
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Severe covid-19 infection caused rapid multiple pneumatoceles
development due to hyper inflammation and
accelerated pulmonary fibrosis
Muhamed Agbaria; Eli Karniel; Hadas Etel Sela; Lidiya Maor; Leonid Galin; Irit Kaye; Anna Shoychet; Dorin Baziv; Lior Grossman; Katia Muzzikovsky; Ahmad Balum; Gideon Charach; Lior Charach*
Department of Internal Medicine B, Meir Medical Center, Kfar Saba, Israel, affiliated with Sackler Medical School, Tel Aviv University, Tel Aviv, Israel.
*Corresponding Author : Lior Charach, MD
Department of Internal Medicine B, Meir Medical Center, Kfar Saba, Israel, affiliated with Sackler Medical School, Tel Aviv University, Tel Aviv, Israel.
Tel: +972 9 7472515; Fax: +972 3 5040538;
Email: drcharach@012.net.il
Received : Apr 10, 2023
Accepted : May 15, 2023
Published : May 22, 2023
Archived : www.jcimcr.org
Copyright : © Charach L (2023).
Abstract
A 70-year-old man was admitted to the internal medicine department complaining of productive cough for three days, severe dyspnea and desaturation with oxygen saturations of 87-89%. On arrival he was diagnosed with severe Covid 19 infection and started treatment with dexamethasone and remdesivir. Mechanical ventilation was installed 7 days after admission.Chest x-ray and chest CT scan issued 3 weeks after admission revealed several large pneumatoceles.
We describe the development of multiple pneumatoceles in severe Covid-19 infection with Adult Respiratory Distress Syndrome (ARDS).
Keywords: Pneumatocelle; ARDS; Covid-19; Pulmonary fibrosis.
Citation: Agbaria M, Karniel E, Sela HE, Maor L, Charach L, et al. Severe covid-19 infection caused rapid multiple pneumatoceles development due to hyper inflammation and accelerated pulmonary fibrosis. J Clin Images Med Case Rep. 2023; 4(5): 2423.
Introduction
There are few reports on Covid- 19 diseases describing pneumatocele development [1]. Pneumatoceles were found on X-ray and especially on the CT scan of the chest [2-4]. Covid -19 infection is associated with pneumonia, hyper inflammation process and accelerated fibrosis of the lungs, which is much more common than in other causes of pneumonias from other etiology [5]. Chemokines are elevated in COVID-19 and they stimulate development of lung fibrosis [6,7]. Due to rapid fibrosis –and because of stretched lung tissue, development of pneumatocele is not uncommon. The reasons for this might include the development of ischemic parenchymal damage lung fibrosis, low lung compliance, bronchiolar necrosis and inflammatory exudate in the airway [2-4,8,9]. Recent histological examinations reported bilateral diffuse alveolar destruction with cellular fibromyxoid exudates in COVID-19 [4,9].
Pneumatocele lesions may form as reaction to cellular fibro myxoidin filtrations, which form one way pass-like valve in the bronchus. Here we present a case of severe fibrosis and pneumatoceles development.
Case presentation
A 70-year-old man was admitted to ICU in the internal medicine department due to shortness of breath, productive cough for three days before admission and desaturation with of SpO2 of 89%. He was diagnosed as suffering from severe Covid 19 infection. His previous medical history was unremarkable with no history of prior medication use. Prominent sings on examinations were dyspnea with respiratory rates of 28 per minute, tachycardia 92 per minute, temperature-38.2, cyanosis, rale and crackles on auscultations in both lungs. Chest X-ray on arrival exhibitedpatchy opacifications in both lungs.
Blood test showed Hb-13, WBC-3400, 18% lymphocytes (lymphopenia). CRP was 14 (normal values < 0.5). Urea 55 Creatinine 1.3, additional blood work were unremarkable.
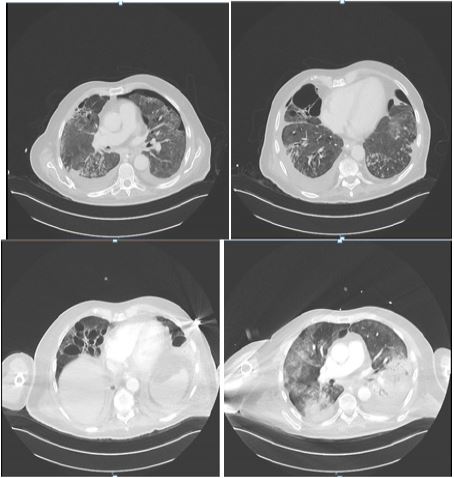
Treatment with Remdesivir and dexamethasone 6 mg Intravenous (IV) was initiated. The patient was treated with supplemental oxygen with improvement of SpO2 to 96%. Within the following 4 days the patients’ medical status improved with normalization of body temperature and cyanosis which disappeared. In addition, Respiratory rates decreased to 18 per minute. Laboratory tests showed improvement in CRP decreasing to a value of 10, however, the other blood work did not show any change. Although the patient exhibited partial improvement in medical status, 7 days after admission the patient developed severe respiratory distress and mechanical ventilation was initiated. On recurrent X ray there were more opacifications and large regions with lung fibrosis. CT scan of the lung (Figure 1) showed adult respiratory distress picture with several large (more than 5 cm in diameter) pneumatoceles. The patient continued the treatment with remdesivir for 10 days. Dexamethasone (IV) was continued and the dose was elevated. Blood cultures were negative however because of possibility of co-existing bacterial pneumonia treatment with ceftriaxone and azenil were added on the 11 day after admission. The patient state improved and deteriorated periodically. He was several times extubated and after several days intubated again because of respiratory instability.
