Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Rosette cataract
K Bouirig*; Y Saoiabi; O Cherkaoui
Ophthalmology Department “A”, Ibn Sina University Hospital (Hôpital des Spécialités), Mohammed V University, Rabat, Morocco.
*Corresponding Author : Kawtar Bouirig
Ophthalmology Department “A”, Ibn Sina University Hospital (Hôpital des Spécialités), Mohammed V University, Rabat, Morocco.
Email: bouirigkawtar@gmail.com
Received : Apr 24, 2023
Accepted : May 15, 2023
Published : May 22, 2023
Archived : www.jcimcr.org
Copyright : © Bouirig K (2023).
Citation: Bouirig K, Saoiabi Y, Cherkaoui O. Rosette cataract. J Clin Images Med Case Rep. 2023; 4(5): 2424.
Clinical image description
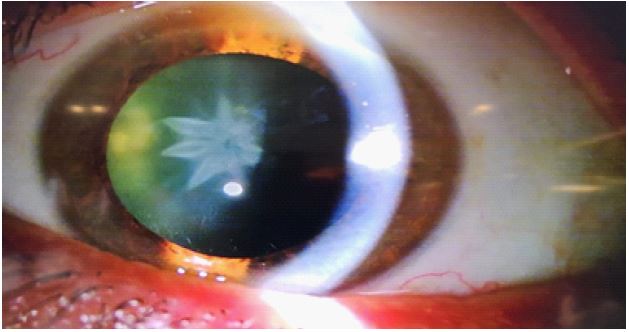
A 50-year-old man presented to our ophthalmology clinic with progressively diminishing vision in the left eye for 6 months. He had sustained a blunt trauma from a fist punch to the left side of his face, 6 months before. His best corrected visual acuity was 20/25 in the left eye and 20/20 in the right eye. The intraocular pressure was 15 mm Hg in both eyes. The slit lamp biomicroscopy of the left eye showed white axial opacities in the form of five distinct quadrangular ‘petals’, giving it a characteristic rosette pattern (Figures 1& 2).
The cataracts presenting with petaloid/rosette-shaped opacifications are typically seen in patients who have sustained blunt or penetrating physical trauma to the eye, and rarely due to electric shock, exposure to infrared energy or ionising radiation.
These opacifications may appear immediately after, or even up to few months after the trauma is inflicted. The opacities formed due to trauma may be stable or progressive. A thorough ocular examination in such cases is essential to ensure other ocular comorbidities, that is, rupture of globe, subluxation of lenses, choroidal detachment, angle recession glaucoma, retinal detachment, traumatic optic neuropathy, retrobulbar haemorrhage, and so on, are not missed.