Medical College Hospital [J]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2017; 39: 352-357.
- SY Zhao, Jiang ZF, Xu SY. Diagnosis and treatment of chronic pulmonary aspergillosis in 4 children][J]. Zhonghua Er Ke Za Zhi. 2005; 43: 113-117.
- World Health Organization. ( 2022) . Global tuberculosis report 2022. World Health Organization. https://apps.who.int/iris/handle/10665/363752.
- R Khan, Malik NI, Razaque A. Imaging of Pulmonary Post-Tuberculosis Sequelae [J]. Pak J Med Sci. 2020; 36: S75-S82.
- J Meghji, Simpson H, Squire SB, et al. A Systematic Review of the Prevalence and Pattern of Imaging Defined Post-TB Lung Disease [J]. PLoS One. 2016; 11: e161176.
- B Menon, Nima G, Dogra V, et al. Evaluation of the radiological sequelae after treatment completion in new cases of pulmonary, pleural, and mediastinal tuberculosis [J]. Lung India. 2015; 32: 241-245.
- NL Smith, Denning DW. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma [J]. Eur Respir J. 2011; 37: 865-872.
- MT Hedayati, Azimi Y, Droudinia A, et al. Prevalence of chronic pulmonary aspergillosis in patients with tuberculosis from Iran [J]. Eur J Clin Microbiol Infect Dis. 2015; 34: 1759-1765.
- DW Denning, Pleuvry A, Cole DC. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis [J]. Bull World Health Organ. 2011; 89: 864-872.
- A Rozaliyani, Rosianawati H, Handayani D, et al. Chronic Pulmonary Aspergillosis in Post Tuberculosis Patients in Indonesia and the Role of LDBio Aspergillus ICT as Part of the Diagnosis Scheme [J]. J Fungi (Basel). 2020; 6.
- F Bongomin. Post-tuberculosis chronic pulmonary aspergillosis: An emerging public health concern [J]. PLoS Pathog. 2020; 16: e1008742.
- GD Brown, Denning DW, Gow NA, et al. Hidden killers: Human fungal infections [J]. Sci Transl Med. 2012; 4: 113r-165r.
- DW Denning, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management [J]. Eur Respir J. 2016; 47: 45-68.
- DW Denning, Page ID, Chakaya J, et al. Case Definition of Chronic Pulmonary Aspergillosis in Resource-Constrained Settings [J]. Emerg Infect Dis. 2018; 24.
- JB Baluku, Nuwagira E, Bongomin F, et al. Pulmonary TB and chronic pulmonary aspergillosis: clinical differences and similarities [J]. Int J Tuberc Lung Dis. 2021; 25: 537-546.
- ID Page, Richardson MD, Denning DW. Comparison of six Aspergillus-specific IgG assays for the diagnosis of Chronic Pulmonary Aspergillosis (CPA) [J]. J Infect. 2016; 72: 240-249.
- D Hsu, Irfan M, Jabeen K, et al. Post tuberculosis treatment infectious complications [J]. Int J Infect Dis. 2020; 92SS41-S45.
- C Kosmidis, Denning DW. The clinical spectrum of pulmonary aspergillosis [J]. Thorax. 2015; 70: 270-277.
- H Li, Gao H, Meng H, et al. Detection of Pulmonary Infectious Pathogens From Lung Biopsy Tissues by Metagenomic Next-Generation Sequencing [J]. Front Cell Infect Microbiol. 2018; 8205.
- G Xie, Zhao B, Wang X, et al. Exploring the Clinical Utility of Metagenomic Next-Generation Sequencing in the Diagnosis of Pulmonary Infection [J]. Infect Dis Ther. 2021; 10: 1419-1435.
- J Wang, Han Y, Feng J. Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis [J]. BMC Pulm Med. 2019; 19: 252.