He received several times different antibiotics including imipenemand piperacillin with tazobactam because of different bacteria –klebsiella pneumonia, pseudomonasaeroginosa in the patient’ssputum test.
Recurrent CT and X- ray showed severe aggravation in lung fibrosis and significant enlargement of several pneumatoceles with pneumothorax. The patient was referred for lung transplantation after stabilization of his condition.
It is important to emphasize that during 15 weeks of mechanical ventilation the patient lost 10% of his weight mostly due to muscle atrophy including diaphragm (measured by US). Although the patient received treatment of hyper alimentation (by nasogastric tube) blood analysis showed hypoalbuminemia of 1.5 mg /dl because of severe catabolic state. 16 weeks after admission the patient died.
Discussion
Searching the literature on Covid- 19 disease there are few reports describing pneumatocele development [1-4,8]. Pneumatoceles were found on X-ray and especially on the CT scan of the chest. Covid -19 infection is associated with pneumonia, hyper inflammation process and accelerated fibrosis of the lungs, which is much more common than in other causes of pneumonias from other etiology. Chemokines are elevated in COVID-19 and they stimulate development of lung fibrosis [1,2]. Due to rapid fibrosis –and because of stretched lung tissue, development of pneumatocele is not uncommon. The reasons for this might include the development of ischemic parenchymal damage lung fibrosis, low lung compliance, and inflammatory exudate in the airway [7-9].
Recent histological examinations reported bilateral diffuse alveolar destruction with cellular fibromyxoid exudates in COVID-19 [11]. Pneumatoceles lesions together with rapid lung fibrosis may critically reduce effective lung alveolar area and insufficient tissue oxygenation which leaded to inability of winning from mechanical ventilation, recurrent infections and lethality .
Current report presents an unusual Covid-19 course of the disease which started with a viral phase including clinical status of dyspnea, desaturation with SpO2 of 89% and fever which deteriorated to severe hyperinflammation state and ARDS indicating the need for mechanical ventilation. The established treatment by remdesivir and dexamethasone and later addition of antibiotics (according to various bacteria) didn’t cessate the process. Patient developed severe fibrosis of the lung with ruptures of the fibrotic tissue which caused pneumatoceles to development with critical reduction of the pulmonary alveolar net. All attempts to extubate the patient were unsuccessful. Another explanationis barotrauma in mechanically ventilated patients; however, the ventilation was done on low pressures. The frequency of barotrauma is 6.5 percent in non covid-19 patients [4] however in Covid -19 patients it seems to be more. The incidence of pneumatocelesand pneumothorax is10% according the studyof Shi H on 81 patients in Wuhan, China [8].
Conclusion
In conclusion, current report of Covid-19 describes severe respiratory distress which caused lung fibrosis, pneumatoceles and failure from of discontinue from mechanical ventilation.
Mechanical ventilation which is necessary, because of ARDS may be an additional reason by causing barotrauma for pneumatocele development in patients with Covid-19.
Declarations
Conflict of interest: None to declare.
Funding: This study was not funded.
References
- Joynt GM, Antonio GE, Lam P, et al. Late-stage adult respiratory distress syndrome caused by severe acute respiratory syndrome: abnormal findings at thin-section CT. Radiology. 2004; 230: 339–346.
- Desai SR. Acute respiratory distress syndrome: Imaging of the injured lung. Clin Radiol. 2002; 57: 8–17.
- Tagliabue M, Casella TC, Zincone GE, et al. CT and chest radiography in the evaluation of adult respiratory distress syndrome. Acta Radiol.1994; 35: 230–234.
- Liu K, Zeng Y, XIE Pye X, Xu G, Liu J, Wang H, et al. Covid -19 with cystic features on computer tomography: A case report. Medicine. 2020; 99: 2017.
- Chen G, Wu D, Guo W, Cao Y, Huang D, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J ClinInves. 2020; 130: 2620-2629.
- Khalil B, Elemam N, Maghazachi A . Chemokines and chemokine receptors during COVID-19 infection Computational and Structural Biotechnology Journal. 2021; 19: 976-988.
- Agostini C, Gurrieri C. Chemokine/cytokine cocktail in idiopathic pulmonary fibrosis. Proc Am Thorac Soc. 2006; 3: 357–363.
- Shi H, Han X, Jiang N, Yacun C, Ahvalid O, Gu J, Fant J, Zheng J, et al. Radiologic findings from 81 patients with Covid-19 infection in WUHAN, China: a descriptive study. Lancet Infect Dis. 2020; 20: 425-434.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020.